A Nervous Breakdown: Multimodality Imaging of Thoracic Neurogenic Tumors
|
|
|
- Alisha Holland
- 5 years ago
- Views:
Transcription





1 A Nervous Breakdown: Multimodality Imaging of Thoracic Neurogenic Tumors John P. Lichtenberger III, MD, Maj, USAF, MC Assistant Professor, Dept. or Radiology Uniformed Services University of the Health Sciences Bethesda, Maryland
2 DISCLOSURES John P. Lichtenberger III, MD: author for Amirsys, Inc.; author for Reed Elsevier The views, information, or content and conclusions expressed herein are those of the author(s) and do not reflect the official position or policy of the Departments of the Army, Air Force, Defense, or the U.S. Government, nor should any official endorsement be inferred by the Department of Defense, or the U.S. Government.





3 GOALS AND OBJECTIVES Illustrate the complex anatomy of the nervous system within the chest wall and mediastinum Detail the important epidemiologic and pathophysiologic features to use in an approach to neurogenic tumors Identify key imaging features of neurogenic tumors occurring in the chest, focusing on distinguishing characteristics Explain the relative advantages of imaging modalities when examining neurogenic tumors







4 NEUROANATOMY OF THE THORAX Spinal Nerve Somatic Nervous System Sensation and motor innervation of the thorax Ventral nerves T1 T11 lateral and anterior cutaneous branches Anterior branch has an accessory branch T1 contributes to the brachial plexus Special nerves such as phrenic nerve course through the thorax T12 part of the lumbar plexus called the subcostal nerve Anterior Cutaneous Nerve Lateral Intercostal Nerves Collateral Intercostal Nerves




5 NEUROANATOMY OF THE THORAX Sympathetic Nervous System Sympathetic chain preganglionic sympathetic fibers arrive via white rami communications of ventral primary rami of spinal nerves T1 L2 Form greater thoracic splanchnic nerve, lesser thoracic splanchnic nerve, and least thoracic splanchnic nerve Left Phrenic Nerve Left Vagus Nerve Sympathetic chain



6 NEUROANATOMY OF THE THORAX Sympathetic ganglia Sympathetic trunk Intercostal nerve Communicating rami Greater splanchnic nerve Lesser splanchnic nerve Least splanchnic nerve



7 NEUROANATOMY OF THE THORAX Recurrent Laryngeal Nerves Parasympathetic Vagus nerve Right Vagus Nerve Left Vagus Nerve Forms several different plexi providing parasympathetic innervation including, esophageal plexus, cardiac plexus, pulmonary plexus Esophageal Plexus
 to define the")

 Posterior")
8 KEY FEATURE: LOCATION A recent study (Japanese Association for Research on Thymus) to define the mediastinum, divided it into the following components: Superior portion of the mediastinum Anterior mediastinum (prevascular) Middle mediastinum (peri-tracheoesophageal zone) Posterior mediastinum (paravertebral)



9 KEY FEATURE: LOCATION Superior portion of the mediastinum borders: Superior border thoracic inlet Inferior border horizontal plane at the intersection of the caudate margin of the brachiocephalic vein with the trachea Anterior sternum Lateral parietal pleural reflections Posteriorly by the anterior rim of the thoracic vertebral body Posterolaterally by a vertical line against the posterior rim of the chest wall at the lateral rim of the thoracic vertebral transverse process

10 KEY FEATURE: LOCATION Anterior mediastinum (prevascular) borders: Superior boundary inferior boundary of the superior portion of the mediastinum Inferior diaphragm Anterior sternum Lateral parietal pleural reflections Posterior the percardium, anterior rims of the left brachiocephalic vein, superior vena cava, superior and inferior pulmonary veins, ascending aorta and the lateral rim of the aortic arch Axial contrast CT at the level of aortic arch Differential diagnosis based on paper results: Thymoma (192), thymic carcinoma (52), thymic lymphoma (24), mature teratoma (24), malignant germ cell tumor (30), pericardial cyst (10) out of 343 tumors.

11 KEY FEATURES: LOCATION Middle mediastinum (peritracheoesophageal zone) borders: Superior boundary inferior boundary of the superior portion of the mediastinum Inferior diaphragm Anterior posterior rim of the left brachiocephalic vein, superior vena cava, ascending aorta, bilateral main pulmonary arteries and the heart Posterior, the anterior rim of the descending aorta and a vertical line connecting a point on each thoracic vertebral body at 1 cm behind it anterior margin Axial contrast CT at the level of the main pulmonary artery Differential diagnosis based on paper results: Bronchogenic cyst (25), neurogenic tumors (6), pericardial cyst (5), enteric cyst (2) out of 38 tumors

12 KEY FEATURES: LOCATION Posterior mediastinum (paravertebral) borders: Superior boundary inferior boundary of the superior mediastinum Inferior border diaphragm Anterior boundary of the middle mediastinum Posterio-lateral vertical line against the posterior rim of the chest wall at the lateral rim of the lateral process of the thoracic spine Axial contrast CT at the level of the heart Differential diagnosis based on paper results: Neurogenic tumors (29) and bronchogenic cyst (7) out of 37 tumors


13 KEY FEATURES: LOCATION Another study evaluating location of neurogenic tumors found: Large airways extremely rare: 26 reported cases from 1950 to 2003, 23 schwannomas and 3 neurofibromas Lung extremely rare: 62 as pulmonary schwannomas, 17 as primary pulmonary paraganglioma Mediastinum one of the most commonly encountered mediastinal tumors (comprising 15-25%), predominantly located in the posterior mediastinum Chest wall one of the more usual chest wall tumors characterized by pressure deformity and displacement of the adjacent ribs and vertebrate Coronal contrast enhanced CT demonstrating a malignant peripheral nerve sheath tumor of the chest wall. Axial contrast CT demonstrating a schwannoma of the posterior mediastinum
14 KEY FEATURE: DEMOGRAPHICS Differentiation based on age Around approximately 15 years of age neurogenic tumors shift from ganglion cell tumors in patient s younger than 15, to nerve sheath tumors in patient s older Similarly at around the same age the prevalence of malignant neurogenic tumors in patient s less than 15 years shift to a greater prevalence of benign neurogenic tumor in patient s older Posteroanterior radiograph of a patient <15 years of age with ganglioneuroma demonstrate a large mass in the posterior mediastinum. Posteroanterior radiograph of a patient >15 years of age with schwannoma demonstrates a smoothly marginated, oval paraspinal mass.

