TCD IN THE NICU, PICU AND OTHER APPLICATIONS. Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
|
|
|
- Annabel Boyd
- 5 years ago
- Views:
Transcription


1 TCD IN THE NICU, PICU AND OTHER APPLICATIONS Dorothy Bulas M.D. Professor of Pediatrics & Radiology Children s National Washington D.C.
2 Objectives Recognize normal and abnormal cranial blood flow patterns Identify applications for TCD in the critical ill child

3 Transcranial Doppler (TCD) Alterations in blood flow following asphyxia trauma subarachnoid hemorrhage Clinical indications include Vasospasm - Hydrocephalus ICP - Vasculitis Sickle Cell - Brain death
4 Factors impacting intracranial flow: Arterial narrowing: Vasospasm, stenosis Occlusion: proximal, local Head injury Changes in CO2: sleeping, crying Age: flow velocity decreases with age
5 Protocols and Technique are Specific to Type of Examination: What is the clinical question? What are the presenting symptoms? Do other vascular studies provide info? Baseline exam for reference? Bedside, OR, ICU, ER or vascular lab? Which instrument provides the best data for this exam? Experienced examiner?

6 Neonatal Technique- Open Fontanelle

7 Neonatal technique Open Fontanelle



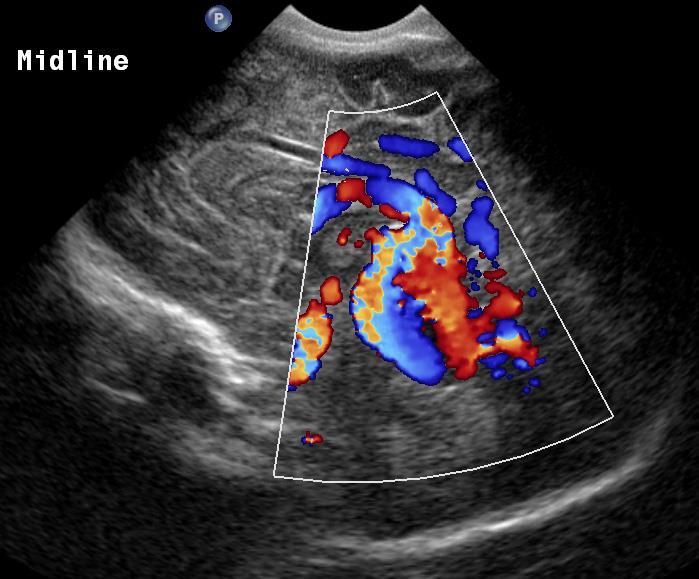
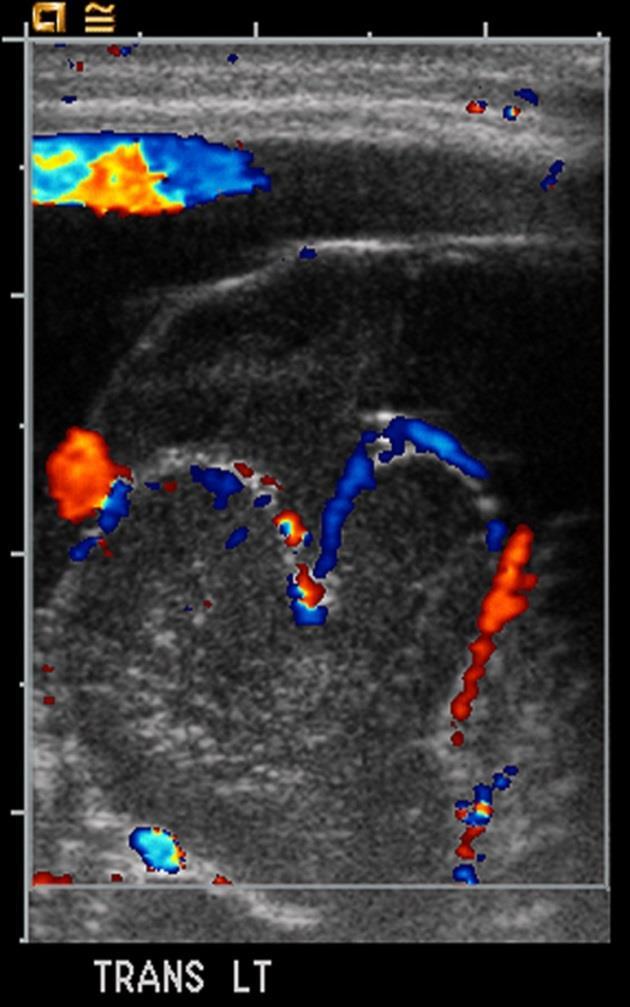
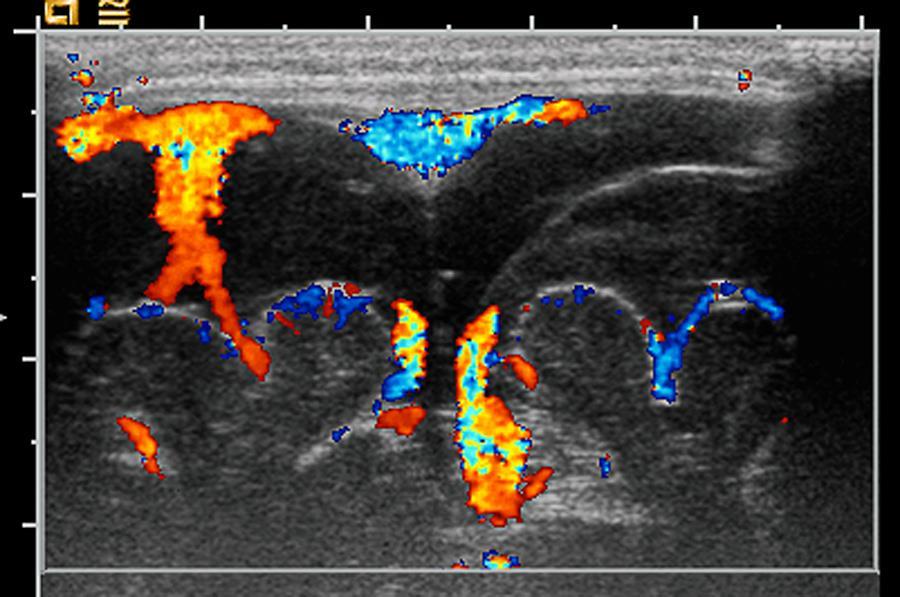
8 Vein of Galen Aneurysm Feeding vessels, nidus and draining veins b c c


