Mixed aortic valve disease
|
|
|
- Clyde Bruce
- 5 years ago
- Views:
Transcription

1 Mixed aortic valve disease IOANNIS NTALAS MD, PhD Cardiologist, Clinical Fellow in Cardiovascular Imaging & Non-Invasive Cardiology, St Thomas Hospital School of Biomedical Engineering & Imaging Sciences King s College London, UK
2 No conflict of interest

3
4 Aortic stenosis Progresses faster in patients with degenerative disease than in those with a rheumatic or congenital aetiology. Wagner, S. & Selzer, A. Patterns of progression of aortic stenosis: a longitudinal hemodynamic study. Circulation 65, (1982). A higher degree of valvular calcification is independently associated with faster stenosis progression and worse outcome. Among symptomatic patients with medically treated moderate-tosevere aortic stenosis, mortality from the onset of symptoms is approximately 25% at 1 year and 50% at 2 years. Rosenhek, R. et al. Predictors of outcome in severe, asymptomatic aortic stenosis. N. Engl. J. Med. 343, (2000).
5 Aortic regurgitation Slow progression. Risk of developing symptoms or LV dysfunction <6.0% per year Weisenberg, D. et al. Mid-term echocardiographic progression of patients with moderate aortic regurgitation: implications for aortic valve surgery. J. Heart Valve Dis. 22, (2013)
6 Mixed aortic valve disease Clinical assessment
7

8 THE CLINICAL USE OF STRESS ECHOCARDIOGRAPHY IN NONISCHAEMIC HEART DISEASE: RECOMMENDATIONS FROM THE EΑCVI AND THE ASE (2016).
9
10
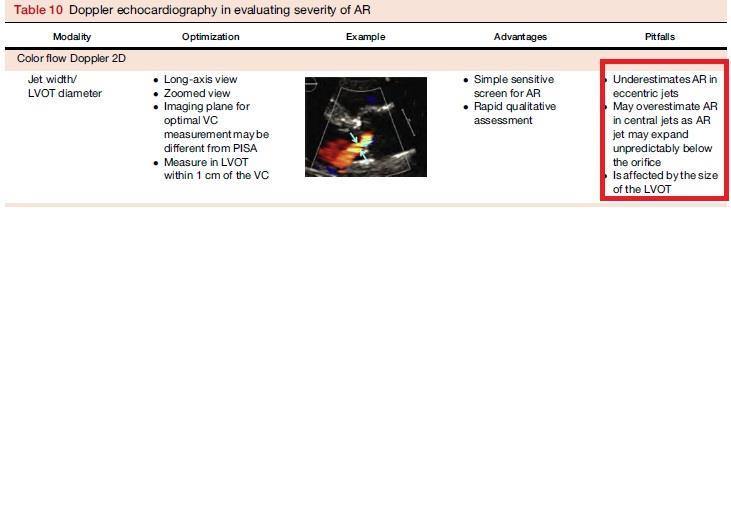
11 Deterioration 2NYHA classes 3% 28% 32% (p=0.006) Follow-up 3.3±1.7years
12 Systemic Hypertension in Low-Gradient Severe Aortic Stenosis With Preserved Ejection Fraction Circulation. MF. Eleid et al. Circulation 2013;128:


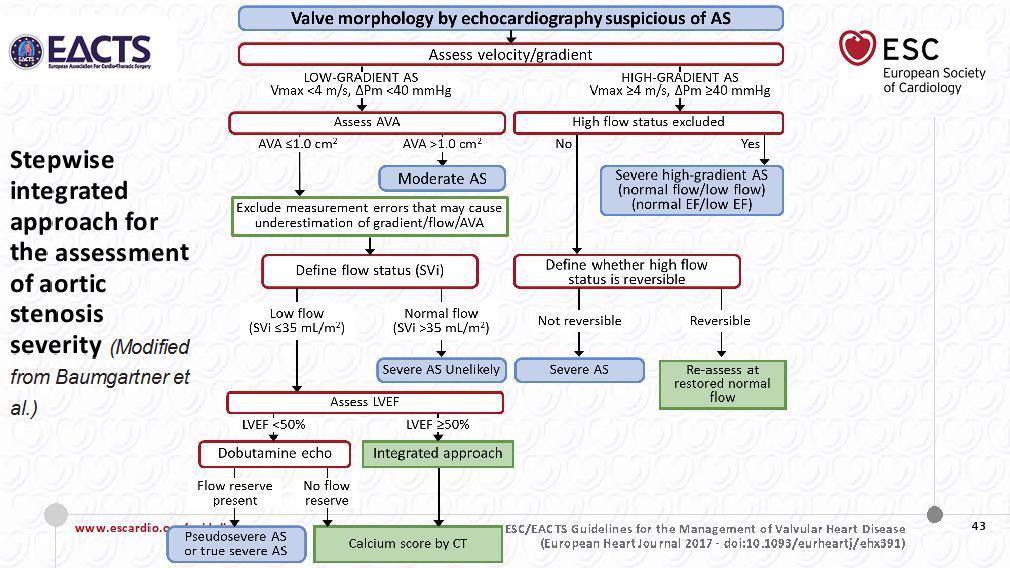
13 Low-Flow, Low-Gradient Aortic Stenosis With Normal and Depressed Left Ventricular Ejection Fraction Philippe Pibarot and Jean G. Dumesnil, JACC 60:19; 2012.
14

15 Conclusion: Among the many echocardiographic measures of longitudinal velocity and deformation, BLS has the strongest association with symptomatic status in aortic stenosis, and BLS < 13% is related to adverse outcomes in severe asymptomatic aortic stenosis.

16 Mechanisms of AR Boodhwani M.et al. Repair-oriented classification of aortic insufficiency: impact on surgical techniques and clinical outcomes. J Thorac Cardiovasc Surg 2009; 137:

17

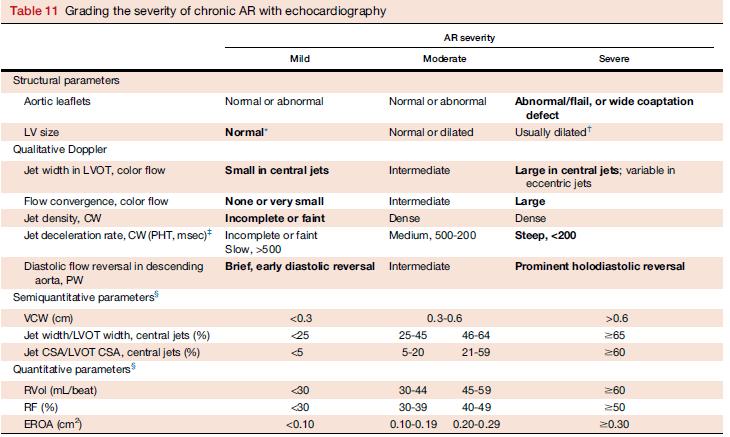
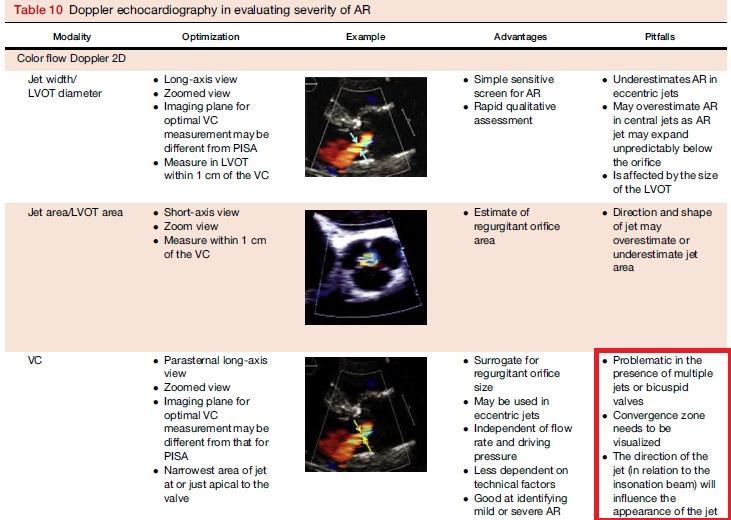
18 Density of regurgitant jet Perfectly central jets may appear denser than eccentric jets of higher severity