15 KEY FEATURE: SHAPE Neurofibromas and schwannomas typically demonstrate a lobulated spherical contour May have a dumbbell or hourglass configuration when projecting through the spinal canal Ganglia tumors typically demonstrate oblong mass with a broad base anterolateral aspect of the spine
16 KEY FEATURE: SHAPE Tumor Morphological differences between schwannomas and ganglioneuromas in the mediastinum Major axis length Craniocaudal length The craniocaudal length to major axis ratio (CC/M) may be used to differentiate between schwannoma and ganglioneuroma Since the plane of growth of ganglion tumors is parallel to the spine the craniocaudal axes is longer than with schwannomas as their plane of growth is perpendicular to the spine
17 KEY FEATURE: SHAPE Morphological differences between schwannomas and ganglioneuromas in the mediastinum Plane of growth of ganglion tumors is parallel to the spine the craniocaudal axes is longer than with schwannomas as their plane of growth is perpendicular to the spine

18 IMAGING FEATURES OF NEUROGENIC TUMORS MRI characteristics and usefullness MRI schwannomas and neurofibromas typically have low to intermediate signal intensity on T1 weighted images and have areas of intermediate to high signal intensity on T2 weighted sequences MRI ganglia cell tumors homogenous intermediate signal intensity on all sequences, occasionally with a whorled appearance on T1 weighted images and heterogenous high signal intensity on T2 weighted sequences MRI is performed to exclude intraspinal tumor extension Axial T2 non fat saturation image of the thorax demonstrates heterogenous internal signal intensity more commonly found in nerve sheath tumors Axial T2 non fat saturation image of the thorax demonstrates a more homogenous signal intensity mass in the posterior mediastinm more consistent with a ganglion cell tumor


19 GANGLION TUMORS Ganglioneuroma Fully differentiated neuronal tumor Patients generally older than 10, male predominant Composed of ganglion cells, schwann cells, and fibrous tissue Key Imaging Features Generally occur in the posterior mediastinum (approximately 40%), then retroperitoneum, and cervical regions Posteroanterior and lateral chest radiographs of a 7 year old with ganglioneuroma demonstrate a large mass in the posterior mediastinum. The mass is elongated and oriented in a vertical axis in the direction of the sympathetic chain.




20 GANGLIONEUROMA MRI FINDINGS Ganglioneuroma in a 7 year old. Enhanced CT scan at the level of the heart shows a left paravertebral oval enhancing soft tissue mass displacing the heart to the right. The low internal attenuation is due to the abundant myxoid matrix. The mass is oriented along the sympathetic chain. Multiplanar multisequece MRI demonstrates an intermediate signal intensity mass on all sequences with a somewhat whorled appearance caused by curvilinear or nodular bands of low signal intensity on both T1- and T2- weighted images Multiplanar multisequece MRI demonstrates an intermediate signal intensity mass on all sequences with a somewhat whorled appearance caused by curvilinear or nodular bands of low signal intensity on both T1- and T2- weighted images



21 GANGLIONEUROMA CT FINDINGS 7 year old with a ganglioneuroma. Bone logrithim demonstrates puncatate calcifications. Calcifications may be present in approximately 20% of tumors and is more common in sympathetic ganglia tumors than nerve sheath tumors. Ganglioneuroma in a 7 year old. Coronal se illustrate the broad base along the anterolateral aspect of the spine spanning 3 to 5 vertebrae a common finding. Coronal and sagittal images illustrate the broad base along the anterolateral aspect of the spine spanning 3 to 5 vertebrae a common finding.


22 GANGLIONEUROMA MRI FINDINGS Multiplanar multisequece MRI demonstrates an intermediate signal intensity mass on all sequences with a somewhat whorled appearance caused by curvilinear or nodular bands of low signal intensity on both T1- and T2-weighted images Multiplanar multisequece MRI demonstrates an intermediate signal intensity mass on all sequences with a somewhat whorled appearance caused by curvilinear or nodular bands of low signal intensity on both T1- and T2-weighted images Multiplanar multisequece MRI demonstrates an intermediate signal intensity mass on all sequences with a somewhat whorled appearance caused by curvilinear or nodular bands of low signal intensity on both T1- and T2-weighted images

23 GANGLION TUMORS Ganglioneuroblastoma Intermediate tumor between ganglioneuroma and neuroblastoma Variable imaging characteristics on a spectrum ranging from a similar appearance to ganglioneuroma à neuroblastoma Affect male and female subjects equally Presents in patients younger than 10 years old Key Imaging Features May manifest as a sharply marginated oblong paraspinous mass or may be irregular, locally invasive, and widely metastatic

24 GANGLION TUMORS Neuroblastoma Most common extracranial solid childhood malignancy Typically occurs in infants and very young children (mean age of presentation 22 months) Most commonly present in the abdomen, then mediastinum, neck and lower extremity Key Imaging Features Non encapsulated, frequently containing extensive areas of hemorrhage, necrosis, and cystic degeneration May be further evaluated with mibg, PET, or Tc-99m bone scan. Posterioanterior radiograph of a 10 month old with neuroblastoma who presents with cough and fever demonstrates a paravertebral mass displacing the azygoesophageal reflection.




25 NEUROBLASTOMA IMAGING FINDINGS Axial contrast enhanced CT in a 10 month old demonstrates a paravertebral posterior mediastinal mass homogenous solid mass. Sagittal T2 image demonstrates a homogenous paraspinal T2 hyperintense signal posterior mediastinal mass Coronal T1 fat saturation contrast enhanced image demonstrates a homogenous paraspinal enhancing posterior mediastinal mass Coronal I-123 mibg demonstrates radiotracer localization within the mass


26 PARAGANGLION TUMORS Paraganglioma Tumor of paraganglion cells Found in sympathetic or parasympathetic chains Benign and malignant are histologically indistinguishable Component of hereditary paragangliomapheochromocytoma syndrome Key Imaging Features Typically arise adjacent to the pericardium or heart, within the interatrial septum or left atrial wall, or from autonomic tissue along the paravertebral sulci Tumors often hypervascular on imaging and demonstrate central necrosis and hemorrhage Coronal contrast-enhanced CT of a patient with paraganglioma in a characteristic location adjacent to the pericardium demonstrates a wellcircumscribed, elongated mass with enhancement and prominent internal vascularity.

 Key Imaging Features Well circumscribed encapsulated masses Adjacent bone changes may")

27 SCHWANNOMAS PERIPHERAL NERVE SHEATH TUMORS Derived from schwann cells Arise eccentrically from the parent nerve Symptoms related to compression of the parent nerve Peak presentation 40 and 50 years of age Histiologically composed of two cell types: Antoni A (cellular) and Antoni B (myxoid) Key Imaging Features Well circumscribed encapsulated masses Adjacent bone changes may include splaying of the ribs, or enlargement of an intervertebral foramen. Posteroanterior and lateral chest radiographs of a patient with schwannoma demonstrates a smoothly marginated, oval paraspinal mass.