9 Normal venous sinuses Vein of Galen a Superior sagittal sinus b

10

11

12 Beware!

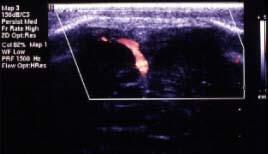
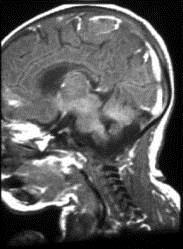
13 Dural sinus fistula
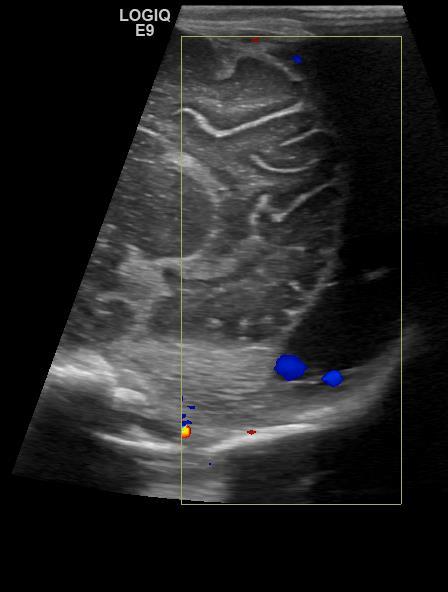
14 Extra-Axial Collections



15 Subdural hematoma a Nonaccidental trauma - no crossing vessels, compressed, flat gyri. b

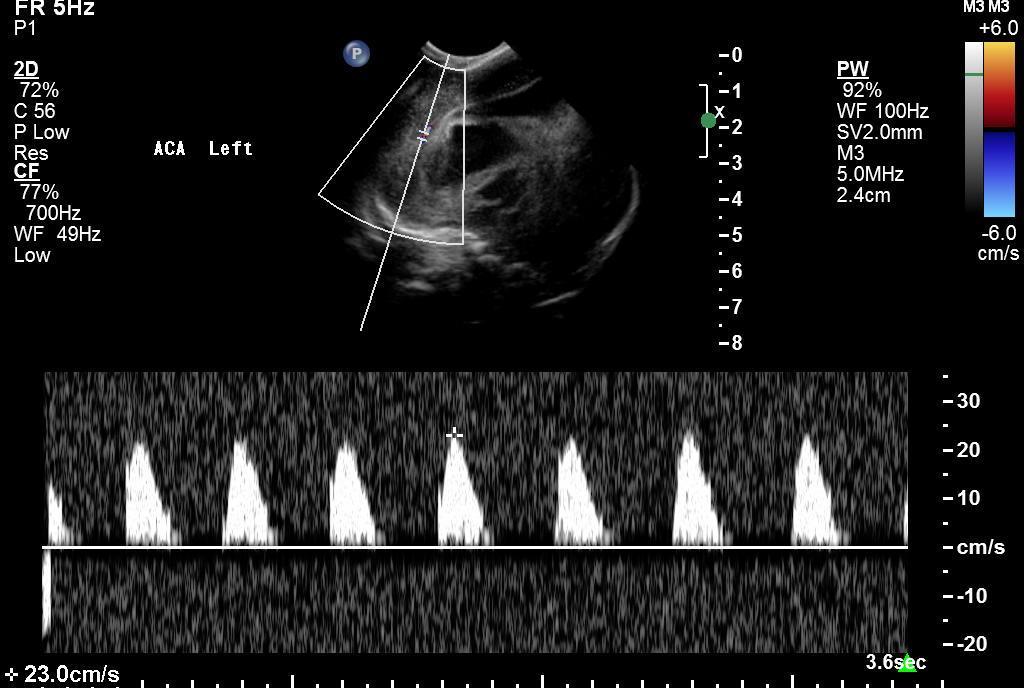
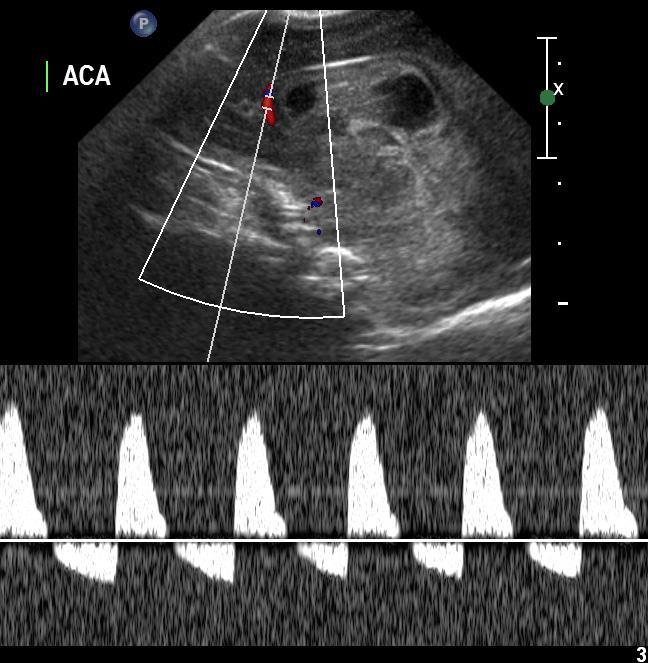
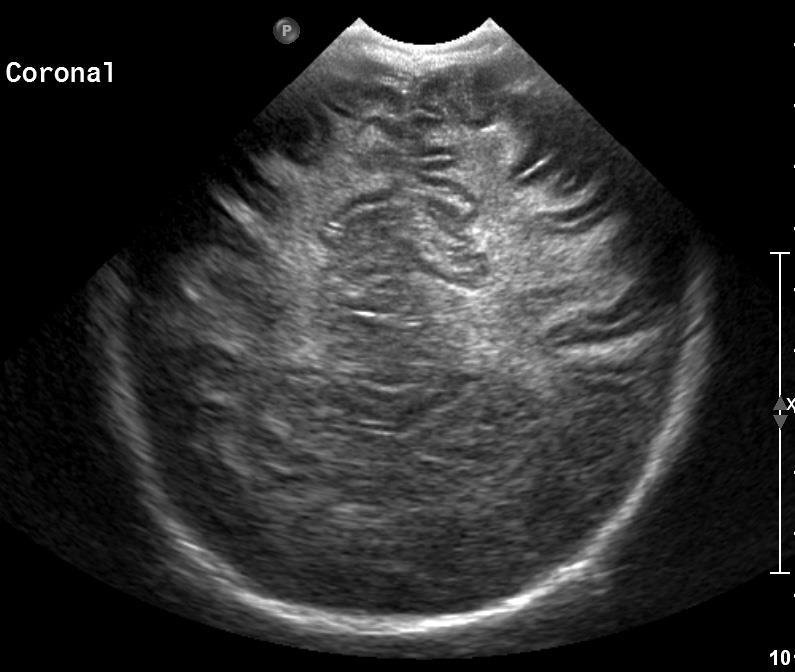
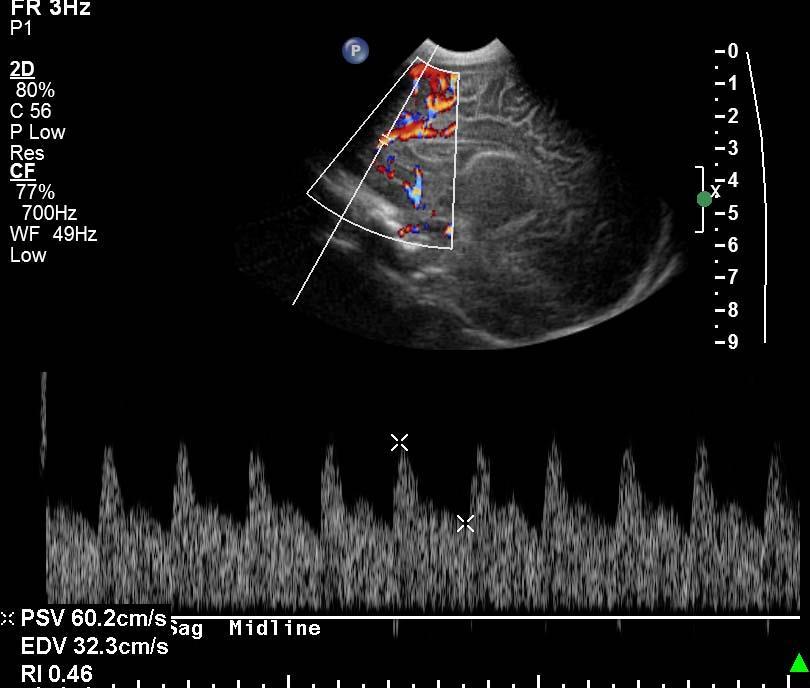
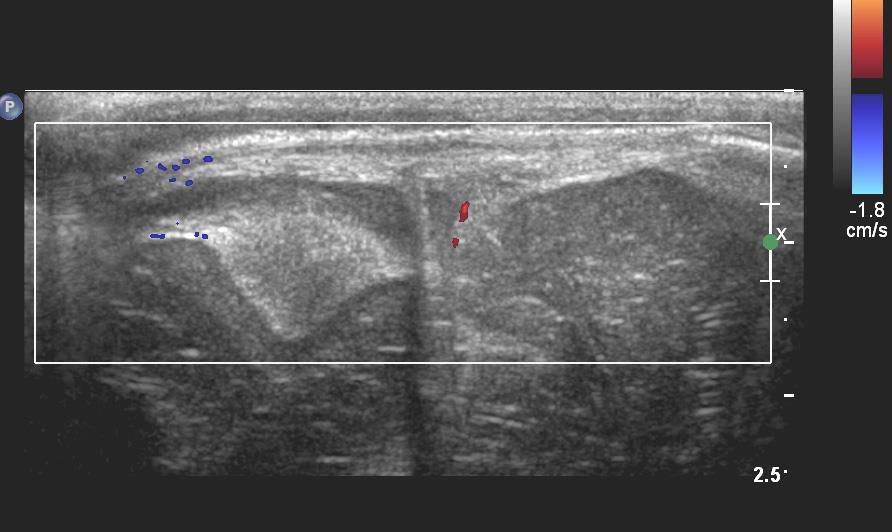
16 Transcranial Doppler Technique Neonate - Anterior Fontanelle Ant Cerebral Artery Sagittal midline