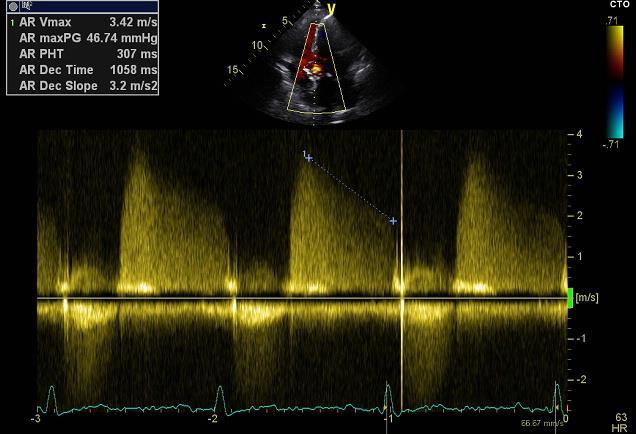
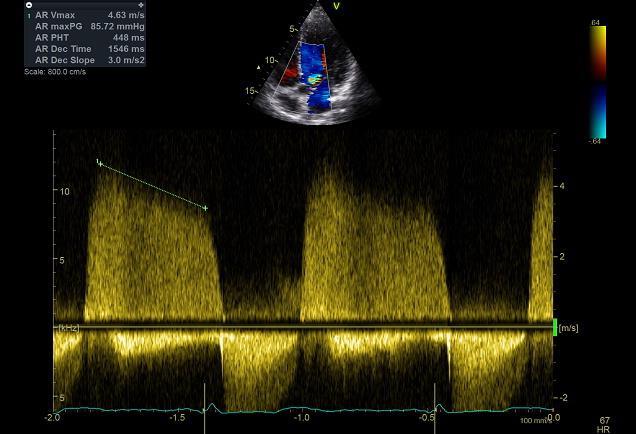
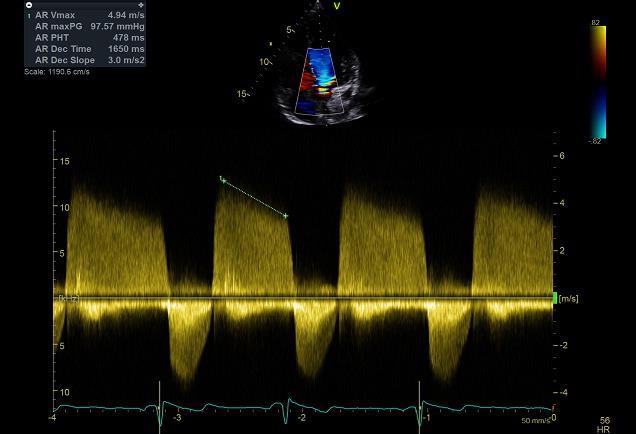
19 Jet deceleration rate (pressure halftime) Poor alignment of Doppler beam may result in lower pressure half-time Affected by changes that modify LV-aorta pressure gradient (if short, implies significant AR or high LV filling pressure- If long, excludes severe AR)

20 Flow reversal in the proximal descending aorta Depends on compliance of the aorta; less reliable in older patients Brief velocity reversal is normal Can be present in arteriovenous fistula in upper extremity, ruptured sinus of Valsalva May not be holodiastolic in acute AR
21
22
23
24

25 Neither exercise nor dobutamine SE can be used to regrade AR severity in a patient with symptoms, because the test-induced increase in heart rate shortens diastole, limiting quantification of AR severity.



26 Additional testing with TEE or CMR is indicated when -TTE is suboptimal in patients with suspected AR, -the mechanism for significant AR is not identified, -the echo/doppler parameters are discordant or inconclusive regarding the AR severity -the aortic root and ascending aorta need better assessment, or - a discrepancy is present between the TTE findings and the clinical setting.
27 Surgery-free survival by aortic regurgitant fraction. Saul G. Myerson et al. Circulation. 2012;126:
28 Main questions What is the fate of asymptomatic MAVD patients with preserved LV function? What is the optimal timing of surgical intervention in this population?
29

30
31

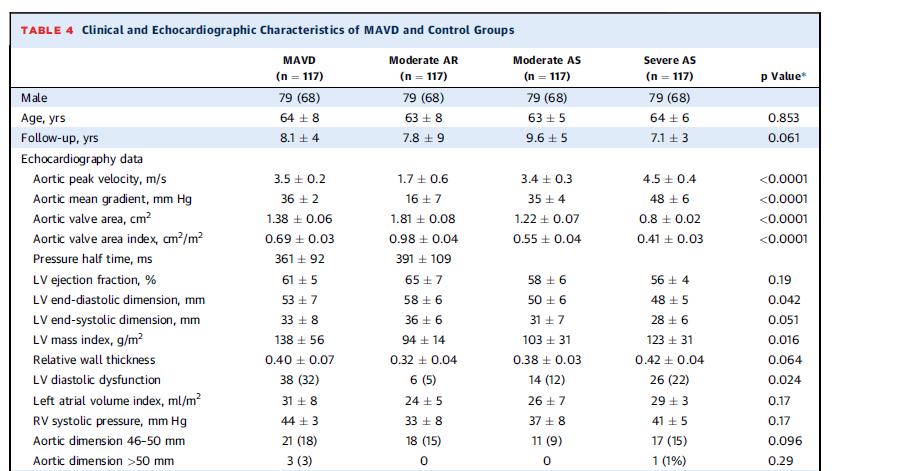
32 Αsymptomatic patients with moderate MAVD behaved similarly to asymptomatic patients with severe AS with regard to the development of symptoms and need for AVR, hence the need for vigilance in follow-up.