28 SCHWANNOMA CT FINDINGS Axial and coronal non-contrast CT images demonstrate expansion of the T2 neuroforamen and erosion of the T2 vertebral body by a smoothly marginated mass in this patient with schwannoma. Axial and coronal non-contrast CT images demonstrate expansion of the T2 neuroforamen and erosion of the T2 vertebral body by a smoothly marginated mass in this patient with schwannoma. Axial and coronal non-contrast CT images demonstrate expansion of the T2 neuroforamen and erosion of the T2 vertebral body by a smoothly marginated mass in this patient with schwannoma.


29 T1 post-gadolinium MR image of this same patient with schwannoma demonstrate characteristic neuroforaminal expansion, vertebral body erosion, and avid enhancement. Regions of high T2 signal intensity as well as central non-enhancing component are also typical features for schwannoma. SCHWANNOMA MRI FINDINGS Axial T2-weighted MR image of this same patient with schwannoma demonstrate characteristic neuroforaminal expansion, vertebral body erosion, and avid enhancement. Regions of high T2 signal intensity as well as central non-enhancing component are also typical features for schwannoma. T1-weighted MR image of this same patient with schwannoma demonstrate characteristic neuroforaminal expansion, vertebral body erosion, and avid enhancement. Regions of high T2 signal intensity as well as central non-enhancing component are also typical features for schwannoma.


30 PERIPHERAL NERVE SHEATH TUMORS NEUROFIBROMAS Localized neurofibroma Most common form of neurofibroma (90%) Primarily affect superficial cutaneous nerves Slow growing Usually < 5 cm in size Peak presentation between 20 and 30 years of age Benign neoplasms composed of schwann cells and fibroblasts, containing a rich network of collagen fibers Key Imaging Features Unencapsulated, infiltrating between nerve fascicles May undergo malignant transformation to malignant peripheral nerve sheath tumor Anteroposterior and lateral chest radiographs of a patient with mediastinal neurofibromas demonstrate a smoothly lobulated mass in the aorticopulmonary window and widening of the left superior mediastinum.



31 NEUROFIBROMA IMAGING FINDINGS Axial contrast enhanced CT of this same patient with mediastinal neurofibromas demonstrates multiple conglomerate mediastinal masses.
 Half associated with NF1 May arise de novo or dedifferentiate from an existing peripheral nerve sheath")

32 PERIPHERAL NERVE SHEATH TUMORS MALIGNANT PERIPHERAL NERVE SHEATH TUMORS (MPNST) Account for 5-10% of all soft tissue sarcomas Metastasize hematogenously, frequently to the lungs Most are high grade tumors (85%) Half associated with NF1 May arise de novo or dedifferentiate from an existing peripheral nerve sheath tumor Key Imaging Features Malignant features: Large lesion (> 5 cm) Irregular borders Rapid growth on interval imaging Axial and coronal FDG PET/CT images of a a patient with MPNST demonstrate a large right chest wall mass with intense activity. Central area of decreased activity correspond to cystic and necrotic components.



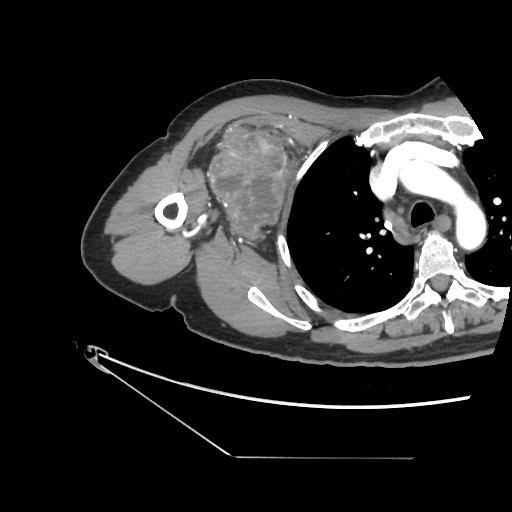
33 MALIGNANT PERIPHERAL NERVE SHEATH TUMOR CT FINDINGS Axial and coronal contrast-enhanced CT images of a patient with MPNST demonstrate a large, enhancing mass in the right chest wall with vascular and cystic components. Axial and coronal contrast-enhanced CT images of a patient with MPNST demonstrate a large, enhancing mass in the right chest wall with vascular and cystic components.








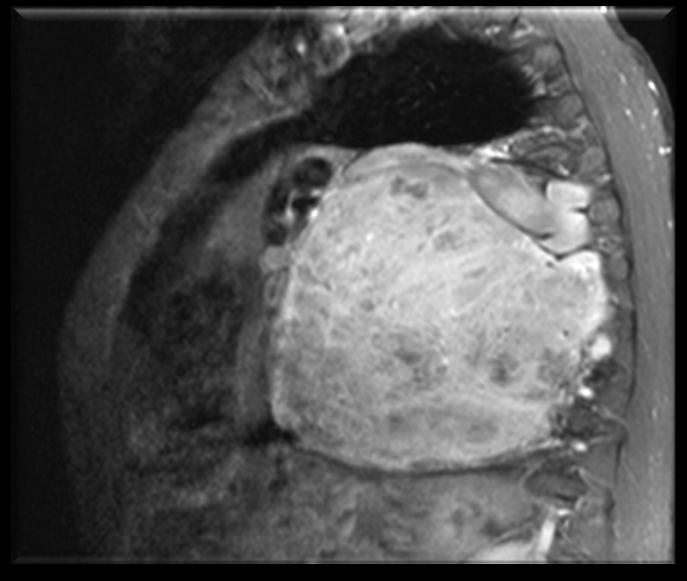
34 MALIGNANT PERIPHERAL NERVE SHEATH TUMOR MRI FINDINGS Coronal STIR demonstrates a heterogenous T2 signal mass along the right chest wall, which was greater than 5 cm with irregular borders Coronal T1 demonstrates a heterogenous T1 signal mass with areas of increased T1 signal likely due to hemorrhage, along the right chest wall, which was greater than 5 cm, with irregular borders Sagittal proton density demonstrates a heterogenous mass along the right chest wall Axial STIR demonstrates a heterogenous T2 signal mass with fluid-fluid levels along the right chest wall, which was greater than 5 cm with irregular borders Axial precontrast T1 non fat sat demonstrates a heterogenous T1 signal mass along the right chest wall Axial postcontrast T1 fat sat show avid heterogenous enhancement with areas of necrosis