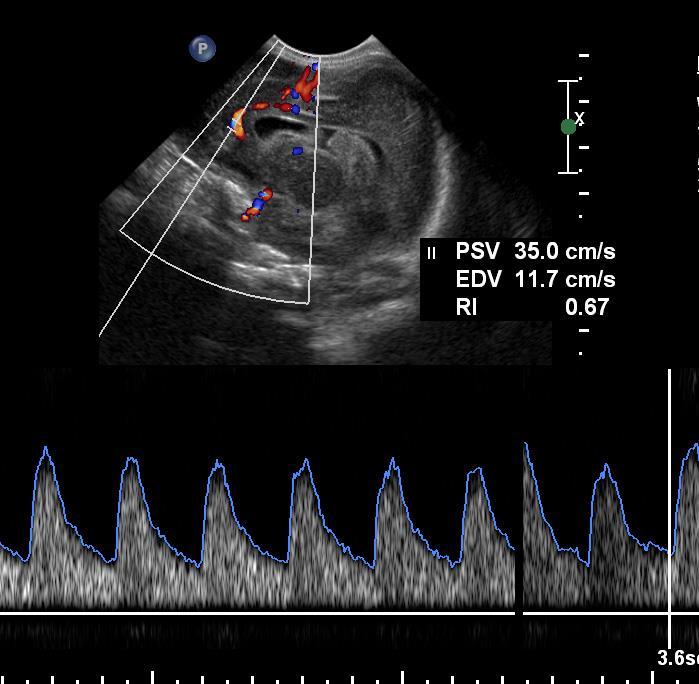
17 Transcranial Doppler Technique Neonate - Anterior Fontanelle Middle Cerebral Artery right and left via coronal plane


18
19

20 Resistive Index Peak Systole End Diastole Peak Systole Minimize affect of angulation Age dependent values Preterm infant % Term infant % By age %

21 Resistive Index An increase in diastolic flow will result in a decrease in RI A decrease in diastolic flow will result in an increase in RI as ICP increases above mean arterial pressure, diastolic flow may become reversed RI > 1.0.