33
 or eccentric hypertrophy (RWT 0.")
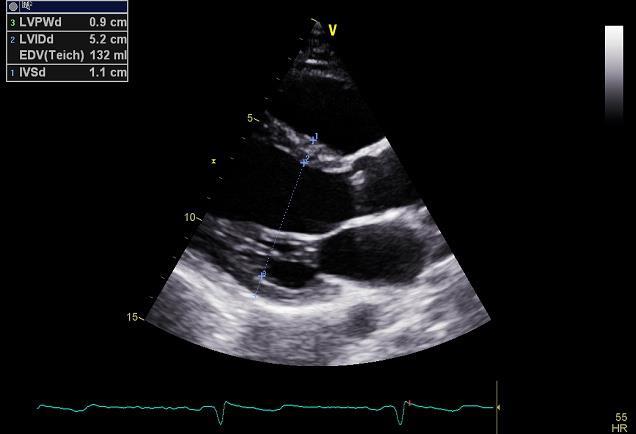
34 Relative wall thickness (RWT=2PWd/ LVEDD) allows further classification of LV mass increase as either concentric hypertrophy (RWT >0.42) or eccentric hypertrophy (RWT 0.42).
35
 A. Chieffo et al.")
36 Impact of Mixed Aortic Valve Stenosis on VARC-2 Outcomes and Postprocedural Aortic Regurgitation in Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the International Multicentric Study PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) A. Chieffo et al. Catheterization and Cardiovascular Interventions 86: (2015)
37 Impact of Mixed Aortic Valve Stenosis on VARC-2 Outcomes and Postprocedural Aortic Regurgitation in Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the International Multicentric Study PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) A. Chieffo et al. Catheterization and Cardiovascular Interventions 86: (2015)
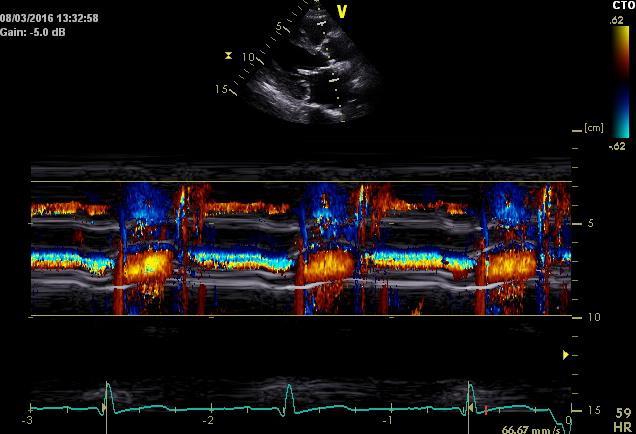
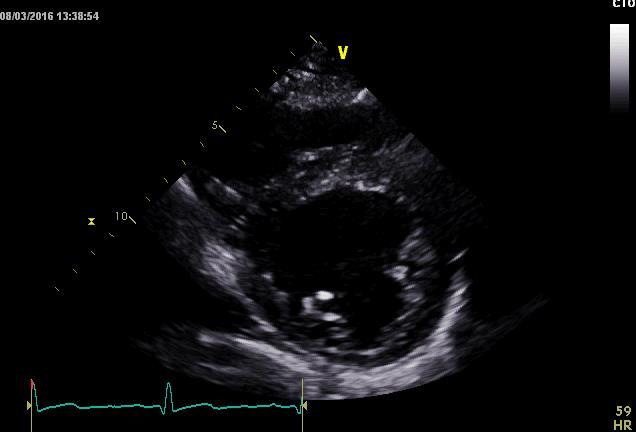
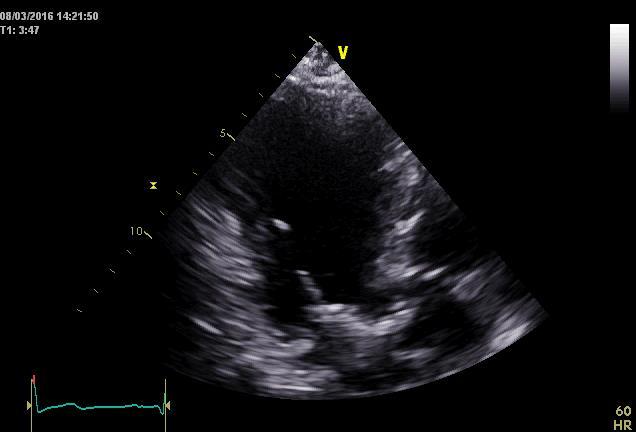
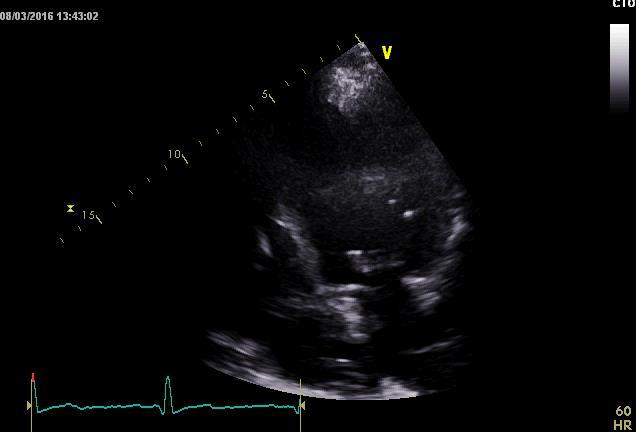
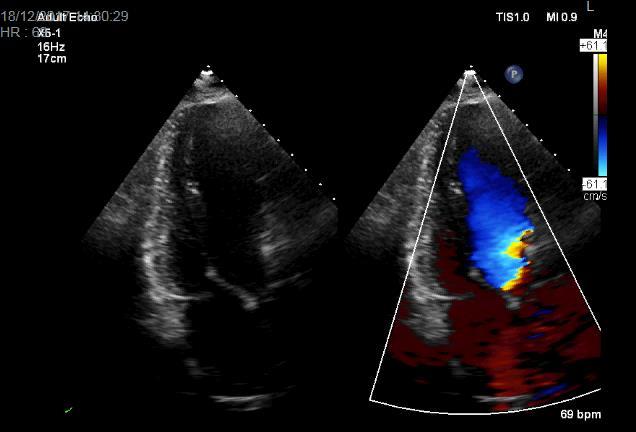
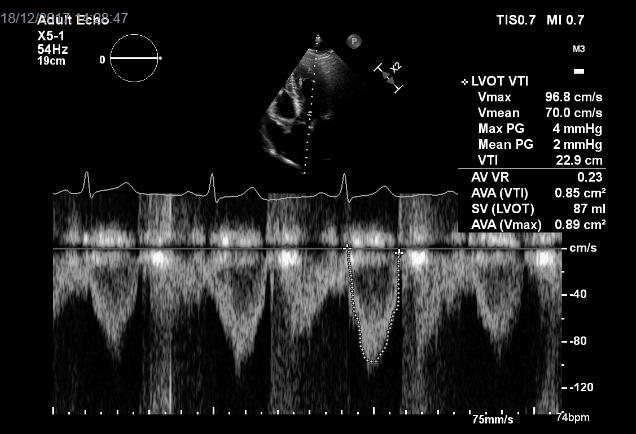
38 CASE No 1 75 year old man 1.62m, 62Kg (BSA 1.66m²) CABG 10 years ago (LIMA-LAD, SVG-RCA) ICD 7years ago Follow-up echocardiogram (3/2016)
39

40




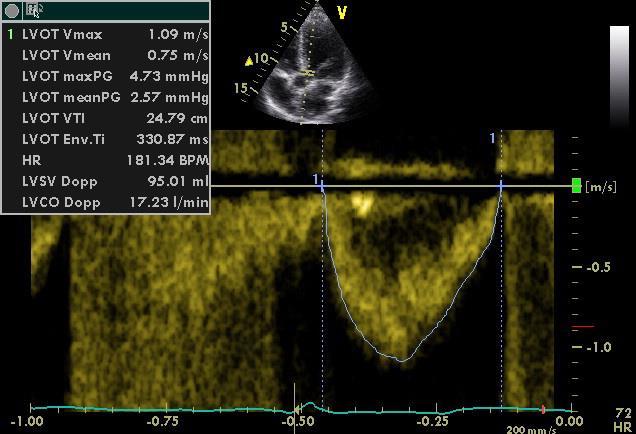
41 AVA:1.40 cm2, AVAi: 0.85 cm2/m2 DVI:0.40
42


43


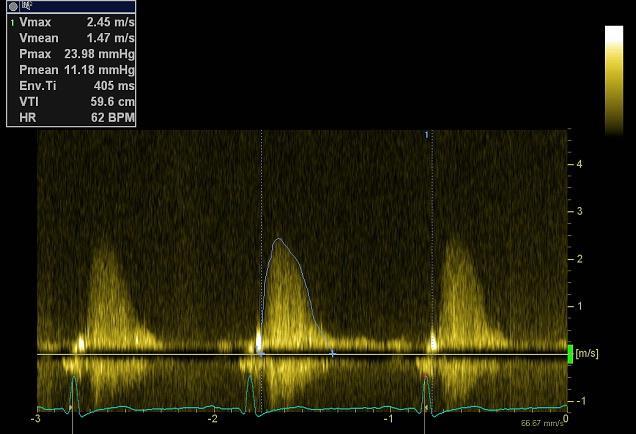
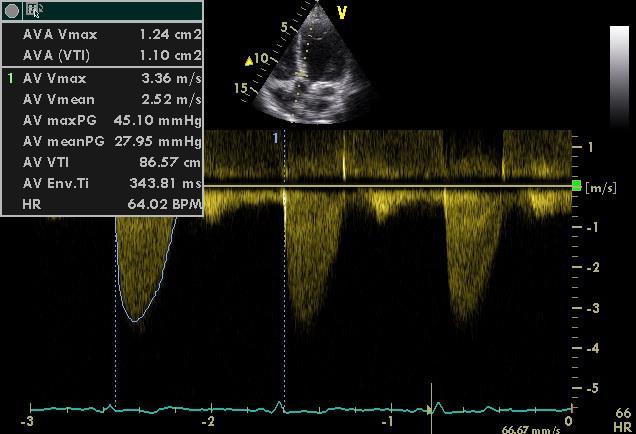
44 AVA: 0.72 cm2 AVAi:0.44cm2/m2 DVI: 0.21
45