35 NEUROFIBROMATOSIS TYPE 1 NERVE SHEATH TUMORS Autosomal dominant disorder with a frequency of 1 in Plexiform neurofibroma is pathognomonic Key Imaging Features Rib deformity Scoliosis Posterior scalloping of vertebral bodies from dural ectasia Thin-walled bullae, fibrosis Coronal T2-weighted MR image with fat saturation of a patient with neurofibromatosis type 1 shows multiple T2 hyperintense masses, many of which demonstrate low signal intensity centrally.
36 Mediastinal Mass (Superior or Posterior) Suspect neurogenic tumor Aggressive or non aggressive features Benign versus malignant Shape Imaging characteristics Age Plane of growth parallel to the spine Nerve sheath tumor T2 heterogenous internal signal intensity more commonly found in nerve sheath tumors Posteroanterior radiograph of a patient <15 years of agewith ganglioneuroma demonstrate a large mass in the posterior mediastinum. Plane of growth perpendicular to the spine ganglion cell tumor T2 homogenous signal intensity mass in the posterior mediastinm more consistent with a ganglion cell tumor Posteroanterior radiograph of a patient >15 years of age with schwannoma demonstrates a smoothly marginated, oval paraspinal mass.
37 Mediastinal Mass (Superior or Posterior) Suspect neurogenic tumor Aggressive or non aggressive features Benign versus malignant Shape Plane of growth parallel to the spine or perpendicular Imaging characteristics Heterogenous tumoral T2 signal, homogenous tumoral T2 signal Age Less than 15 years of age or greater than 15 years of age Plane of growth parallel to the spine Nerve sheath tumor Plane of growth perpendicular to the spine ganglion cell tumor Axial T2 non fat saturation image of the thorax demonstrates heterogenous internal signal intensity more commonly found in nerve sheath tumors Axial T2 non fat saturation image of the thorax demonstrates a more homogenous signal intensity mass in the posterior mediastinm more consistent with a ganglion cell tumor Posteroanterior radiograph of a patient <15 years of agewith ganglioneuroma demonstrate a large mass in the posterior mediastinum. Posteroanterior radiograph of a patient >15 years of age with schwannoma demonstrates a smoothly marginated, oval paraspinal mass.