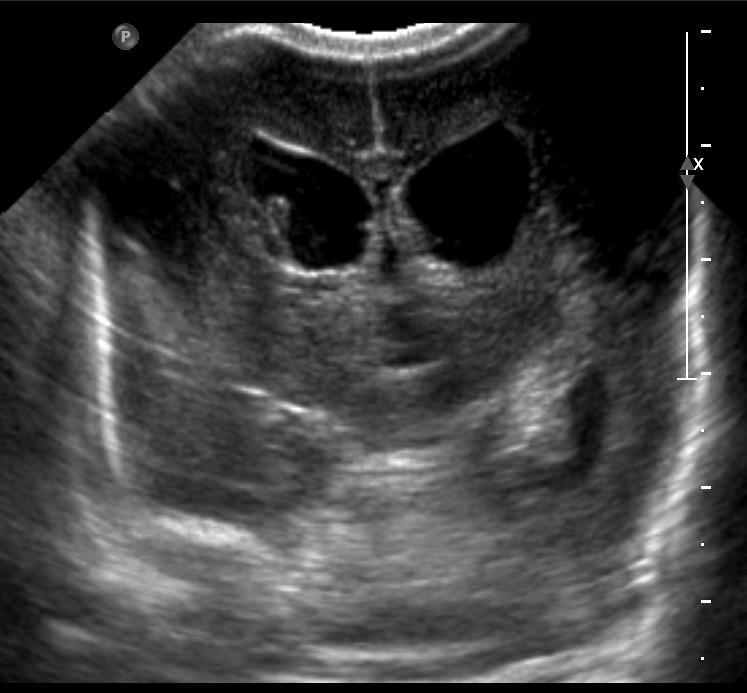
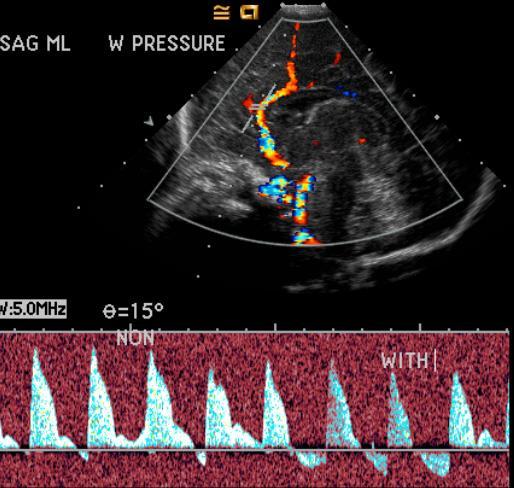
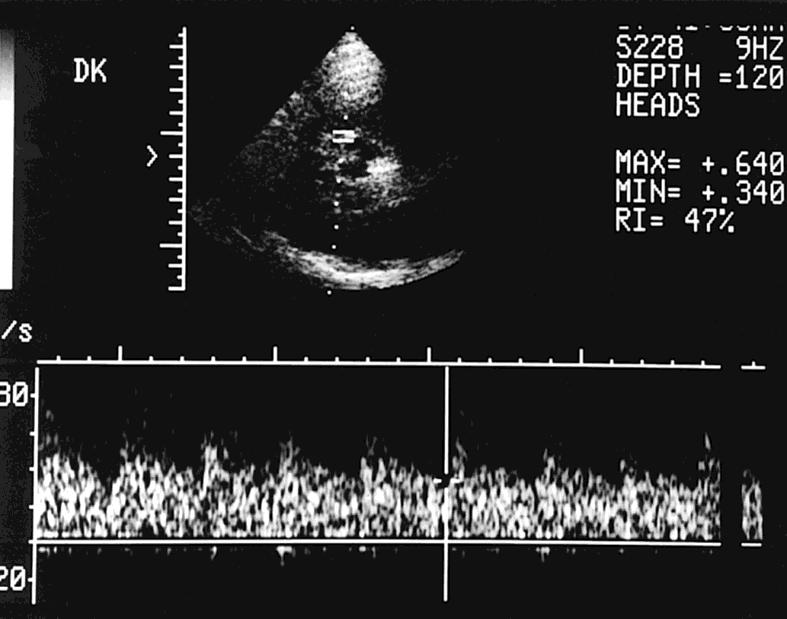
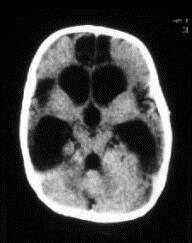
22 Hydrocephalus RI useful to identify increased ICP

23 Hydrocephalus Goh et al - RI sign of ICP >0.8 in neonate 0.65 in children Use to determine who needs to be tapped or shunted


24 Hydrocephalus Post tap, RI will decrease Persistently elevated RI may imply need to shunt
25

26 Determine Change in RI Taylor et al
27 R Barth
28 Beware! Head connected to the body!!

29 Patent Ductus Arteriosus
30 Hydrocephalus in Adults Resistive Index- wide variation of normal overlap nl/abn Need baseline values Need close correlation with clinical findings


31 Shunt Failure
32 Asphyxia May result in impaired cerebral autoregulation producing an increase in diastolic blood flow. Term infants following asphyxia. Low RI ( <.6) w/in the 48 o of asphyxia correlated with poor neurologic outcome. Archer et al Siebert et al

33

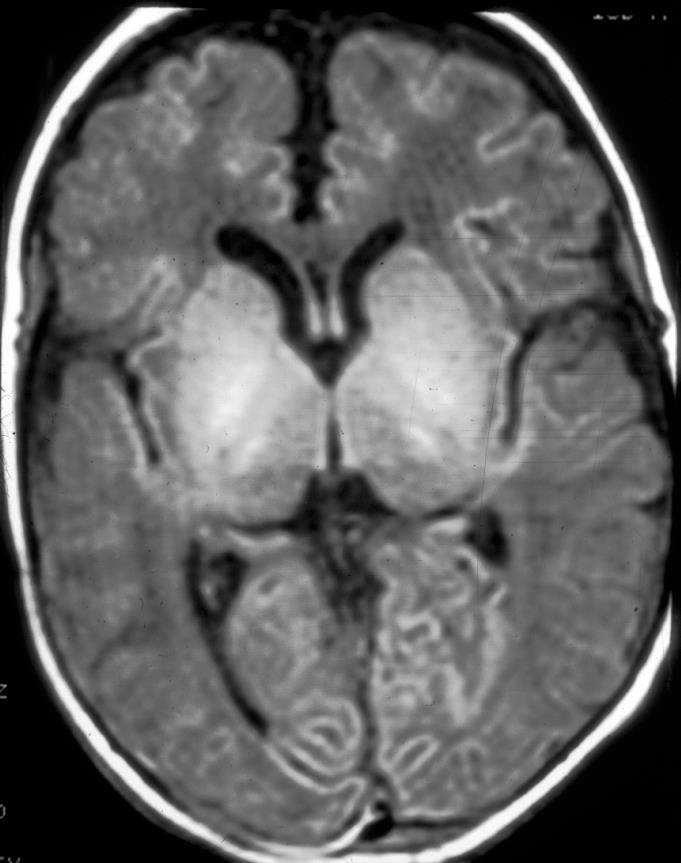
34 Hypoxic Ischemic Encephalopathy?