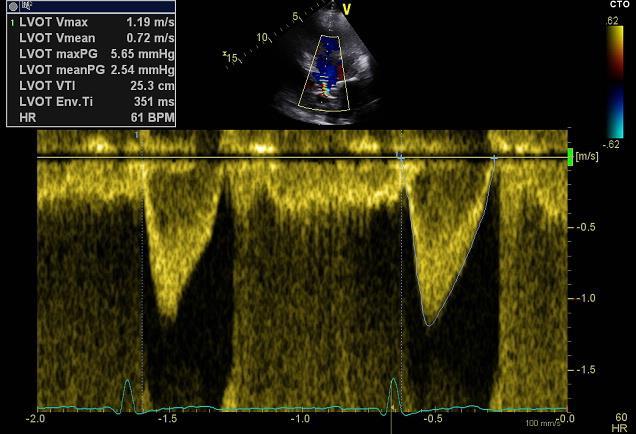
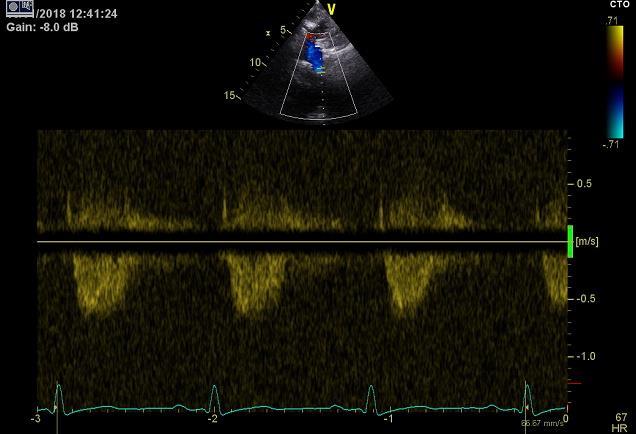
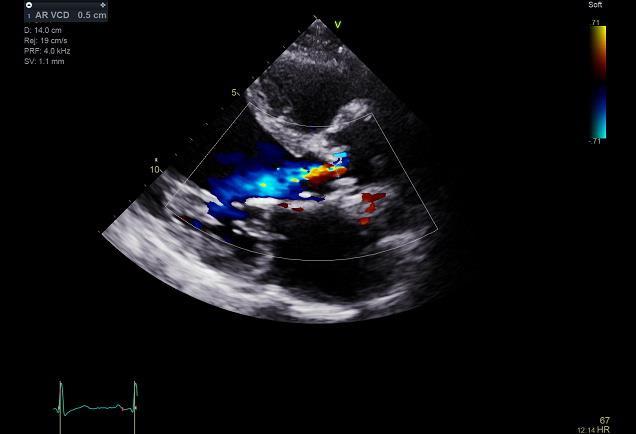
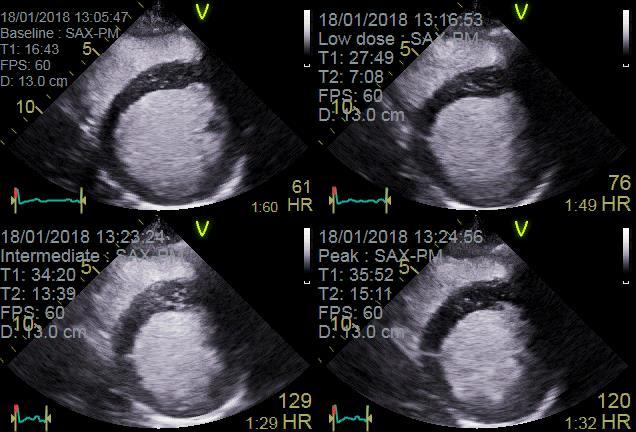
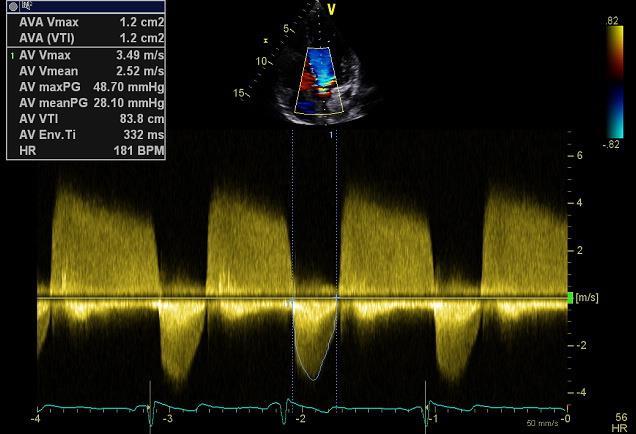
46 AVAproj= AVArest+(DAVA/DQ)x(250-Qrest)=1.03 cm2 Baseline: AV: Vmax=3.2m/sec, PG=41mmHg, MG=24.7mmHg, VTI=85.8 cm LVOT: Vmax=0.7m/sec, VTI=15cm DVI=0.17, AVA=0.61cm², AVAi=0.36 cm²/m², Stroke Volume=52ml Peak: AV: Vmax=3.3m/sec, PG=43mmHg, MG=26.6mmHg, VTI=48.4 cm LVOT: Vmax=1.0m/sec, VTI=19m DVI=0.39, AVA=1.36cm², AVAi=0.82cm²/m², Stroke Volume=66ml
47 Coronary Angiogram PCI SVG to RCA Patent LIMA to LAD. Learning Point: When a patient with HFrEF has a deterioration of symptoms and a decrease of AVA, pseudosevere AS (with AVAproj measurement) need to be excluded.