38 SUMMARY Neurogenic tumors of the chest may be a diagnostic challenge both clinically and radiologically. A detailed anatomic understanding of the chest nervous system will serve as a foundation for evaluating these tumors. Attention to key imaging features on imaging will suggest neurogenic tumors in a differential diagnosis. The complementary features of imaging modalities, when used deliberately and protocolled appropriately, will further refine a differential diagnosis and ultimately improve patient care.
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Imaging Of Cystic Paravertebral Masses:
 Imaging Of Cystic Paravertebral Masses: Differential Diagnosis and Key Discriminators John P. Lichtenberger III, MD, Maj, USAF, MC Brent McCarragher, MD, CPT, USA John R. Dryden, MD, LT, USN P. Gabriel
Imaging Of Cystic Paravertebral Masses: Differential Diagnosis and Key Discriminators John P. Lichtenberger III, MD, Maj, USAF, MC Brent McCarragher, MD, CPT, USA John R. Dryden, MD, LT, USN P. Gabriel
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region.
 1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
1 THE THORACIC REGION DESCRIPTION: This is the part of the trunk, which is located between the root of the neck and the superior border of the abdominal region. SHAPE : T It has the shape of a truncated
Mediastinum and pericardium
 Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum and pericardium Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com The mediastinum: is the central compartment of the thoracic cavity surrounded by
Mediastinum It is a thick movable partition between the two pleural sacs & lungs. It contains all the structures which lie
 Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
Sectional Anatomy Quiz II
 Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Human Anatomy Biology 351
 nnnnn 1 Human Anatomy Biology 351 Exam #2 Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
nnnnn 1 Human Anatomy Biology 351 Exam #2 Please place your name on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Essentials of Clinical MR, 2 nd edition. 51. Primary Neoplasms
 51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
51. Primary Neoplasms As with spinal central canal neoplasms in other regions, those of the lumbar spine may be classified as extradural, intradural extramedullary, and medullary. If an extradural lesion
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
THE THORACIC WALL. Boundaries Posteriorly by the thoracic part of the vertebral column. Anteriorly by the sternum and costal cartilages
 THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces Superiorly by the suprapleural
THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces Superiorly by the suprapleural
Intercostal Muscles LO4
 Intercostal Muscles LO4 4 List the structures, from superficial to deep, in an intercostal space. Describe their relationships to each other, to the associated neurovascular bundle and to the pleural cavity.
Intercostal Muscles LO4 4 List the structures, from superficial to deep, in an intercostal space. Describe their relationships to each other, to the associated neurovascular bundle and to the pleural cavity.
Anatomy of the Thorax
 Anatomy of the Thorax A) THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces
Anatomy of the Thorax A) THE THORACIC WALL Boundaries Posteriorly by the thoracic part of the vertebral column Anteriorly by the sternum and costal cartilages Laterally by the ribs and intercostal spaces
Chapter 5: Other mediastinal structures. The Large Arteries. The Aorta. Ascending aorta
 Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
Chapter 5: Other mediastinal structures The Large Arteries The Aorta The aorta is the main arterial trunk of the systemic circulation and in the healthy state its wall contain a large amount of yellow
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments
 Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Done By : Rahmeh Alsukkar Date : 26 /10/2017 slide 23 The lobes in the right and left lungs are divided into segments,which called bronchopulmonary segments Each segmental bronchus passes to a structurally
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line
 L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
L 14 A B O R A T O R Y Thorax THORACIC WALL Identify the lines used in anatomical surface descriptions of the thorax. median line mid-axillary line mid-clavicular line Identify the surface landmarks of
Anatomy of thoracic wall
 Anatomy of thoracic wall Topographic Anatomy of the Thorax 1 Bones of Thoracic wall ribs 1-7"true" ribs -those which attach directly to the sternum true ribs actually attach to the sternum by means of
Anatomy of thoracic wall Topographic Anatomy of the Thorax 1 Bones of Thoracic wall ribs 1-7"true" ribs -those which attach directly to the sternum true ribs actually attach to the sternum by means of
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
THE GOOFY ANATOMIST QUIZZES
 THE GOOFY ANATOMIST QUIZZES 5. NERVES Q1. Which of the following classifications of the nervous systems is correct? A. The autonomic nervous system is composed of the brain, cranial nerves and spinal nerves.
THE GOOFY ANATOMIST QUIZZES 5. NERVES Q1. Which of the following classifications of the nervous systems is correct? A. The autonomic nervous system is composed of the brain, cranial nerves and spinal nerves.
STERNUM. Lies in the midline of the anterior chest wall It is a flat bone Divides into three parts:
 STERNUM Lies in the midline of the anterior chest wall It is a flat bone Divides into three parts: 1-Manubrium sterni 2-Body of the sternum 3- Xiphoid process The body of the sternum articulates above
STERNUM Lies in the midline of the anterior chest wall It is a flat bone Divides into three parts: 1-Manubrium sterni 2-Body of the sternum 3- Xiphoid process The body of the sternum articulates above
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Pathology of Mediastinal Tumors
 SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms
SAMO Meeting Lucerne 2009 Pathology of Mediastinal Tumors Alex Soltermann Most common lesions (adults) Clinical presentation 50% of the patients are asymptomatic, lesion discovered incidentally Symptoms
Dr. Pratik Mukherjee, MMed, FRCR Dr. Ashish Chawla, MD, ABR (USA) Khoo Teck Puat Hospital, Singapore
 Khoo Teck Puat Hospital, Singapore") Dr. Pratik Mukherjee, MMed, FRCR Dr. Ashish Chawla, MD, ABR (USA) Khoo Teck Puat Hospital, Singapore The authors declare no financial disclosures. To revisit the basics of approach to mediastinal masses
Dr. Pratik Mukherjee, MMed, FRCR Dr. Ashish Chawla, MD, ABR (USA) Khoo Teck Puat Hospital, Singapore The authors declare no financial disclosures. To revisit the basics of approach to mediastinal masses
NERVOUS SYSTEM ANATOMY
 INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
INTRODUCTION to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science
cardiac plexus is continuous with the coronary and no named branches pain from the heart and lungs
 Nerves of the Thoracic Region Nerve Source Branches Motor Sensory Notes cardiac plexus cardiac brs. of the vagus n. and cervical ; thoracic l nn. the heart and lungs cardiac, cervical cardiac, vagal vagus
Nerves of the Thoracic Region Nerve Source Branches Motor Sensory Notes cardiac plexus cardiac brs. of the vagus n. and cervical ; thoracic l nn. the heart and lungs cardiac, cervical cardiac, vagal vagus
Organisation of the nervous system
 Chapter1 Organisation of the nervous system 1. Subdivisions of the nervous system The nervous system is divided: i) Structurally The central nervous system (CNS) composed of the brain and spinal cord.
Chapter1 Organisation of the nervous system 1. Subdivisions of the nervous system The nervous system is divided: i) Structurally The central nervous system (CNS) composed of the brain and spinal cord.
The Heart & Pericardium Dr. Rakesh Kumar Verma Assistant Professor Department of Anatomy KGMU UP Lucknow