35 Asphyxia Loss of autoregulation described in older child after head injury or cardiac arrest. Bode et al May be useful in predicting cerebral injury If hyperventilation fails to alter the waveform pattern - vasomotor paralysis.
36 Hyperventilation CO 2 vasodilates > diastolic flow > RI. Low pco 2 vasoconstricts > diastolic flow > RI. CO 2 reactivity measurable If RI doesn t change with hyperventilation, severe brain injury present


37 Ruptured Intracranial Aneurysm 50% die within minutes ACA, ICA & MCA most frequent sites

38 Vasospasm Develops in first 2 days after SAH. Peaks 2 weeks later. Declines gradually during the subsequent 3 weeks.
39 Vasospasm As cross sectional area of vessel decrease, blood velocity increases TCD highly specific increased flow velocities precede clinical sxs of cerebral ischemia Guide optimal timing of surgery and Rx Decrease velocity > appropriate time to stop Rx Minimize complications, shorten ICU stay

40 Hemodynamics of Vasospasm: Attempt to maintain flow volume Elevated velocity often precedes onset of neurologic symptoms Velocity data impacts management
41 Vasospasm Protocol and Criteria: Criteria: Reach maximum: 7-12days; resolve 3wks. Mild: PSV cm/sec Moderate: cm/sec Severe: >200cm/sec risk for ischemia Rapid increase: PSV >25-50 cm/sec/day poor outcome Exam Protocol: Perform complete baseline study: R & L Identify highest velocities Monitor daily
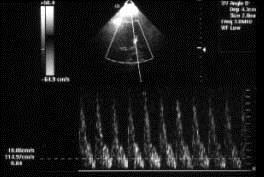
42 Vasospasm 18 yo s/p SAH LMCA >250 cm/s Lt MCA PSV 256 cm/s Therapy recommended w/ rapid increase vel (>50cm/s/day) or MCA PSV > 200 cm/sec a

43 Vasospasm Proximal MCA most accurate Severe PSV > 200 cm/sec rapid increase (>50 cm/s/day) Mean CBFV MCA/ICA ratio (cm/s) Lindegaard Ratio < 3 Nonspecific 3-6 Mild 3-6 Moderate >6 Severe Errors: increased ICP low volume flow peripheral vasospasm Combine with CLINICAL and LAB DATA


44 Cerebral vasculitis L. Lowe Small vessel vasculopathy rare in children Rt MCA PSV 108 cm/s acute stroke causes - post infectious, autoimmune, idiopathic. a PSV 310 cm/sec LMCA. b
45 Traumatic Brain Injury Pathologic processes often result in significant changes in cerebral hemodynamics. Timely dx crucial in head injury management.
46 Traumatic Brain Injury Acutely Loss of autoregulation -decrease in RI Vasospasm from SAH or posttraumatic hypervolemia - CBF velocity may increase
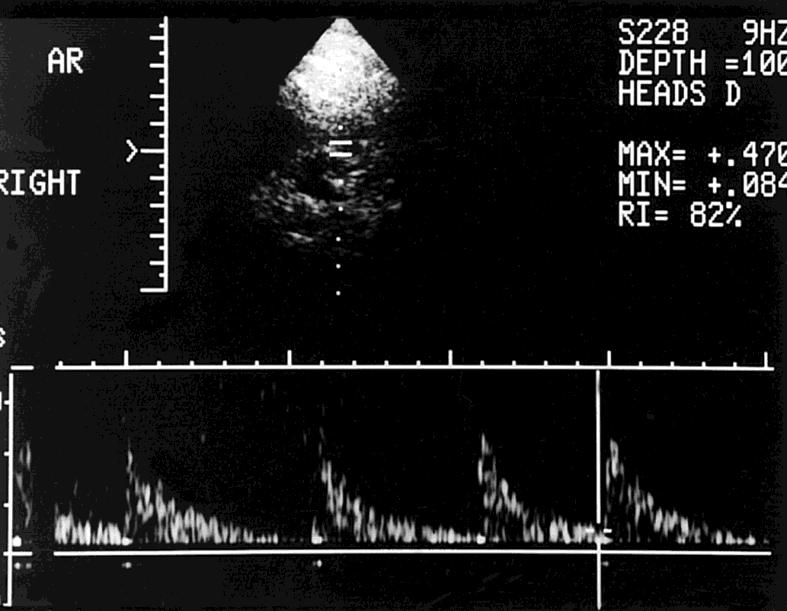
47 Traumatic Brain Injury If cerebral edema develops, RI will increase Vessels vasoconstrict As ICP increases above mean AA pressure, diastolic flow reverses. (RI>1)


48 Decrease then reversed diastolic flow
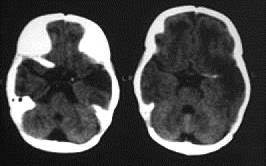
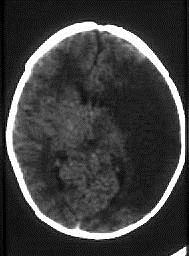
49 Progression to Brain Death Arrest of CBF at microcirculation level. Large vessels distend/constrict, thrombose/collapse. Cerebral circulation arrest Decrease in systolic velocity. Small spikes
50 Following trauma, Flow patterns - 4 categories 1. No significant intracranial flow 2. Reversal of diastolic flow 3. RI elevated 4. RI within normal range

51 1. No significant flow
52 2. Reversal of diastolic flow Typically clinical criteria for brain death within 24 hours of this pattern

53


54 3. Elevated RI with antegrade diastolic flow Can survive but may be neurologically devastated
55


56 4. Normal RI Typically survive but can have neurologic deficits

57 Retinal Artery Reduction in Retinal Arterial and Venous flow velocities in children w/ elevated ICP Miller et al J of Child Neurology 2009;24:30
58

59 Miller et al J of Child Neurology 2009;24:30
60 Retinal Artery Another potential adjunct to monitor ICP in the acute setting when serial evaluations are needed if transtemporal TCD or ICP monitoring not available
61 Safety Can cause heat and cavitation Must keep output to a minimum ALARA Limit examination time
62 Traumatic Brain Injury Serial TCD readings can evaluate progression of cerebral edema follow course of treatment. Useful to assess response to hyperventilation
63 Hyperventilation Rx Decreasing CO 2 - cerebral vessels vasoconstrict - RI should increase Children w/ reduced or absent PaCo 2 vasoreactivity w/in 24 o of injury = vegetative or died Beyda DH,. Wade ed. 1987
64 Brain Death Establishing brain death can be problematic. Neurologic examination-apnea test EEG Brainstem evoked potential Nuclear blood flow studies The use of TCD adds another noninvasive method of determining brain death
65 Brain Death-TCD Advantages Noninvasive Repeatable Portable Inexpensive Ease in performing Can be used in phenobarb coma (EEG nondiagnostic).

66 Brain Death?




67 Brain Death?

68 Cerebral Angiogram

69 Brain Death Reversal of diastolic flow can be characteristic of essentially absent effective cerebral circulation in the adult and older child.
70 Direction of Flow Index Kirkham - Direction of Flow Index: DFI = 1 peak systolic velocity area peak diastolic velocity area If DFI negative- area of reverse flow >forward flow All children with a negative DFI and time ave velocity < 10 cm/sec over 30 min died w/out brainstem function recovery. Kirkham F, J Neurology 1987;50:1504.