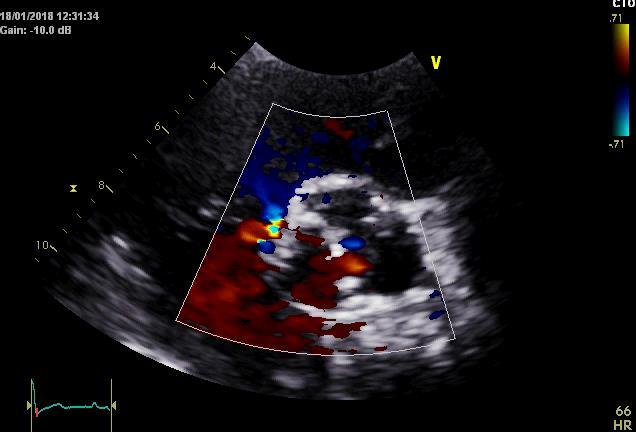
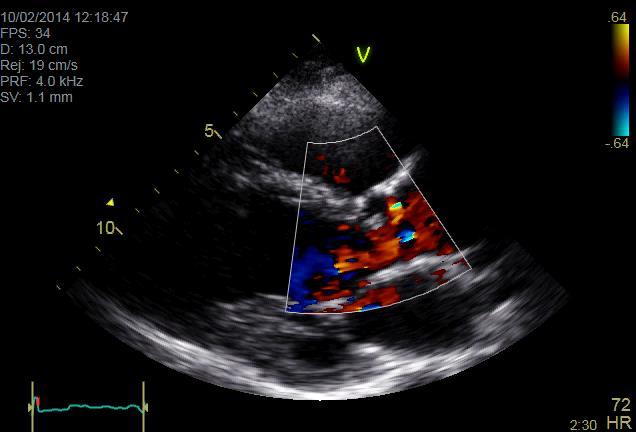
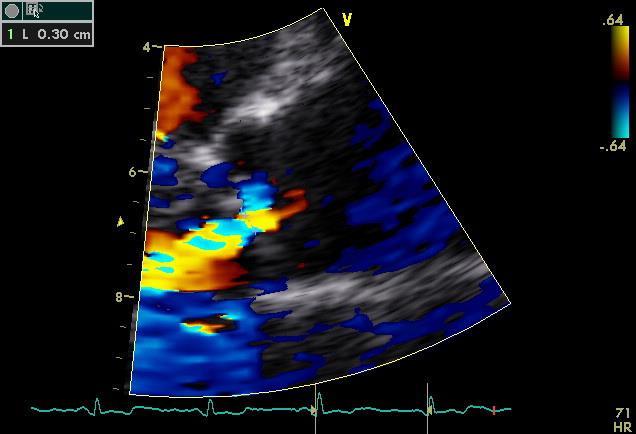
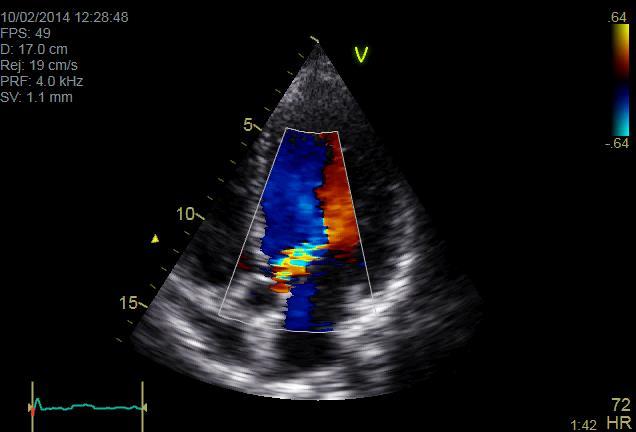
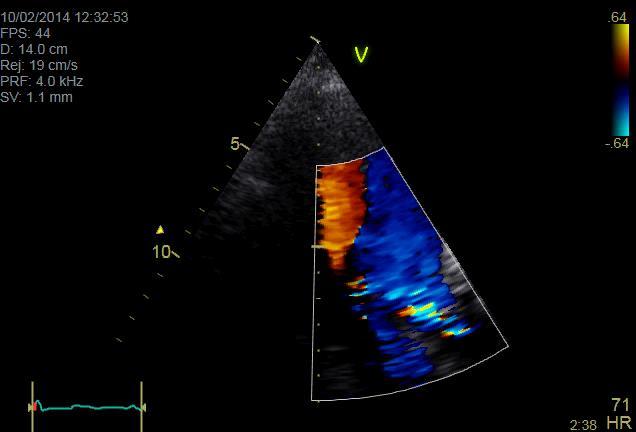
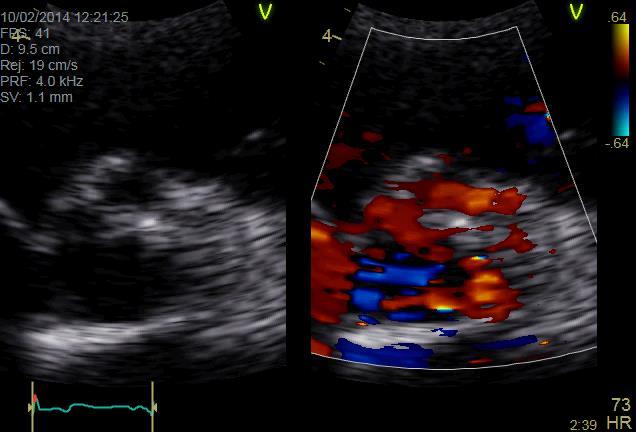
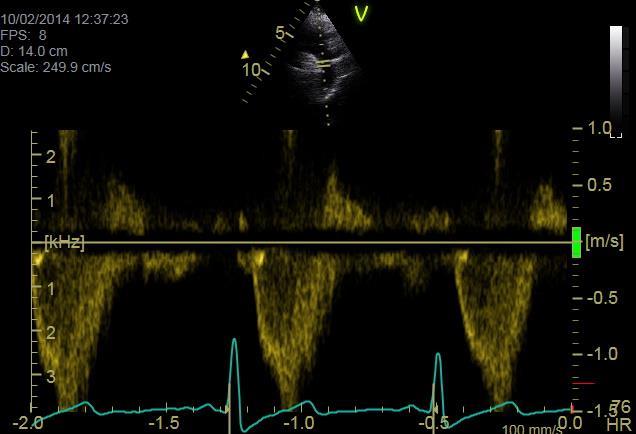
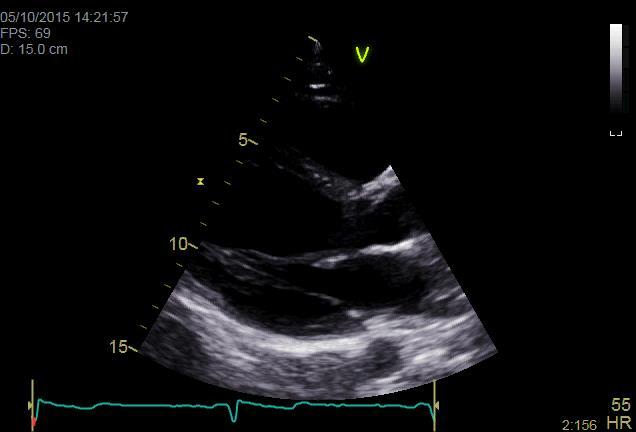
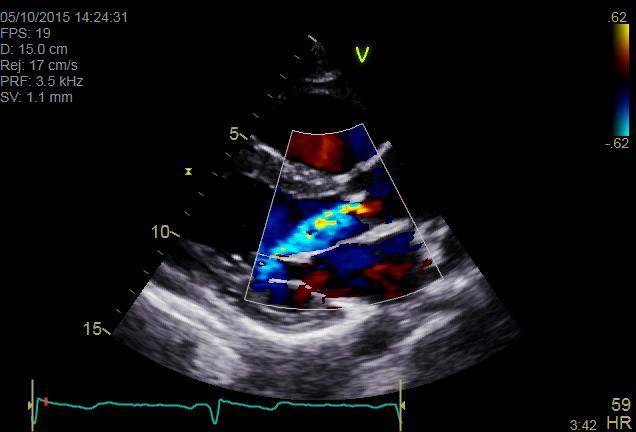
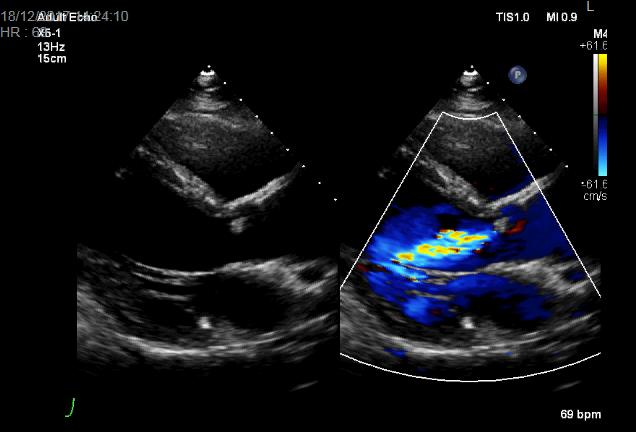
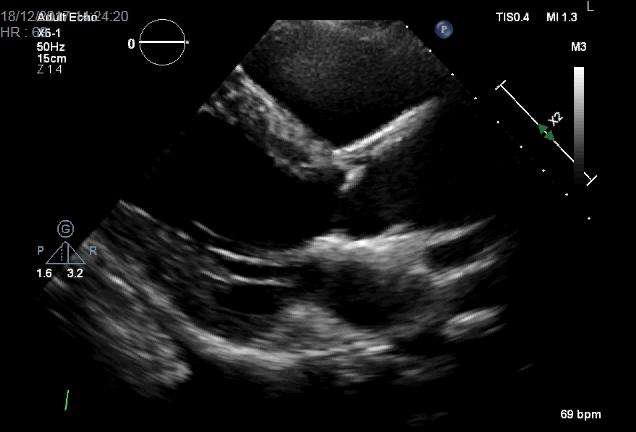
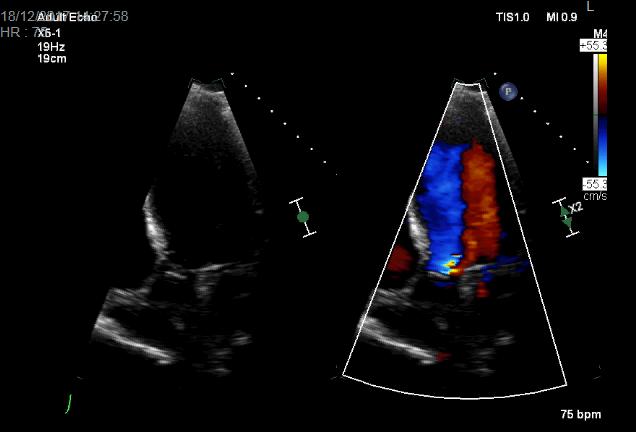
48 CASE No 2 27 year old woman 1.70 m, 72 Kg Her GP requested a TTE due to palpitations + systolic murmur-aortic position (2/2014)
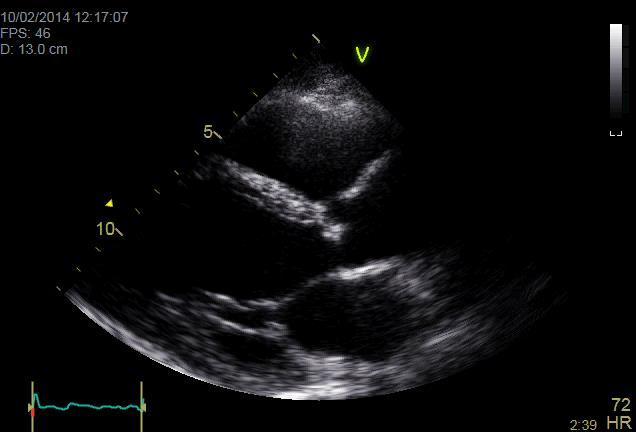