 The Heart & Pericardium Dr. Rakesh Kumar Verma Assistant Professor Department of Anatomy KGMU UP Lucknow Fibrous skeleton Dense fibrous connective tissue forms a structural foundation around AV & arterial
The Heart & Pericardium Dr. Rakesh Kumar Verma Assistant Professor Department of Anatomy KGMU UP Lucknow Fibrous skeleton Dense fibrous connective tissue forms a structural foundation around AV & arterial
Tumors of the posterior mediastinum, located in the paravertebral
 Technique of Thoracoscopic Resection of Posterior Mediastinal Tumors Michael F. Reed, MD Tumors of the posterior mediastinum, located in the paravertebral sulcus, account for about 25% of all mediastinal
Technique of Thoracoscopic Resection of Posterior Mediastinal Tumors Michael F. Reed, MD Tumors of the posterior mediastinum, located in the paravertebral sulcus, account for about 25% of all mediastinal
Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi. E mail: a.al E. mail:
 Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi E mail: a.al nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Branches of ophthalmic artery Muscles of face A spinal nerve Spinal
Spinal nerves and cervical plexus Prof. Abdulameer Al Nuaimi E mail: a.al nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Branches of ophthalmic artery Muscles of face A spinal nerve Spinal
Tumors. Chapter 3. Primary neurogenic tumors. Tumors 27
 Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
[ANATOMY #12] April 28, 2013
![[ANATOMY #12] April 28, 2013](/thumbs/86/93473883.jpg "[ANATOMY #12] April 28, 2013") Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Sympathetic chain : Sympathetic chain is each of the pair of ganglionated longitudinal cords of the sympathetic nervous system; extend from level of atlas (base of skull) till coccyx. It is paravertebral
Yara saddam & Dana Qatawneh. Razi kittaneh. Maher hadidi
 1 Yara saddam & Dana Qatawneh Razi kittaneh Maher hadidi LECTURE 10 THORAX The thorax extends from the root of the neck to the abdomen. The thorax has a Thoracic wall Thoracic cavity and it is divided
1 Yara saddam & Dana Qatawneh Razi kittaneh Maher hadidi LECTURE 10 THORAX The thorax extends from the root of the neck to the abdomen. The thorax has a Thoracic wall Thoracic cavity and it is divided
Radiological Anatomy of Thorax. Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem
 Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Radiological Anatomy of Thorax Dr. Jamila Elmedany & Prof. Saeed Abuel Makarem Indications for Chest x - A chest x-ray may be used to diagnose and plan treatment for various conditions, including: Diseases/Fractures
Diaphragm and intercostal muscles. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Diaphragm and intercostal muscles Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skeletal System Adult Human contains 206 Bones 2 parts: Axial skeleton (axis): Skull, Vertebral column,
Diaphragm and intercostal muscles Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skeletal System Adult Human contains 206 Bones 2 parts: Axial skeleton (axis): Skull, Vertebral column,
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Superior and Posterior Mediastinum. Assoc. Prof. Jenny Hayes
 Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
Superior and Posterior Mediastinum Assoc. Prof. Jenny Hayes WARNING This material has been provided to you pursuant to section 49 of the Copyright Act 1968 (the Act) for the purposes of research or study.
The posterior abdominal wall. Prof. Oluwadiya KS
 The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
The posterior abdominal wall Prof. Oluwadiya KS www.oluwadiya.sitesled.com Posterior Abdominal Wall Lumbar vertebrae and discs. Muscles opsoas, quadratus lumborum, iliacus, transverse, abdominal wall
NERVOUS SYSTEM ANATOMY
 NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering
NTRODUCTON to NERVOUS SYSTEM ANATOMY M1 - Gross and Developmental Anatomy Dr. Milton M. Sholley Professor of Anatomy and Neurobiology and Dr. Michael H. Peters Professor of Chemical and Life Science Engineering
1 Normal Anatomy and Variants
 1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
1 Normal Anatomy and Variants 1.1 Normal Anatomy MR Technique. e standard MR protocol for a routine evaluation of the spine always comprises imaging in sagittal and axial planes, while coronal images are
THE SURGEON S LIBRARY
 THE SURGEON S LIBRARY THE HISTORY AND SURGICAL ANATOMY OF THE VAGUS NERVE Lee J. Skandalakis, M.D., Chicago, Illinois, Stephen W. Gray, PH.D., and John E. Skandalakis, M.D., PH.D., F.A.C.S., Atlanta, Georgia
THE SURGEON S LIBRARY THE HISTORY AND SURGICAL ANATOMY OF THE VAGUS NERVE Lee J. Skandalakis, M.D., Chicago, Illinois, Stephen W. Gray, PH.D., and John E. Skandalakis, M.D., PH.D., F.A.C.S., Atlanta, Georgia
2. right heart = pulmonary pump takes blood to lungs to pick up oxygen and get rid of carbon dioxide
 A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
A. location in thorax, in inferior mediastinum posterior to sternum medial to lungs superior to diaphragm anterior to vertebrae orientation - oblique apex points down and to the left 2/3 of mass on left
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
Group of students. - Rawan almujabili د. محمد المحتسب - 1 P a g e
 - 14 - Group of students - Rawan almujabili د. محمد المحتسب - 1 P a g e Nerves of the posterior abdominal wall The spinal cord gives off spinal nerves between the vertebrae. In the abdomen, through the
- 14 - Group of students - Rawan almujabili د. محمد المحتسب - 1 P a g e Nerves of the posterior abdominal wall The spinal cord gives off spinal nerves between the vertebrae. In the abdomen, through the
Classification of the nervous system. Prof. Dr. Nikolai Lazarov 2
 1 1. Formation and general organization 2. Spinal ganglia 3. Zonal and segmental innervation 4. Dorsal rami of the spinal nerves 5. Ventral rami of the spinal nerves 6. Cervical plexus Classification of
1 1. Formation and general organization 2. Spinal ganglia 3. Zonal and segmental innervation 4. Dorsal rami of the spinal nerves 5. Ventral rami of the spinal nerves 6. Cervical plexus Classification of
Chest and cardiovascular
 Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Module 1 Chest and cardiovascular A. Doss and M. J. Bull 1. Regarding the imaging modalities of the chest: High resolution computed tomography (HRCT) uses a slice thickness of 4 6 mm to identify mass lesions
Paraspinal Venous Malformation Joseph Junewick, MD FACR
 Paraspinal Venous Malformation Joseph Junewick, MD FACR 06/04/2010 History 2 year old with history of fall. Rule out spinal injury. Diagnosis Paraspinal Venous Malformation Additional Clinical CT of the
Paraspinal Venous Malformation Joseph Junewick, MD FACR 06/04/2010 History 2 year old with history of fall. Rule out spinal injury. Diagnosis Paraspinal Venous Malformation Additional Clinical CT of the
The Heart. The Heart A muscular double pump. The Pulmonary and Systemic Circuits
 C H A P T E R 19 The Heart The Heart A muscular double pump circuit takes blood to and from the lungs Systemic circuit vessels transport blood to and from body tissues Atria receive blood from the pulmonary
C H A P T E R 19 The Heart The Heart A muscular double pump circuit takes blood to and from the lungs Systemic circuit vessels transport blood to and from body tissues Atria receive blood from the pulmonary
Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th & 12 th Eds.)
") PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
Intrathoracic neural tumours
 Intrathoracic neural tumours K. G. DAVIDSON, P. R. WALBAUM, AND R. J. M. McCORMACK From the Thoracic Surgery Department, City Hospital, Edinburgh, UK Thorax, 1978, 33, 359-367 Davidson, K. G., Walbaum,
Intrathoracic neural tumours K. G. DAVIDSON, P. R. WALBAUM, AND R. J. M. McCORMACK From the Thoracic Surgery Department, City Hospital, Edinburgh, UK Thorax, 1978, 33, 359-367 Davidson, K. G., Walbaum,
Autonomic Nervous System. Ms. DS Pillay Room 2P24
 Autonomic Nervous System Ms. DS Pillay Room 2P24 OVERVIEW OF THE NERVOUS SYSTEM NERVOUS SYSTEM CNS PNS BRAIN SPINAL CORD SOMATIC ANS SYMPATHEIC PARASYMPATHEIC LOCATION OF GANGLIA IN THE ANS Short post-ganglionic
Autonomic Nervous System Ms. DS Pillay Room 2P24 OVERVIEW OF THE NERVOUS SYSTEM NERVOUS SYSTEM CNS PNS BRAIN SPINAL CORD SOMATIC ANS SYMPATHEIC PARASYMPATHEIC LOCATION OF GANGLIA IN THE ANS Short post-ganglionic
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW
 INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D.
 Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D. Chest cavity - bony structures Chest cavity- bony structures Sternum Ribs True ribs: first seven pairs connect
Chest cavity, vertebral column and back muscles. Respiratory muscles. Sándor Katz M.D., Ph.D. Chest cavity - bony structures Chest cavity- bony structures Sternum Ribs True ribs: first seven pairs connect
Case 9087 Retropharyngeal nodular fasciitis
 Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
Case 9087 Retropharyngeal nodular fasciitis Santiago I 1; Cavalheiro F 2; Noruégas MJ 3; Sanches MC3 1 Hospital Infante D. Pedro, Aveiro, Portugal 2 Hospitais da Universidade de Coimbra, Portugal 3 Hospital
thoracic cage inlet and outlet landmarks of the anterior chest wall muscles of the thoracic wall sternum joints ribs intercostal spaces diaphragm
 Thoracic Wall Lecture Objectives Describe the shape and outline of the thoracic cage including inlet and outlet. Describe the anatomical landmarks of the anterior chest wall. List various structures making
Thoracic Wall Lecture Objectives Describe the shape and outline of the thoracic cage including inlet and outlet. Describe the anatomical landmarks of the anterior chest wall. List various structures making
Chapter 3: Thorax. Thorax
 Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
Chapter 3: Thorax Thorax Thoracic Cage I. Thoracic Cage Osteology A. Thoracic Vertebrae Basic structure: vertebral body, pedicles, laminae, spinous processes and transverse processes Natural kyphotic shape,
e-anatomy Paper 2 Exam Monday, 4 April 2016
 e-anatomy Paper 2 Exam Monday, 4 Level 9, 51 Druitt Street, Sydney NSW 2000, Australia Ph: +61 2 9268 9777 Fax: +61 2 9268 9799 Web: www.ranzcr.edu.au Email: ranzcr@ranzcr.edu.au ABN 37 000 029 863 CASE
e-anatomy Paper 2 Exam Monday, 4 Level 9, 51 Druitt Street, Sydney NSW 2000, Australia Ph: +61 2 9268 9777 Fax: +61 2 9268 9799 Web: www.ranzcr.edu.au Email: ranzcr@ranzcr.edu.au ABN 37 000 029 863 CASE
Imaging of Thoracic Neurogenic
 Cardiopulmonary Imaging Review Pavlus et al. Imaging of Thoracic Neurogenic Tumors Cardiopulmonary Imaging Review John D. Pavlus 1 rett W. Carter 2 Marc D. Tolley 3 Elaine S. Keung 4 Leila Khorashadi 5
Cardiopulmonary Imaging Review Pavlus et al. Imaging of Thoracic Neurogenic Tumors Cardiopulmonary Imaging Review John D. Pavlus 1 rett W. Carter 2 Marc D. Tolley 3 Elaine S. Keung 4 Leila Khorashadi 5
Anterior Mediastinal Masses: The 4 T s
 May 2001 Anterior Mediastinal Masses: The 4 T s Rachel Van Sambeek, Harvard Medical School, Year III 1 Mediastinal Compartments 3 arbitrary divisions that do not correlate with anatomic planes: Anterior
May 2001 Anterior Mediastinal Masses: The 4 T s Rachel Van Sambeek, Harvard Medical School, Year III 1 Mediastinal Compartments 3 arbitrary divisions that do not correlate with anatomic planes: Anterior
Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions
 Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
Original Research Article Imaging in neurofibromatosis type 1: An original research article with focus on spinal lesions Kalpesh Patel 1*, Siddharth Zala 2, C. Raychaudhuri 3 1 Assistant Professor, 2 1
Note : I put the sheet's info within the slides to easily understand this lecture Done by : Zaid Al-Ghnaneem
 Note : I put the sheet's info within the slides to easily understand this lecture Done by : Zaid Al-Ghnaneem Thoracic Wall Lecture Objectives Describe the shape and outline of the thoracic cage including
Note : I put the sheet's info within the slides to easily understand this lecture Done by : Zaid Al-Ghnaneem Thoracic Wall Lecture Objectives Describe the shape and outline of the thoracic cage including
Vasculature and innervation of the heart. A. Bendelic Human Anatomy Department
 Vasculature and innervation of the heart A. Bendelic Human Anatomy Department Plan: 1. Arterial blood supply of the heart. Coronary arteries 2. Venous drainage of the heart. Cardiac veins 3. Innervation
Vasculature and innervation of the heart A. Bendelic Human Anatomy Department Plan: 1. Arterial blood supply of the heart. Coronary arteries 2. Venous drainage of the heart. Cardiac veins 3. Innervation
Basic Data. Sex:Male 31 years old Occupation: 搬家工人
 Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Basic Data Sex:Male 31 years old Occupation: 搬家工人 Chief Complaint Intermittent chest pain with shortness of breath for 2-3 months. Present Illness 4 months ago, he started having occasional chest pain
Sheet. April/14 th /2013. Introduction to Anatomy. Dr. Maher Hadidi. Muna Abu Hijleh. 1 P a g e
 Sheet Introduction to Anatomy Dr. Maher Hadidi Muna Abu Hijleh 1 P a g e 29 April/14 th /2013 Superior & Posterior Mediastinum ***Superior mediastinum * is bounded from: -Anterior by manubrium sterni -posterior
Sheet Introduction to Anatomy Dr. Maher Hadidi Muna Abu Hijleh 1 P a g e 29 April/14 th /2013 Superior & Posterior Mediastinum ***Superior mediastinum * is bounded from: -Anterior by manubrium sterni -posterior
Nerves on the Posterior Abdominal Wall
 Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
Nerves on the Posterior Abdominal Wall Lumbar Plexus The lumbar plexus, which is one of the main nervous pathways supplying the lower limb, is formed in the psoasmuscle from the anterior ramiof the upper
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
1/9/2013 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE. Introduction. Classification for Extramedullary Tumors
 EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
EXTRAMEDULLARY TUMORS OF THE PEDIATRIC SPINE Eugene Wang 1/20/12 Dent Neurologic Institute Introduction 2/3 of all intraspinal tumors of childhood are extramedullary 50% Extradural 10-15% Intradural Back
Presacral Neuroblastoma Joseph Junewick, MD FACR
 Presacral Neuroblastoma Joseph Junewick, MD FACR 01/12/2010 History 16 month old male with irritability. Diagnosis Presacral Neuroblastoma Additional Clinical Initial US to evaluate for intussusception
Presacral Neuroblastoma Joseph Junewick, MD FACR 01/12/2010 History 16 month old male with irritability. Diagnosis Presacral Neuroblastoma Additional Clinical Initial US to evaluate for intussusception
In the Last Three Lectures We Already Discussed the Importance of the Thoracic Cage.
 -This Lecture Will Revise what we took in the last three lectures and will introduce the concept of the chest cavity ( Thoracic Cavity ) In the Last Three Lectures We Already Discussed the Importance of
-This Lecture Will Revise what we took in the last three lectures and will introduce the concept of the chest cavity ( Thoracic Cavity ) In the Last Three Lectures We Already Discussed the Importance of
Ex. 1 :Language of Anatomy
 Collin College BIOL 2401 : Human Anatomy & Physiology Ex. 1 :Language of Anatomy The Anatomical Position Used as a reference point when referring to specific areas of the human body Body erect Head and
Collin College BIOL 2401 : Human Anatomy & Physiology Ex. 1 :Language of Anatomy The Anatomical Position Used as a reference point when referring to specific areas of the human body Body erect Head and
A Journey Down The Canal
 A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
A Journey Down The Canal Radiological Assessment of Spinal Cord Masses John Berry-Candelario HMS III Gillian Lieberman, MD BIDMC Objectives Patient review Anatomy of the spine Imaging techniques Classification
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY. Guidelines. Module 2 Topic of the lesson Aorta. Thoracic aorta.
 BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY Guidelines Academic discipline HUMAN ANATOMY Module 2 Topic of the lesson Aorta. Thoracic aorta. Course 1 The number of hours 3 1. The
BOGOMOLETS NATIONAL MEDICAL UNIVERSITY DEPARTMENT OF HUMAN ANATOMY Guidelines Academic discipline HUMAN ANATOMY Module 2 Topic of the lesson Aorta. Thoracic aorta. Course 1 The number of hours 3 1. The
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji
 Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
Neckmasses in infancy and childhood: Clinical and radiological classification and imaging approaches M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Neck masses are a frequent
PLEURAE and PLEURAL RECESSES
 PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
Synapse Homework. Back page last question not counted. 4 pts total, each question worth 0.18pts. 26/34 students answered correctly!
 Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Synapse Homework Back page last question not counted 26/34 students answered correctly! 4 pts total, each question worth 0.18pts Business TASS hours extended! MWF 1-2pm, Willamette 204 T and Th 9:30-10:30am,
Sympathetic Nervous System
 Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
Sympathetic Nervous System Lecture Objectives Review the subdivisions of the nervous system. Review the general arrangement and compare the sympathetic and parasympathetic parts. Describe the following
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Theme 30. Structure, topography and function of the lungs and pleura. Mediastinum and its contents. X -ray films digestive and respiratory systems.
 Theme 30. Structure, topography and function of the lungs and pleura. Mediastinum and its contents. X -ray films digestive and respiratory systems. STRUCTURE, TOPOGRAPHY AND FUNCTІON OF LUNGS AND PLEURA.
Theme 30. Structure, topography and function of the lungs and pleura. Mediastinum and its contents. X -ray films digestive and respiratory systems. STRUCTURE, TOPOGRAPHY AND FUNCTІON OF LUNGS AND PLEURA.
Anatomy Lecture 8. In the previous lecture we talked about the lungs, and their surface anatomy:
 Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Anatomy Lecture 8 In the previous lecture we talked about the lungs, and their surface anatomy: 1-Apex:it lies 1 inch above the medial third of clavicle. 2-Anterior border: it starts from apex to the midpoint
Bronchioles. Alveoli. Type I alveolar cells are very thin simple squamous epithelial cells and form most of the lining of an alveolus.
 276 Bronchioles Bronchioles continue on to form bronchi. The primary identifying feature is the loss of hyaline cartilage. The epithelium has become simple ciliated columnar, and there is a complete ring
276 Bronchioles Bronchioles continue on to form bronchi. The primary identifying feature is the loss of hyaline cartilage. The epithelium has become simple ciliated columnar, and there is a complete ring
Mediastinum. Respiratory block-anatomy-lecture 6. Editing file
 Mediastinum Respiratory block-anatomy-lecture 6 Editing file Objectives At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum.
Mediastinum Respiratory block-anatomy-lecture 6 Editing file Objectives At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum.
Human Anatomy, First Edition
 Human Anatomy, First Edition McKinley & O'Loughlin Chapter 22 : Heart 1 Functions of the Heart Center of the cardiovascular system, the heart. Connects to blood vessels that transport blood between the
Human Anatomy, First Edition McKinley & O'Loughlin Chapter 22 : Heart 1 Functions of the Heart Center of the cardiovascular system, the heart. Connects to blood vessels that transport blood between the
Retroperitoneal Sarcomas - A pictorial review
 Retroperitoneal Sarcomas - A pictorial review Poster No.: C-1409 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Douraghi-Zadeh, K. L. Shahabuddin, R. H. Thomas, E. Moskovic; London/UK Keywords:
Retroperitoneal Sarcomas - A pictorial review Poster No.: C-1409 Congress: ECR 2013 Type: Educational Exhibit Authors: D. Douraghi-Zadeh, K. L. Shahabuddin, R. H. Thomas, E. Moskovic; London/UK Keywords:
Cardiovascular system:
 Cardiovascular system: Mediastinum: The mediastinum: lies between the right and left pleura and lungs. It extends from the sternum in front to the vertebral column behind, and from the root of the neck
Cardiovascular system: Mediastinum: The mediastinum: lies between the right and left pleura and lungs. It extends from the sternum in front to the vertebral column behind, and from the root of the neck
Objectives. Thoracic Inlet. Thoracic Inlet Boundaries. Thoracic Inlet Sagittal View ANTERIOR SCALENE ANTERIOR SCALENE
 Objectives Thoracic Inlet Deborah L. Reede M.D. SUNY Downstate Medical Center Learn the anatomy of the thoracic inlet (TI) Review the clinical and radiographic findings of common lesions encountered in
Objectives Thoracic Inlet Deborah L. Reede M.D. SUNY Downstate Medical Center Learn the anatomy of the thoracic inlet (TI) Review the clinical and radiographic findings of common lesions encountered in
Welcome to the Structure & Development Dissector. Section I
 Welcome to the Structure & Development Dissector The vast majority of questions will be drawn from structures present in the checklist; however, we reserve the right to use a structure or two that is not
Welcome to the Structure & Development Dissector The vast majority of questions will be drawn from structures present in the checklist; however, we reserve the right to use a structure or two that is not
11.1 The Aortic Arch General Anatomy of the Ascending Aorta and the Aortic Arch Surgical Anatomy of the Aorta
 456 11 Surgical Anatomy of the Aorta 11.1 The Aortic Arch 11.1.1 General Anatomy of the Ascending Aorta and the Aortic Arch Surgery of the is one of the most challenging areas of cardiac and vascular surgery,
456 11 Surgical Anatomy of the Aorta 11.1 The Aortic Arch 11.1.1 General Anatomy of the Ascending Aorta and the Aortic Arch Surgery of the is one of the most challenging areas of cardiac and vascular surgery,
nerve blocks in the diagnosis and therapy of visceral disease
 Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
Visceral Pain nerve blocks in the diagnosis and therapy of visceral disease Guy Hans, MD, PhD Dept. of Anesthesiology, Multidisciplinary Pain Center Visceral Pain? Type of nociceptive pain (although often
Dana Alrafaiah. - Moayyad Al-Shafei. -Mohammad H. Al-Mohtaseb. 1 P a g e
 - 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
- 6 - Dana Alrafaiah - Moayyad Al-Shafei -Mohammad H. Al-Mohtaseb 1 P a g e Quick recap: Both lungs have an apex, base, mediastinal and costal surfaces, anterior and posterior borders. The right lung,
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Neuroblastoma Joseph Junewick, MD FACR
 Neuroblastoma Joseph Junewick, MD FACR 03/18/2011 History 15 month old with anemia. Diagnosis Neuroblastoma Discussion Neuroblastic tumors derive from primordial neural crest cells destined for sympathetic
Neuroblastoma Joseph Junewick, MD FACR 03/18/2011 History 15 month old with anemia. Diagnosis Neuroblastoma Discussion Neuroblastic tumors derive from primordial neural crest cells destined for sympathetic
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Chapter 20 (1) The Heart
 The Heart") Chapter 20 (1) The Heart Learning Objectives Describe the location and structure of the heart Describe the path of a drop of blood from the superior vena cava or inferior vena cava through the heart out
Chapter 20 (1) The Heart Learning Objectives Describe the location and structure of the heart Describe the path of a drop of blood from the superior vena cava or inferior vena cava through the heart out
Open surgery for posterior mediastinal neurogenic tumors
 Review Article Page 1 of 5 Open surgery for posterior mediastinal neurogenic tumors Erkan Kaba 1, Mazen Rasmi Alomari 2, Alper Toker 2 1 Department of Thoracic Surgery, Istanbul Bilim University Medical
Review Article Page 1 of 5 Open surgery for posterior mediastinal neurogenic tumors Erkan Kaba 1, Mazen Rasmi Alomari 2, Alper Toker 2 1 Department of Thoracic Surgery, Istanbul Bilim University Medical