71 Brain Death Patterns - Small early systolic spikes - Arrest of antegrade flow

72 Brain Death Patterns

73 Brain Death Patterns Absent flow in MCA Reversal of diastolic flow in extracranial ICA
74 Infant Brain Death Concern of TCD reliability in infant brain death assessment In neonates, low RI s have been described in clinically dead patients. Infants with extremely high RI s have survived Careful clinical correlation crucial in determining brain death as arrest of supratentorial flow not synonymous with brain death rather it is confirmatory
75 Brain Death TCD exam should never be used in isolation to supplant clinical neurologic findings in children and neonates Provides data indicating severity of cerebrovascular arrest. Repeat study to confirm CBF arrest sufficient to cause irreversible damage to supratentorial structures
76 Conclusions TCD can be used to monitor children with severe head injury portable noninvasive rapid can be repeated often Provides a useful adjunct in the clinical assessment of the injured patient.
77 US is a powerful tool Provides a useful adjunct in the neurologic assessment of the critically ill patient.


78 Thank you!
79 Retinoschesis
80
81
82
 Connected to the subarachnoid space, ONS diameter is influenced by CSF pressure")
83 Optic Nerve Sheath Optic NN surrounded by CSF and dura forming the optic nerve sheath (ONS) Connected to the subarachnoid space, ONS diameter is influenced by CSF pressure variation
84 Optic Nerve Sheath Diameter Rapid diagnosis of Intracranial Hypertension can be critical to appropriate therapy Invasive procedures such as ICP monitoring or neuroimaging may not be available CT may underestimate the amount of ICP elevation
85 Optic Nerve Sheath Diameter Several ONSD Studies have demonstrated correlation with direct measurement of ICP low interobserver variability Meretti et al Acta Anesth Scan 2011
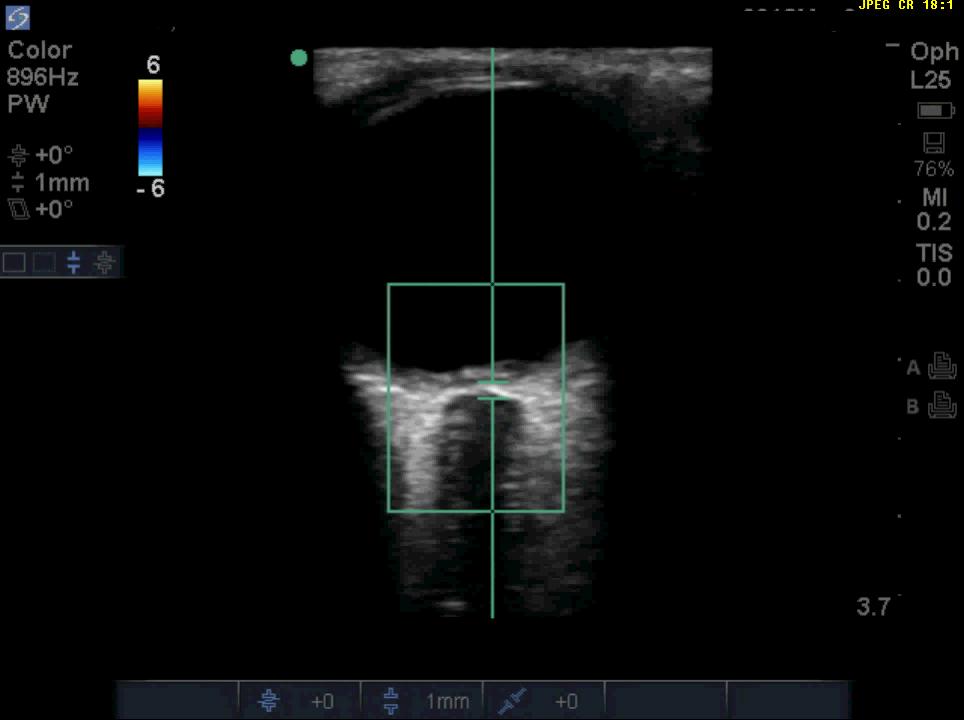
86 Technique High frequency linear probe > 7.5 MHz. Gel on closed eyelid - No pressure Superficial program 4-5 cm depth gain optimize contrast b/w ONS and periorbital fat. 2 measures in transverse and sag planesmean



87 Optic Nerve Measured 3 mm behind the globe
88 ONSD Measurement cut offs > 4 yo to Adults 5mm 1-4 years 4.5 mm < 1 yo 4 mm Bedside US of ONSD may be useful in assessing ICP if invasive monitoring not feasible
89 ONSD Problems No clear consensus on upper normal ONSD limit Difficulty measuring diameter dependent on experience, frequency of probe, age of equipment. Rapid ICP changes may underestimate measures- lag times documented
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
DISCLOSURES. Specific TCD clinical applications for patients with traumatic brain injury 1/10/2015. FTE, Private Practice for profit TBI TBI: SCOPE
 DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
DISCLOSURES Specific TCD clinical applications for patients with traumatic brain injury FTE, Private Practice for profit Alexander Razumovsky, PhD, FAHA 38 35 th Annual Meeting 38 35 th Annual Meeting
SCORCH 2018 Bone, Brain & Vessels
 To complete the SAM assessment, please use one of the methods below: Complete a paper version of the exam Go to: https://www.surveymonkey.com/r/thurssam Open your smartphone camera and scan this QR Code
To complete the SAM assessment, please use one of the methods below: Complete a paper version of the exam Go to: https://www.surveymonkey.com/r/thurssam Open your smartphone camera and scan this QR Code
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Neurosonography: State of the art
 Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
Neurosonography: State of the art Lisa H Lowe, MD, FAAP Professor and Academic Chair, University MO-Kansas City Pediatric Radiologist, Children s Mercy Hospitals and Clinics Learning objectives After this
noninvasive, nonionizing, portable, inexpensive, safe for serial or prolonged studies
 TRANS CRANIAL DOPPLER Presented by : Anil Garg Transcranial Doppler 1982, Aaslid and colleagues introduced TCD as a non-invasive technique for monitoring blood flow velocity in basal cerebral arteries
TRANS CRANIAL DOPPLER Presented by : Anil Garg Transcranial Doppler 1982, Aaslid and colleagues introduced TCD as a non-invasive technique for monitoring blood flow velocity in basal cerebral arteries
Intracranial Cerebrovascular Evaluation Transcranial Doppler (Non-Imaging) and Transcranial Duplex Imaging (TCD-I)
 and Transcranial Duplex Imaging (TCD-I)") VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Intracranial Cerebrovascular Evaluation Transcranial Doppler (Non-Imaging) and Transcranial Duplex Imaging (TCD-I) This Guideline was prepared by
VASCULAR TECHNOLOGY PROFESSIONAL PERFORMANCE GUIDELINES Intracranial Cerebrovascular Evaluation Transcranial Doppler (Non-Imaging) and Transcranial Duplex Imaging (TCD-I) This Guideline was prepared by
What effects will proximal or distal disease have on an waveform?
 Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Spectral Doppler Interpretation Director Director of of Ultrasound Ultrasound Education Education & & Quality Quality Assurance Assurance Baylor Baylor College College of of Medicine Medicine Division
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
ISPUB.COM. Transcranial Doppler: An Overview of its Clinical Applications. A Alexandrov, M Joseph INTRODUCTION SICKLE CELL DISEASE
 ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
What effects will proximal or distal disease have on a waveform?
 Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
Spectral Doppler Interpretation Director of Ultrasound Education & Quality Assurance Baylor College of Medicine Division of Maternal-Fetal Medicine Maternal Fetal Center Imaging Manager Texas Children
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Transcranial Doppler In Cerebral Vasospasm
 Cerebral Vasospasm 1042-3680/90 $0.00 +.20 Transcranial Doppler In Cerebral Vasospasm David W. Newell, MD,* and H. Richard Winn, MDt The confirmation of cerebral vasospasm following subarachnoid hemorrhage,
Cerebral Vasospasm 1042-3680/90 $0.00 +.20 Transcranial Doppler In Cerebral Vasospasm David W. Newell, MD,* and H. Richard Winn, MDt The confirmation of cerebral vasospasm following subarachnoid hemorrhage,
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico
 Roma 25 Maggio 2018 L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico behind the cotton wool of papilledema Dott. Elena Casiello Scuola di Specializzazione in Anestesia
Roma 25 Maggio 2018 L'Ecografia del nervo ottico nel monitoraggio della PIC nel traumatizzato cranico behind the cotton wool of papilledema Dott. Elena Casiello Scuola di Specializzazione in Anestesia
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
patients having vascular malformations of the brain, a relatively normal vascular tree can be assumed for
 Intracranial Duplex Doppler: Practical Uses in Pediatric Neurology and Neurosurgery William M. Chadduck, MD; Joanna J. Seibert, MD Abstract The value of pulsed Doppler studies of the cerebral vessels of
Intracranial Duplex Doppler: Practical Uses in Pediatric Neurology and Neurosurgery William M. Chadduck, MD; Joanna J. Seibert, MD Abstract The value of pulsed Doppler studies of the cerebral vessels of
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
Probe Selection A high frequency (7-12 MHz) linear array transducer should be used to visualize superficial structures (Image 1).
 linear array transducer should be used to visualize superficial structures (Image 1).") ! Teresa S. Wu, MD, FACEP Director, Emergency Ultrasound Program & Fellowships Co-Director, Women s Imaging Fellowship Maricopa Medical Center Associate Professor, Emergency Medicine Director, Simulation
! Teresa S. Wu, MD, FACEP Director, Emergency Ultrasound Program & Fellowships Co-Director, Women s Imaging Fellowship Maricopa Medical Center Associate Professor, Emergency Medicine Director, Simulation
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Case Conference: Neuroradiology. Case 1: Tumor Case 1: 22yo F w/ HA and prior Seizures
 Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Case Conference: Neuroradiology Case 1: 22yo F w/ HA and prior Seizures David E. Rex, MD, PhD Stanford University Hospital Department of Radiology Case 1: Tumor Most likely gangiloglioma, oligodendroglioma,
Transcranial Doppler (Basic Step) Dae-il Chang, M.D., Sung Sang Yoon, M.D. Department of Neurology, College of Medicine, Kyunghee university
 Dae-il Chang, M.D., Sung Sang Yoon, M.D. Department of Neurology, College of Medicine, Kyunghee university") Transcranial Doppler (Basic Step) Dae-il Chang, M.D., Sung Sang Yoon, M.D. Department of Neurology, College of Medicine, Kyunghee university Principles of Doppler Ultrasonography Major target Speed & direction
Transcranial Doppler (Basic Step) Dae-il Chang, M.D., Sung Sang Yoon, M.D. Department of Neurology, College of Medicine, Kyunghee university Principles of Doppler Ultrasonography Major target Speed & direction
Dural Arteriovenous Malformations and Fistulae (DAVM S DAVF S)
") Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Jorge Guedes Campos NEUROIMAGING DEPARTMENT HOSPITAL SANTA MARIA UNIVERSITY OF LISBON PORTUGAL DEFINITION region of arteriovenous shunting confined to a leaflet of packymeninges often adjacent to a major
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography
 Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards
 Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
Protokollanhang zur SPACE-2-Studie Neurology Quality Standards 1. General remarks In contrast to SPACE-1, the neurological center participating in the SPACE-2 trial will also be involved in the treatment
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Bilaga 4 till rapport 1 (17)
") Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
Bilaga 4 Tabeller, beskrivning av studier Bilaga 4 till rapport 1 (17) Bilddiagnostik vid misstanke om total hjärninfarkt en systematisk litteraturöversikt, rapport 282 (2018) SBU Statens beredning för
TCD evaluation is used in several countries as a confirmatory test to assess CBF arrest
 ! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
! BRAIN DEATH IS THE IRREVERSIBLE LOSS OF FUNCTION OF THE ENTIRE BRAIN INCLUDING THE BRAIN STEM Conventional Confirmatory Tests: EEG, CEREBRAL AGF, BRAIN SCINTIGRAPHY LOGISTICAL PROBLEMS TCD evaluation
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Ultrasound examination of the neonatal brain
 Ultrasound examination of the neonatal brain Guideline for the performance and reporting of neonatal and preterm brain ultrasound examination, by the Finnish Perinatology Society and the Paediatric Radiology
Ultrasound examination of the neonatal brain Guideline for the performance and reporting of neonatal and preterm brain ultrasound examination, by the Finnish Perinatology Society and the Paediatric Radiology
Monitoring of Regional Cerebral Blood Flow Using an Implanted Cerebral Thermal Perfusion Probe Archived Medical Policy
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Neuroradiology. of Stroke and Headaches
 Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
Neuroradiology of Stroke and Headaches Learning Objec:ves 1. Iden:fy T1 and T2 sequences 2. Recall the normal anatomy of the intracranial circula:on 3. Apply appropriate CT and MR imaging of the brain
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
acute-onset, severe, recurrent reversible vasoconstriction
 1 RCVS A clinical and radiologic syndrome Characterized by acute-onset, severe, recurrent headache and reversible vasoconstriction of the cerebral arteries RCVS accounts for most benign thunderclap headaches"
1 RCVS A clinical and radiologic syndrome Characterized by acute-onset, severe, recurrent headache and reversible vasoconstriction of the cerebral arteries RCVS accounts for most benign thunderclap headaches"
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Dorit Donoviel, Ph.D.
 Dorit Donoviel, Ph.D. Assistant Professor Pharmacology & Center for Space Medicine Baylor College of medicine Deputy Chief Scientist Industry Forum Lead National Space Biomedical Research Institute (NSBRI)
Dorit Donoviel, Ph.D. Assistant Professor Pharmacology & Center for Space Medicine Baylor College of medicine Deputy Chief Scientist Industry Forum Lead National Space Biomedical Research Institute (NSBRI)
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech
 Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Acute Complications of Sickle Cell Disease Case Study 5 year old girl with Hemoglobin SS, weakness and slurred speech Beatrice E. Gee, MD Medical Director, Sickle Cell and Hematology Program Children s
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
This quiz is being published on behalf of the Education Committee of the SNACC.
 Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
Quiz 48 Cerebrovascular Atherosclerotic Disease Shobana Rajan, M.D. Associate Director of Neuroanesthesia, Vice Chair of Education, Allegheny Health Network. Quiz team; Suneeta Gollapudy M.D, Angele Marie
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Carotid Ultrasound: Improving Ultrasound
 Carotid Ultrasound: Improving Ultrasound Edward I. Bluth, M.D., F.A.C.R. Chairman Emeritus, Department of Radiology, Ochsner Clinic Foundation, New Orleans, Louisiana Professor, Ochsner Clinical School,
Carotid Ultrasound: Improving Ultrasound Edward I. Bluth, M.D., F.A.C.R. Chairman Emeritus, Department of Radiology, Ochsner Clinic Foundation, New Orleans, Louisiana Professor, Ochsner Clinical School,
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
TCD in Intensive Care
 TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
TCD in Intensive Care Background: Transcranial Doppler (TCD) ultrasonography is a technique that uses a hand-held Doppler transducer (placed on the surface of the cranial skin) to measure the velocity
Transorbital blood flow sound recordings have the
 397 Noninvasive Detection of Intracranial Vascular Lesions by Recording Blood Flow Sounds Yasushi Kurokawa, MD; Seisho Abiko, MD; Kohsaku Watanabe, MD Background and Purpose Transorbital blood flow sound
397 Noninvasive Detection of Intracranial Vascular Lesions by Recording Blood Flow Sounds Yasushi Kurokawa, MD; Seisho Abiko, MD; Kohsaku Watanabe, MD Background and Purpose Transorbital blood flow sound
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
JMSCR Vol 07 Issue 01 Page January 2019
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v7i1.01 Utility of Serial Transcranial
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v7i1.01 Utility of Serial Transcranial
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Vascular Imaging in the Pediatric Abdomen. Jonathan Swanson, MD
 Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Carotid US: More than just a chart on the wall
 Carotid US: More than just a chart on the wall Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section Medical
Carotid US: More than just a chart on the wall Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section Medical
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL
 GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
GUNDERSEN/LUTHERAN ULTRASOUND DEPARTMENT POLICY AND PROCEDURE MANUAL SUBJECT: Carotid Duplex Ultrasound SECTION: Vascular Ultrasound ORIGINATOR: Deborah L. Richert, BSVT, RDMS, RVT DATE: October 15, 2015
Any vascular studies performed should be as a result of, or to complement, a thorough patient evaluation and neurological examination.
 National Imaging Associates, Inc. Clinical guidelines NON-INVASIVE CEREBROVASCULAR ARTERIALS TUDIES Original Date: October 2015 Page 1 of 8 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes: Please refer to page
National Imaging Associates, Inc. Clinical guidelines NON-INVASIVE CEREBROVASCULAR ARTERIALS TUDIES Original Date: October 2015 Page 1 of 8 FOR CMS (MEDICARE) MEMBERS ONLY CPT4 Codes: Please refer to page
Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries
 J Neurosurg 57:769-774, 1982 Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries RUNE AASLID, PH.D., THOMAS-MARC MARKWALDER, M.D., AND HEt,CE NORNES, M.D.
J Neurosurg 57:769-774, 1982 Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries RUNE AASLID, PH.D., THOMAS-MARC MARKWALDER, M.D., AND HEt,CE NORNES, M.D.
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Cerebrovascular Malformations in the Elderly Indications for Treatment
 Cerebrovascular Malformations in the Elderly Indications for Treatment Johanna T. Fifi, MD, FAHA, FSVIN Director of Endovascular Ischemic Stroke Assistant Professor of Neurology, Neurosurgery, and Radiology
Cerebrovascular Malformations in the Elderly Indications for Treatment Johanna T. Fifi, MD, FAHA, FSVIN Director of Endovascular Ischemic Stroke Assistant Professor of Neurology, Neurosurgery, and Radiology
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Hypervolemic Versus Normovolemic Therapy in Patients with Ruptured Cerebral Aneurysm. Sung Don Kang, M.D., Ph.D., Yo Sik Kim, M.D., Ph.D.
 원저 J Korean Neurol Assoc / Volume 24 / August, 2006 파열동맥류환자에서과혈량대정상혈량치료 원광대학교의과대학신경외과학교실, 신경과학교실 a 강성돈김요식 a Hypervolemic Versus Normovolemic Therapy in Patients with Ruptured Cerebral Aneurysm Sung Don
원저 J Korean Neurol Assoc / Volume 24 / August, 2006 파열동맥류환자에서과혈량대정상혈량치료 원광대학교의과대학신경외과학교실, 신경과학교실 a 강성돈김요식 a Hypervolemic Versus Normovolemic Therapy in Patients with Ruptured Cerebral Aneurysm Sung Don
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Cerebral vasospasm evaluated by transcranial Doppler ultrasonography at different intracranial pressures
 J Neurosurg 75:752-758, 1991 Cerebral vasospasm evaluated by transcranial Doppler ultrasonography at different intracranial pressures J[)RGEN KLINGELH()FER, M.D., DIRK SANDER, M.D., MANFRED HOLZGRAEFE,
J Neurosurg 75:752-758, 1991 Cerebral vasospasm evaluated by transcranial Doppler ultrasonography at different intracranial pressures J[)RGEN KLINGELH()FER, M.D., DIRK SANDER, M.D., MANFRED HOLZGRAEFE,
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Managing pediatric head trauma with elevated intracranial
 Original Article ARapidNoninvasiveMethodofDetectingElevated Intracranial Pressure Using Bedside Ocular Ultrasound Application to 3 Cases of Head Trauma in the Pediatric Emergency Department James W. Tsung,
Original Article ARapidNoninvasiveMethodofDetectingElevated Intracranial Pressure Using Bedside Ocular Ultrasound Application to 3 Cases of Head Trauma in the Pediatric Emergency Department James W. Tsung,
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012
 Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Carotid Abnormalities Coils, Kinks and Tortuosity David Lorelli M.D., RVT, FACS Michigan Vascular Association Conference Saturday, October 20, 2012 Page 1 Table of Contents Carotid Anatomy Carotid Duplex
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report
 214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
214 Balasa et al - Acute cerebral MCA ischemia Acute cerebral MCA ischemia with secondary severe head injury and acute intracerebral and subdural haematoma. Case report D. Balasa 1, A. Tunas 1, I. Rusu
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.