49
50
51
52
53
54
55

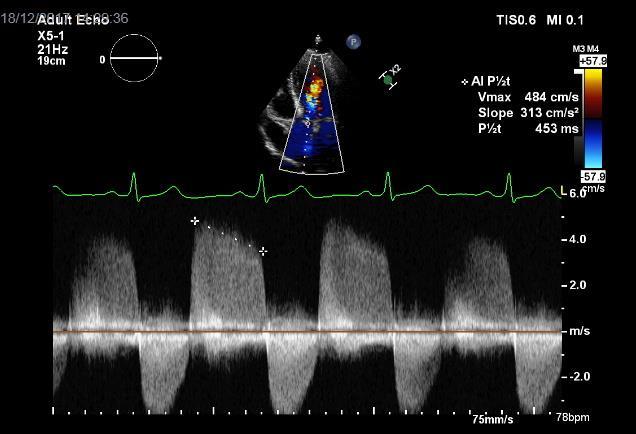
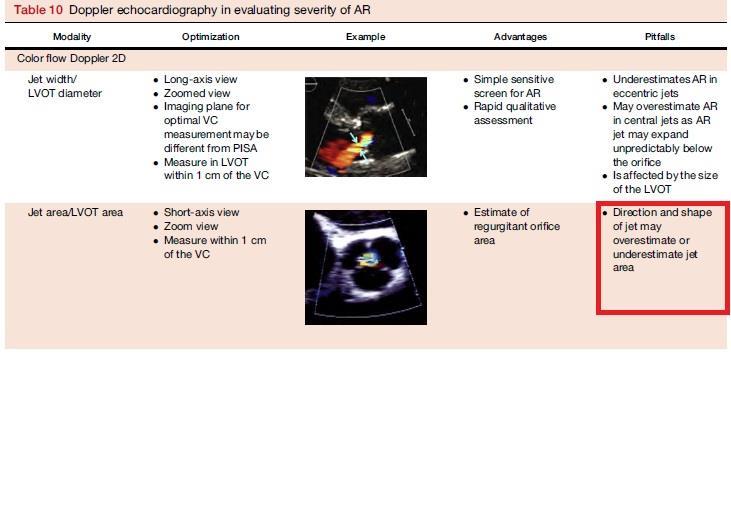
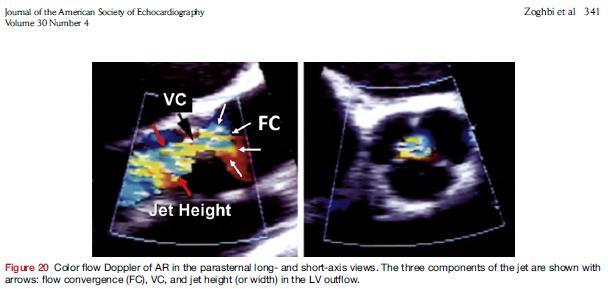
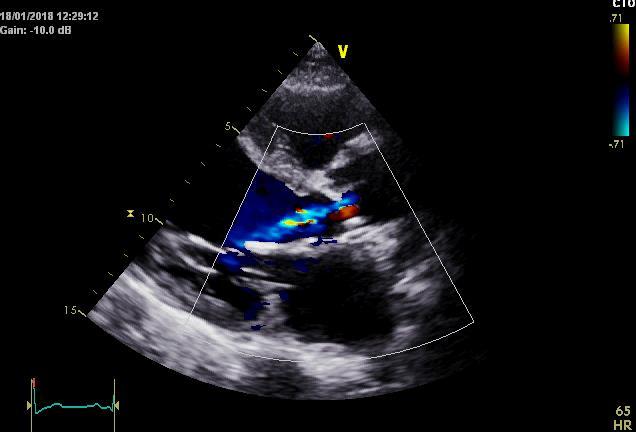
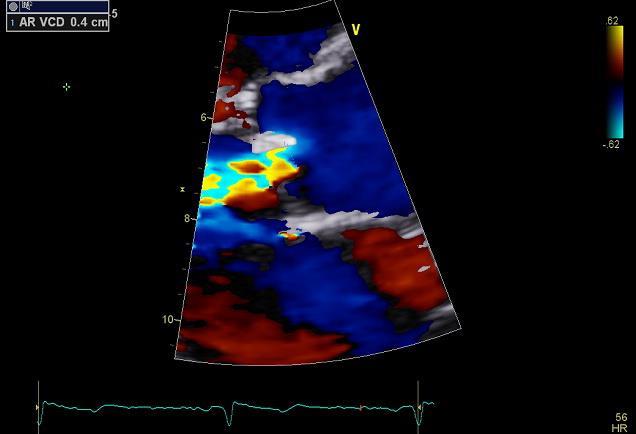
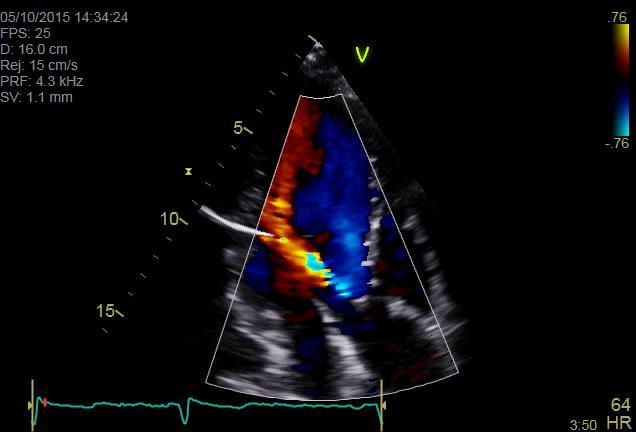
56 VC=0.6 cm Jet width/lvot diameter=45%

57 Εxercise ECG test


58
59
60 MDT Meeting 24/1/18 CTCA and potential candidate for Minimally Invasive Aortic Valve Replacement (mini-avr) Learning Point: Patients with moderate MAVD need to be followed every 6 to 12 months and monitored closely for rapid progression of valve disease or development of symptoms.
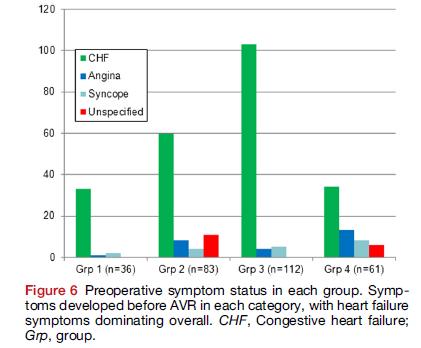
61 Almost 40% of the asymptomatic patients with moderate MAVD will become symptomatic and require AVR within 3 years from the time of diagnosis, similar to the patients with severe AS. TAKE HOME MESSAGES The combination of pressure and volume load in MAVD poses a unique haemodynamic stress on the LV different from that of isolated AS or AR. Αsymptomatic patients with moderate MAVD behaved similarly to asymptomatic patients with severe AS with regard to the development of symptoms and need for AVR.


62 Τhank you @DrNtalas
63
64
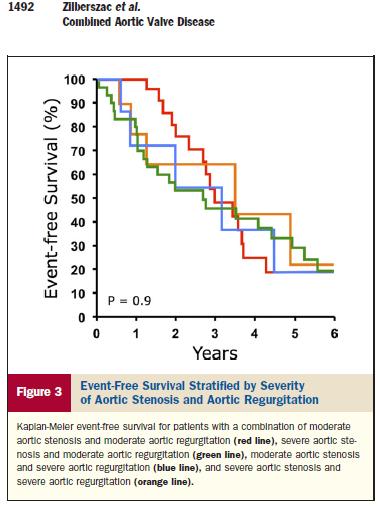
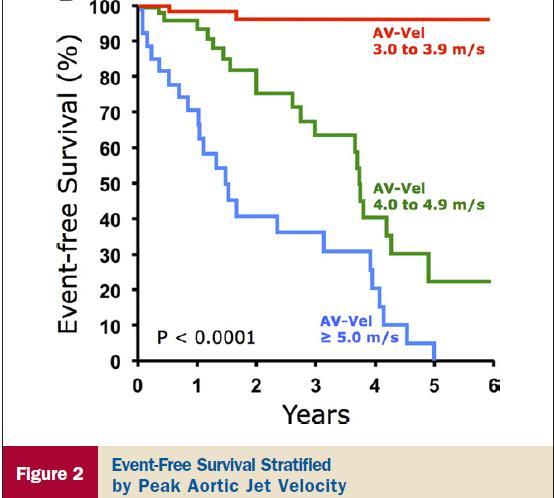
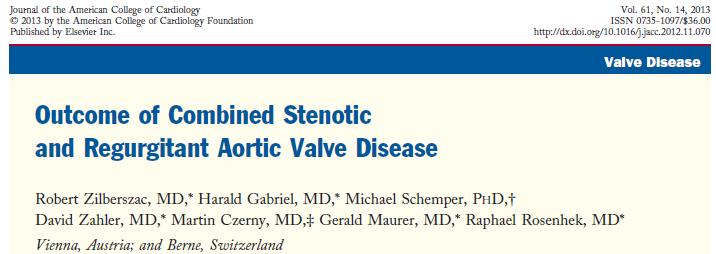
65 Conclusions: Asymptomatic patients with combined aortic valve disease can be safely followed until surgical criteria defined for AS, AR, or the aorta are reached. Good surgical and postoperative outcomes are achieved when following such a strategy. However, high event rates can be expected despite a relatively young age of the population and even in patients with moderate disease severity. AV-Vel, which reflects both stenosis and regurgitant severity, provides an objective and easily assessable parameter to risk stratify these patients
66 Conclusions -The AE outcomes in moderate MAVD appeared to be similar to those with asymptomatic isolated severe AS with preserved LV systolic function. This suggests that it would be inappropriate to apply guideline recommendations for isolated moderate AS or moderate AR to this population. -11% of moderate MAVD patients with concentric hypertrophy can become symptomatic even in the absence of severe aortic valve disease. -Patients with moderate MAVD be followed every 6 to 12 months and monitored closely for rapid progression of valve disease or development of symptoms, similar to patients with isolated severe AS. -Early valve replacement may be considered for MAVD patients without comorbidities in centers with low risk for such procedures.
 A. Chieffo et al.")
67 Impact of Mixed Aortic Valve Stenosis on VARC-2 Outcomes and Postprocedural Aortic Regurgitation in Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the International Multicentric Study PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) A. Chieffo et al. Catheterization and Cardiovascular Interventions 86: (2015)
68 Outcome of Patients with Mixed Aortic Valve Disease Undergoing Transfemoral Aortic Valve Replacement J. Seeger et al. Structural Heart, 2017; 1:3-4, Mixed aortic valve disease was defined as coexisting severe AS and moderate or severe AR. There was no significant difference in procedural results in the propensity matched population.

69 Conclusion TAVR in patients with mixed aortic valve disease is associated with comparable 30 days, 12- and 24-month clinical outcome compared to patients undergoing TAVR for severe aortic stenosis.
70

71
72
 A. Chieffo et al.")
73 Impact of Mixed Aortic Valve Stenosis on VARC-2 Outcomes and Postprocedural Aortic Regurgitation in Patients Undergoing Transcatheter Aortic Valve Implantation: Results From the International Multicentric Study PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) A. Chieffo et al. Catheterization and Cardiovascular Interventions 86: (2015)
74 Conclusion: MAS was associated with lower device success. However, despite these findings, it had no influence on long-term postoperative outcomes.
75
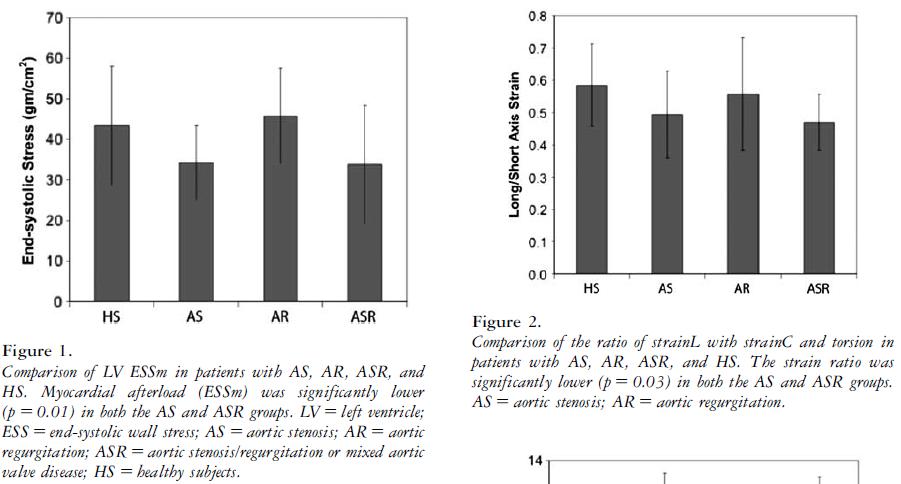
76 End-systolic circumferential midwall stress (ESWS) was calculated from Mirsky's variation of the LaPlace relationship as it pertains to the left ventricle Stress= P*b h h (1 2b where p = pressure measured at the dicrotic notch of the aortic pressure tracing, h = wall thickness, a = midwall semi-major axis (L2 + h ) at end-systole and b = midwall semi-minor axis (-D + -b-) at end-systole. The result obtained by this formula was converted to dyn X 103/cm2 by multiplying by a conversion factor of 1332 dyn/cm2/mm Hg. Wall thickness was obtained using the method of Hugenholtz et al.
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY?
 HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
HOW IMPORTANT ARE THESE ECHO MEASUREMENTS ANYWAY? John D. Carroll, MD Professor, Director of Interventional Cardiology and Co-Medical Director of the Cardiac and Vascular Center, University of Colorado
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Managing the Low Output Low Gradient Aortic Stenosis Patient
 Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Managing the Low Output Low Gradient Aortic Stenosis Patient R A Nishimura MD Judd and Mary Leighton Professor of CV Mayo Clinic No disclosures Valvular Stenosis Severity of Aortic Stenosis Mean gradient
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis
 TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
TEE guided TAVR using BASILICA technique in patient with stenotic Freestyle aortic bioprosthesis Zuyue Wang MD Associate professor, Georgetown University School of Medicine MedStar Heart and Vascular Institute
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
DISCLOSURE. Relevant Financial Relationship(s) Off Label Usage. None. None
 Off Label Usage. None. None") Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
Echo for TAVR Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director, Cardiology Fellowship Mayo
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
Comments restricted to Sapien and Corevalve 9/12/2016. Disclosures: Core Lab contracts with Edwards Lifesciences, Middlepeak, Medtronic
 Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Para-ValvularRegurgitation post TAVR: Predict, Prevent, Quantitate, Manage Linda D. Gillam, MD, MPH, FACC, FASE Chair, Department of Cardiovascular Medicine Morristown Medical Center/Atlantic Health System
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
22/06/2017. Oxford City. Transcatheter aortic valve replacement 2017 guidelines. 1. First time I have heard about it. 2.
 Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Oxford City Transcatheter aortic valve replacement 2017 guidelines Monday 19 th June Jim Newton Oxford Oxford University Hospitals NHS FT How familiar are you with TAVR? 1. First time I have heard about
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Aortic stenosis aetiology: morphology of calcific AS,
 How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
How to improve patient selection in aortic stenosis? Fausto J. Pinto, FESC Aortic stenosis aetiology: morphology of calcific AS, bicuspid valve, and rheumatic AS (Adapted from C. Otto, Principles of
Welcome 17 Michigan TAVR Participating Hospitals!
 Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Welcome 17 Michigan TAVR Participating Hospitals! 1 MICHIGAN TAVR BRIEF OVERVIEW HOW AND WHY PRE-TAVR IMAGING EVALUATION AND THE TVT Michael Grossman, MD Co-Director, BMC2 Coordinating Center Why Michigan
Imaging in TAVI. Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013
 Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
Imaging in TAVI Jeroen J Bax Dept of Cardiology Leiden Univ Medical Center The Netherlands Davos, feb 2013 Research grants: Medtronic, Biotronik, Boston Scientific, St Jude, BMS imaging, GE Healthcare,
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter
 Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Options for my no option Patients Treating Heart Conditions Via a Tiny Catheter Nirat Beohar, MD Associate Professor of Medicine Director Cardiac Catheterization Laboratory, Medical Director Structural
Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S.
 CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
CORONARY ARTERY REVASCULARIZATION WITH MILD AORTIC STENOSIS: STRATEGIES OF TREATMENT 9 th ANNUAL MEETING OF THE EAB SOCIETY, Pravets, Bulgaria, 2012 Sotirios N. Prapas, M.D., Ph.D, F.E.C.T.S. Director
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data
 Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Transcatheter Aortic Valve Replacement: Current and Future Devices: How do They Work, Eligibility, Review of Data Echo Florida 2013 Jonathan J. Passeri, M.D. Co-Director, Heart Valve Program Director,
Low gradient severe aortic stenosis with preserved left ventricular ejection fraction
 Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Review Article Low gradient severe aortic stenosis with preserved left ventricular ejection fraction Alper Ozkan Heart and Vascular Institute, Cleveland Clinic, Cleveland, Ohio, USA Corresponding to: Alper
Hypertension in Aortic Valve Disease
 Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Hypertension in Aortic Valve Disease Hanna M. Nosseir MRCP, FRCP Head of Cardiology department Galaa Military Medical Complex Aortic stenosis: Introduction Arterial hypertension and aortic stenosis are
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
2019 Qualified Clinical Data Registry (QCDR) Performance Measures
 Performance Measures") 2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
2019 Qualified Clinical Data Registry (QCDR) Performance Measures Description: This document contains the 18 performance measures approved by CMS for inclusion in the 2019 Qualified Clinical Data Registry
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
TAVR : Caring for your patients before and after TAVR
 TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
TAVR : Caring for your patients before and after TAVR Zubair Ahmed MD FSCAI Interventional Cardiologist Washington Regional Medical Center / Walker Heart Institute What is Aortic Valve Stenosis? AVA ~4
Severity of AS Degree of AV calcification (? Bicuspid AV), annulus size, & aortic root
, annulus size, & aortic root") The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
The role of Cardiac Imaging modalities in evaluation & selection of patients for Trans-catheter Aortic Valve Implantation Dr.Saeed AL Ahmari Consultant Cardiologist Prince Sultan Cardaic Center, Riyadh
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC
 CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC Background Aortic stenosis is the commonest form of valvular heart disease in the UK Asymptomatic patients with mild AS make up a significant
CARDIAC PHYSIOLOGIST LED AORTIC STENOSIS SURVEILLANCE CLINIC Background Aortic stenosis is the commonest form of valvular heart disease in the UK Asymptomatic patients with mild AS make up a significant
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Nothing to Disclose. Questions. Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Paul Wood at the Nathanson Lecture, 1958
 Should One Intervene? Paul Wood at the Nathanson Lecture, 1958") Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
Disclosure Asymptomatic Severe Aortic Stenosis: (When) Should One Intervene? Nothing to Disclose Gabriel Gregoratos, MD, FACC, FAHA Questions Can one improve globally on the asymptomatic state? and if
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece
 A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
A patient with aortic stenosis and LV dysfunction EuroECHO & Other Imaging Modalities 2012 Athens, Greece Jean-Luc MONIN, MD, PhD. University Hospital, Créteil, FRANCE My disclosures: Lecture and/ or consulting
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens
 MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
MITRAL REGURGITATION IN PATIENT WITH SEVERE AORTIC VALVE STENOSIS Ioannis Alexanian, MD, PhD Department of Cardiology General Hospital of Chest Diseases Sotiria Athens I HAVE NOTHING TO DECLARE Management
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
A Health Care Professional s Guide Aortic Stenosis in Seniors
 A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
A Health Care Professional s Guide Aortic Stenosis in Seniors With highlights from the 2014 ACC/AHA practice guidelines for valve disease Aortic stenosis (AS) is primarily caused by calcification of the
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
 Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
Stress Echocardiography: Illustrative Cases Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate Director,
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Aortic Stenosis: UPDATE Anjan Sinha, MD Krannert Institute of Cardiology
 Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Aortic Stenosis: UPDATE 2010 Anjan Sinha, MD Krannert Institute of Cardiology None Disclosures 67-Year-Old Male Dyspnea and angina Class III heart failure No PND or orthopnea 3/6 late peak SEM Diminished
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation
 Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Incidence And Predictors Of Left Bundle Branch Block After Transcatheter Aortic Valve Implantation Ömer Aktug 1, MD; Guido Dohmen 2, MD; Kathrin Brehmer 1, MD; Verena Deserno 1 ; Ralf Herpertz 1 ; Rüdiger
Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών Σ.Ράμμος
 ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Improving Quality of Care for Patients with Heart Valve Disease
 Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Improving Quality of Care for Patients with Heart Valve Disease The Heart Team The Heart Valve Clinic Raphael Rosenhek Department of Cardiology Medical University of Vienna Eurovalve 2016 Brussels, March
Policy #: 222 Latest Review Date: March 2009
 Name of Policy: MRI Phase-Contrast Flow Measurement Policy #: 222 Latest Review Date: March 2009 Category: Radiology Policy Grade: Active Policy but no longer scheduled for regular literature reviews and
Name of Policy: MRI Phase-Contrast Flow Measurement Policy #: 222 Latest Review Date: March 2009 Category: Radiology Policy Grade: Active Policy but no longer scheduled for regular literature reviews and
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
TGA atrial vs arterial switch what do we need to look for and how to react
 TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
TGA atrial vs arterial switch what do we need to look for and how to react Folkert Meijboom, MD, PhD, FES Dept ardiology University Medical entre Utrecht The Netherlands TGA + atrial switch: Follow-up
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Aortic stenosis (AS) is common with the aging population.
 is common with the aging population.") New Insights Into the Progression of Aortic Stenosis Implications for Secondary Prevention Sanjeev Palta, MD; Anita M. Pai, MD; Kanwaljit S. Gill, MD; Ramdas G. Pai, MD Background The risk factors affecting
New Insights Into the Progression of Aortic Stenosis Implications for Secondary Prevention Sanjeev Palta, MD; Anita M. Pai, MD; Kanwaljit S. Gill, MD; Ramdas G. Pai, MD Background The risk factors affecting
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes
 Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Australia and New Zealand Source Registry Edwards Sapien Aortic Valve 30 day Outcomes A/ Professor Darren Walters On behalf of the ANZ Source Investigators Director of Cardiology Brisbane, Australia ANZ
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014
 Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Indications of Coronary Angiography Dr. Shaheer K. George, M.D Faculty of Medicine, Mansoura University 2014 Indications for cardiac catheterization Before a decision to perform an invasive procedure such
Asymptomatic Valvular Disease:
 Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Asymptomatic Valvular Disease: Can Echocardiography Help You Decide When to Intervene? Neil J. Weissman, MD MedStar Health Research Inst at MedStar Washington Hospital Center & Professor of Medicine Georgetown
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Edwards Sapien. Medtronic CoreValve. Inoperable FDA approved High risk: in trials. FDA approved
 Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Transcatheter Aortic Valve Replacement Symptomatic Aortic Stenosis Asymptomatic Juan Crestanello, MD Interim Director, Division of Cardiac Surgery Associate Professor Division of Cardiac Surgery The Ohio
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut