Incidence of ductal lesions
|
|
|
- Godwin Burke
- 6 years ago
- Views:
Transcription


 London, Connolly, Schnitt and Colditz: JAMA 1992 Breast Cancer Detection Demonstration Project")
1 Ductal Proliferative Lesions of the Breast: From FEA to ADH to DCIS Incidence of ductal lesions Pre-mammography: DCIS < 3% of breast cancers, large palpable masses, with invasion Mammography: DCIS 25% of newly diagnosed breast cancers in US, most non-palpable Yunn-Yi Chen, MD, PhD Department of Pathology, UCSF Concurrent prevalence of ADH and FEA: ADH: 2.1% to 10% FEA: < 1% (not recognized) to 3.6% Outline Conventional intraductal proliferative lesions Distinguish UDH from ADH and low-grade DCIS Clinical significance and management FEA Distinguish various columnar cell lesions Clinical significance of FEA Management for FEA Studies addressing benign breast disease (BBD) and breast cancer risk using criteria by Page et al Nashville Breast Cohort Dupont and Page: N Engl J Med 1985 Nurses Health Study (NHS) London, Connolly, Schnitt and Colditz: JAMA 1992 Breast Cancer Detection Demonstration Project (BCDDP) Dupont, Parl, Hartmann, et al: Cancer 1993 Mayo Clinic Hartmann, Sellers, Frost, et al: N Engl J Med

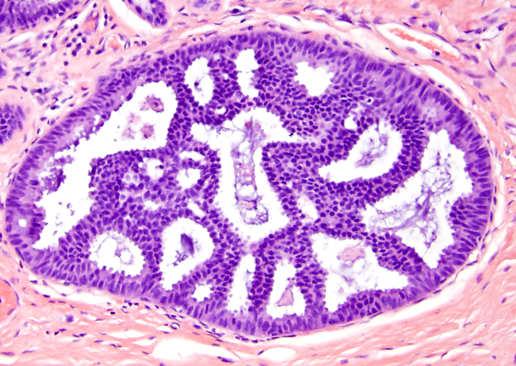
 Architectural features Irregular, peripheral fenestrations")
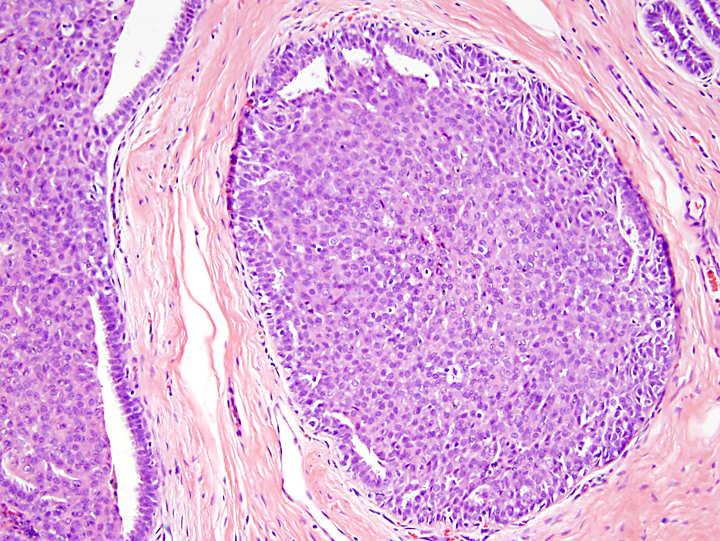
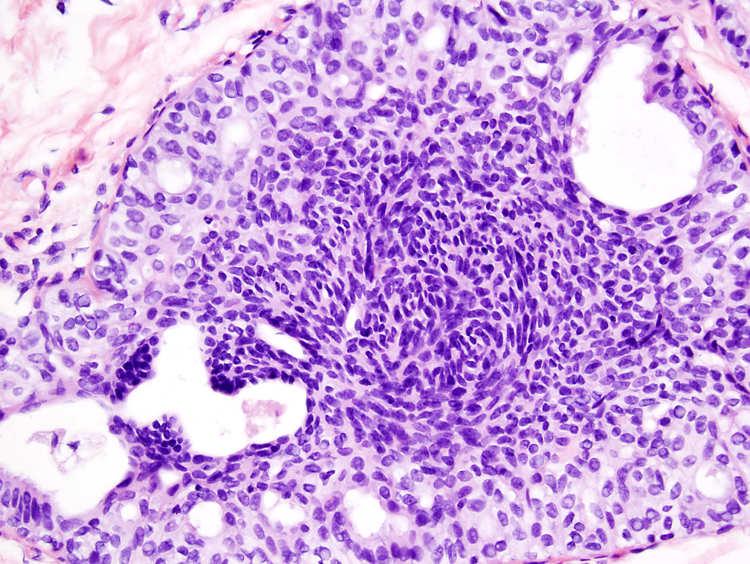
2 Breast diseases and risk of invasive ca Diagnosis of ductal proliferative lesions: Architecture and Cytology Nonproliferative lesions: no increased risk mild hyperplasia (< 4-cell layers), cysts, apocrine change, duct ectasia, simple FA, mastitis Proliferative lesions without atypia: 1.5-2x risk moderate to florid UDH, sclerosing adenosis, complex FA, papilloma, radial scar Atypical hyperplasia (ADH, ALH): 4-5x risk Low-grade DCIS and LCIS: 8-10x risk Page D, Rogers L. Hum Pathol 1992;23: WHO classification of tumors of the breast and female genital organs 2003 Histologic criteria for UDH (WHO 2003) Architectural features Irregular, peripheral fenestrations Stretched or twisted epithelial bridges Streaming or whirling Uneven distribution of nuclei and overlapped nuclei Cytologic features Multiple cell types Variation in size and shape of cells/nuclei Indistinct cell margins and deviation from a round contour 2
3 3
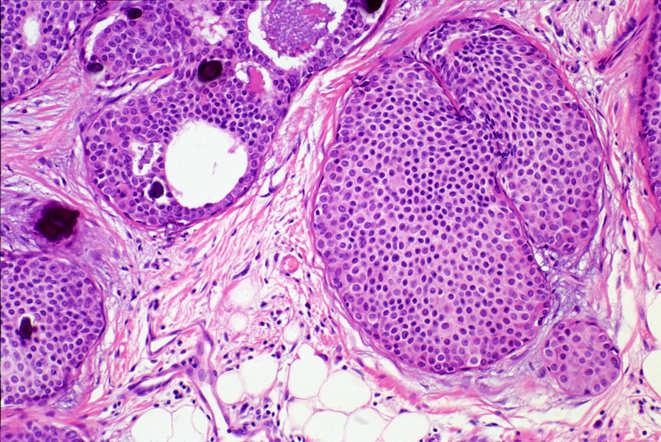
 Cytologic features Monomorphic rounded cell population Evenly spaced")


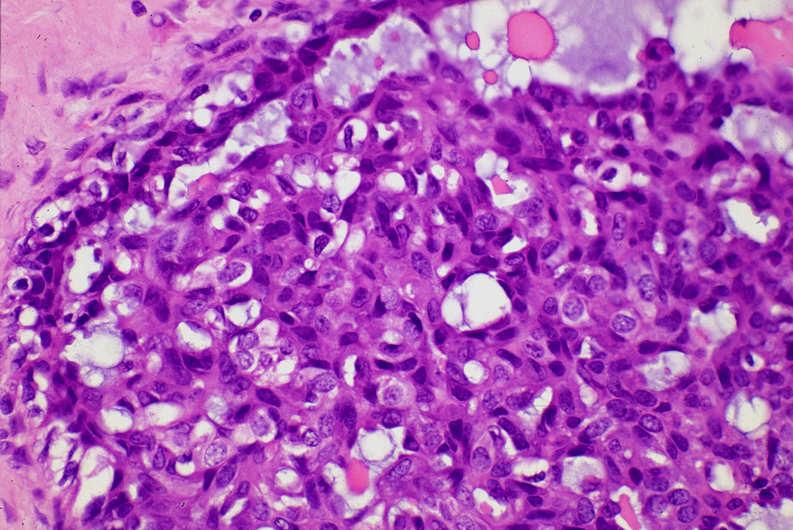
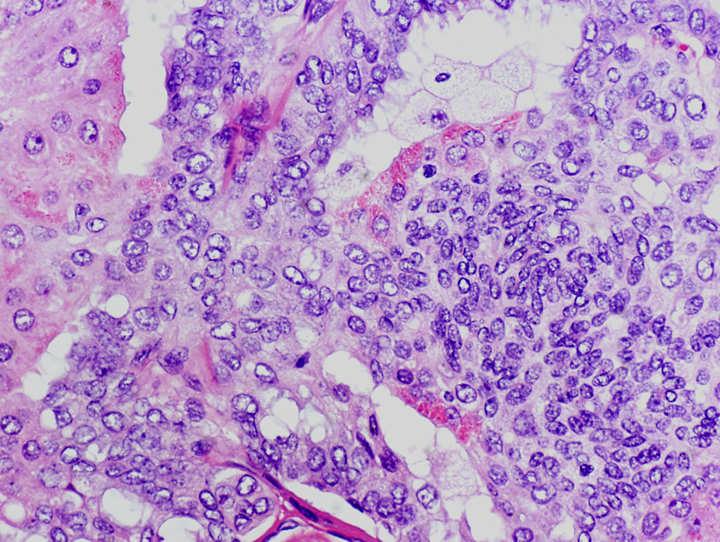
4 Necrosis may rarely be seen in UDH Histologic criteria for low-grade DCIS (WHO 2003) Cytologic features Monomorphic rounded cell population Evenly spaced with distinct cell borders Oval to round nuclei, ± hyperchromasia Equidistant or highly organized nuclear distribution Architectural features Arcades, cribriform, solid, and/or micropapillary Size/extent criteria: 2 ducts or 2 mm Cytologic features of LG DCIS Monotonous Round to oval nuclei Distinct cell membrane 4




5 Cytologic features of LG DCIS Highly organized nuclear distribution: polarization to lumen DCIS--architectural pattern cribriform DCIS--architectural pattern Roman arch/bridge DCIS--architectural pattern solid 5






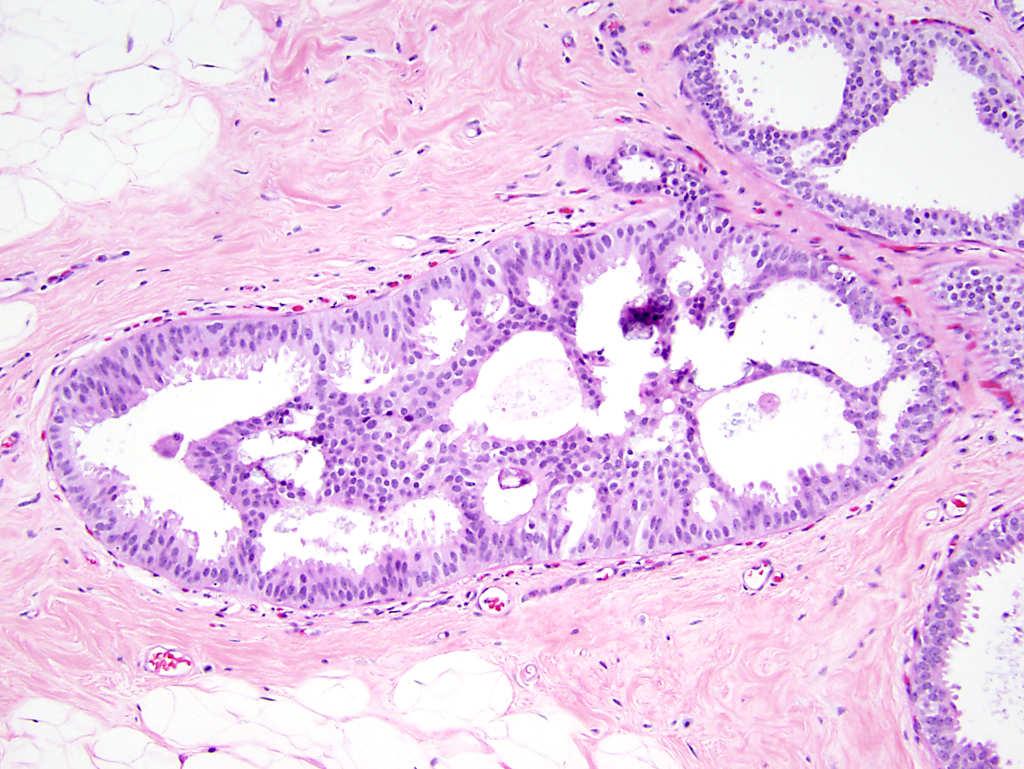
6 DCIS--architectural pattern micropapillary DCIS UDH Monotonous Evenly spaced Distinct cell membrane Heterogeneous Crowded and overlapping Indistinct cell membrane DCIS UDH Micropapillary DCIS Micropapillary hyperplasia Rigid bar Nuclei perpendicular to bar Tapering bar Nuclei parallel to bar Papillae: Narrow base Bulbous tip Papillae: Broad base Pointed or tapering tip 6


7 Micropapillary DCIS Micropapillary hyperplasia Atypical ductal hyperplasia (Page and Rogers, 1992) Partial involvement of the duct by a cell population of the type defined for LG DCIS Diagnostic criteria imperfect, based on exclusion rather than positive criteria Monotonous population Hyperchromatic Organized: nuclei perpendicular to lumen Heterogeneous population Hyperchromatic at tip, normochromatic at base Crowded and overlapping nuclei Histologic criteria for ADH-- two categories Qualitatively insufficient for DCIS: mimic DCIS partial involvement of duct by atypical cells; or architectural atypia insufficient Quantitatively insufficient for DCIS: mini DCIS characteristic cytologic and architectural atypia, but aggregate diameter < 2 mm 7


8 8
9 Interobserver reproducibility in the diagnosis of ductal proliferative breast lesions using standardized criteria S. Schnitt et al AJSP 16: , 1992 Six breast pathologists /c 24 proliferative ductal lesions; classify as UDH, AH, CIS Written & diagrammatic summary of diagnostic criteria (D. Page) and a set of 15 teaching slides 14 cases (58%): complete agreement 17 cases (71%): 5 or more agreed 22 cases (92%): 4 or more agreed Approach to borderline ductal lesions Epithelial proliferation and atypia: morphologic and molecular continuum Distinction between ADH and LG DCIS not clear-cut, cut-off arbitrary When in doubt (between ADH and DCIS), the more benign diagnosis is appropriate (ADH) For borderline lesion, suggest conservative approach, recommend clinical follow-up Marker: distinguishing UDH from LG DCIS? HMW-CK in ductal lesions ER Ki67 Cyclin D1 CK5/6, 34βE12, CK14, CK17 UDH: HMWK + ADH/DCIS: HMWK (rare exception) HMW-CK 9








10 Florid usual ductal hyperplasia Atypical ductal hyperplasia CK5/6 CK5/6 High grade basal-like DCIS Problematic DCIS lesions Intermediate grade DCIS DCIS with spindle cells Papillary and solid/papillary DCIS To be discussed in another lecture CK5/6 10




11 Intermediate grade DCIS may mimic UDH Intermediate grade DCIS CK5/6 Intermediate grade DCIS DCIS with spindle cells: mimic of UDH CK5/6 11




12 DCIS with spindle cells High grade DCIS Dx of high grade DCIS: based on cytologic features No minimal size required CK5/6 Clinical significance & management for DCIS Clinical significance & management for ADH Relative risk of cancer: 8-10X Subsequent invasive cancer occurs in same area of breast Precursor to invasive ca Surgical excision with negative margin adjuvant XRT in patients with breast conservation Hormonal therapy if hormone receptor positive Relative risk of cancer: 4-5X Risk may be further increased in premenopausal women and those with a firstdegree relative with breast cancer Subsequent cancer bilateral 12
 and flat epithelial atypia (FEA): classification, diagnostic criteria Distinguishing FEA")
13 Clinical significance & management for ADH Non-obligate precursor to invasive ca, risk factor for breast ca Excision recommended if found on CNB 33-87% upgraded to ca No features reliably predictive of upgrade Close follow-up if found on excision Flat epithelial atypia--outline Columnar cell lesions (CCL) and flat epithelial atypia (FEA): classification, diagnostic criteria Distinguishing FEA from ADH and other mimics Clinical features and biology Management Columnar cell lesions (CCLs) Classification of CCLs-- Based on cytologic atypia A spectrum of lesions with cuboidal to columnar epithelial cells lining variably dilated TDLUs Ranging from little or no cytologic or architectural atypia to ADH or DCIS Have long been recognized with various names Increasingly encountered due to mammographic calcifications No cytologic atypia Columnar cell change (CCC) Columnar cell hyperplasia (CCH) With cytologic atypia Flat epithelial atypia (FEA) Consensus terminology by Stuart and WHO 13




14 Columnar cell lesions-- Histologic features Columnar cell change/hyperplasia-- Histologic features CCC: 1-2 cell layers A spectrum of lesions: TDLUs with variably dilated acini Acini lined by cuboidal to columnar cells, often with apical snouts ± luminal secretions CCH: 3-5 cell layers; may form tufts, but complex architectural patterns are absent Ovoid to elongated nuclei oriented perpendicular to basement membrane; nucleoli absent or inconspicuous ± microcalcifications, may be psamommatous Columnar cell change Columnar cell change 14
 TDLUs usually bluer and rounder at low power")


15 Columnar cell change Columnar cell hyperplasia Flat epithelial atypia-- Histologic features (I) TDLUs usually bluer and rounder at low power Acini lined by low-grade (monomorphic type) mildly atypical cells, similar to those seen in low grade DCIS and tubular ca Round to oval nuclei; nucleoli may or may not be prominent Nuclear chromatin either finely dispersed or slightly clumping and marginated (Source: Stuart and Vincent-Salomon 2003) 15
 Flat epithelial atypia Nuclei lack")


 Flat growth pattern")
 Flat")
16 Flat epithelial atypia-- Histologic features (II) Flat epithelial atypia Nuclei lack polarity and are not regularly oriented perpendicular to basement membrane some cases: stratified, tall ovoid to fusiform hyperchromatic nuclei perpendicular to basement membrane (colonic adenoma-like or endometrioid appearance) Flat growth pattern (no complex architectural patterns) (Source: Stuart and Vincent-Salomon 2003) Flat epithelial atypia Flat epithelial atypia 16






17 Flat epithelial atypia Flat epithelial atypia-- adenoma-like or endometrioid CCC Cytologic features in CLL FEA CCH Diagnosis of FEA Subjective evaluation of cytologic features Diagnostic challenge Problem with lowest threshold 17


18 Role of IHC in evaluation of CCL? Columnar cell lesions HMW-CK: negative in CCL irrespective of cytologic atypia ER: diffuse and intense + in CCL cells Mib-1: low in all CCL Limited value of IHC in diagnosis of FEA CK5/6 Reproducibility in diagnosis of FEA O Malley F, et al. Mod Pathol 2006;19: Differential diagnosis for FEA 30 columnar lesions, 8 breast pathologists Powerpoint tutorial with written criteria and images Classified as atypia or no atypia 91.8% agreement (25 cases unanimous agreement) Better agreement on determining no atypia Atypical ductal hyperplasia Apocrine metaplasia Focal secretory change Clinging type DCIS, pleomorphic type (highgrade) 18



19 FEA versus ADH Both with low-grade cytologic atypia Distinction based on architectural atypia FEA: flat, lack architectural complexity ADH: with architectural atypia Apocrine metaplasia FEA Brightly eosinophilc granular cytoplasm Low N/C ratio Calcium oxalate Eosinophilic or amphophilic cytoplasm High N/C ratio Psammoma calcification Both with apical snouts and uniform round nuclei 19








20 Apocrine metaplasia FEA Secretory change ER ER Secretory change Secretory change FEA Bubbly or vacuolated cytoplasm Prominent hobnail cells Nuclei not monotonous ± smudging degenerating chromatin 20


21 Clinging DCIS, high-grade HG clinging DCIS FEA Pleomorphic HG nuclei Monomorphic LG nuclei Clinical features of FEA Risk factor for concomitant cancer? Risk factor for long-term cancer development? Clinical features of FEA Risk factor for concomitant cancer? FEA is frequently associated with ADH, DCIS, lobular neoplasia and invasive cancer in adjacent breast Risk factor for long-term cancer development? 21




22 FEA with low-grade DCIS and tubular carcinoma FEA with tubular carcinoma FEA with ductal carcinoma in situ FEA with lobular neoplasia 22
23 FEA is frequently associated with cancer surgical excisions for microcalcifications DCIS associated with FEA Type of atypia FEA (3.6%) ADH (12.1%) LN (7.9%) Without cancer 83% 64% 62% Cancer* 17% # 36% 38% Low nuclear grade Micropapillary and cribriform patterns Absence of comedo necrosis *Cancer defined as DCIS or invasive ca #Invasive cancer often as tubular ca or ILC Collins L et al. Mod Pathol 2007 de Mascarel et al, Virchows Arch 2007 CCL is associated with low-grade invasive ca-- Concomitant lesions with FEA Tubular ca (n=135) Inv lobular ca (n=180) LG IDC (n=60) HG IDC (n=100) CCL Lobular neoplasia ADH/non HG DCIS HG DCIS 93% 35% 92% 1% 60% 90% 34% 10% 82% 23% 87% 15% 8% 10% 15% 70% Atypical ductal hyperplasia Lobular neoplasia Non high-grade DCIS Low-grade invasive ca: tubular ca, ILC FEA: a high risk factor (red flag) for a concomitant worse lesion Modified from Abdel-Fatah et al: 2008 AJSP 23
24 Clinical features of FEA Risk factor for concomitant cancer? FEA is a high risk factor for a concomitant worse lesion in the adjacent breast Risk factor for long-term cancer development? Long-term cancer risk in FEA-- Clinical outcome of FEA on excision Retrospective studies on patients diagnosed with clinging DCIS, mornomorphic type Low recurrence rate (0-4%) Low rate of progression to invasive ca (0-2.6%) Eusebi V et al: 1994 Semin Diagn Pathol Bijker N et al: 2001 J Clin Oncol de Mascare et al: 2007 Virchows Arch 2007 Long-term cancer risk in FEA-- Columnar cell lesions and breast cancer risk Nashiville Breast Cohort RR= 1.47 at 17 years 2-3x increase in prevalence of atypical hyperplasia No differences among 3 categories of CCL Subsequent cancer risk bilateral Nurses Health Study OR= 1.44 Risk attenuated (OR= 1.20) when adjusted for BBD Long-term cancer risk in FEA-- Clinical outcome of FEA on excision Low recurrence rate (0-4%) Low rate of progression to invasive ca (2.6%) Mild increase in cancer risk FEA is a marker of slightly increased risk for subsequent cancer. The risk is bilateral. Mild increase in long-term cancer risk *Boulos et al: 2008 Cancer;113: *Simpson et al: 2010 Mod Pathol:72A (abstr) *Collins et al: 2010 Mod Pathol:42A (abstr) *Eusebi V et al: 1994 Semin Diagn Pathol *de Mascare et al: 2006 Mod Pathol (abstr) *Simpson et: 2010 Mod Pathol (abstr) *Bijker N et al: 2001 J Clin Oncol *Boulos et al: 2008 Cancer *Collins et al: 2010 Mod Pathol (abstr) 24
25 Breast diseases and risk of invasive ca Nonproliferative lesions: no increased risk mild hyperplasia (< 4-cell layers), cysts, apocrine change, duct ectasia, simple FA, mastitis Proliferative lesions without atypia: 1.5-2x risk moderate to florid UDH, sclerosing adenosis, complex FA, papilloma, radial scar Columnar cell lesion/fea: ~1.5x risk Atypical hyperplasia (ADH, ALH): 4-5x risk Biomarker profile of FEA CK19 +, CK5/6 Strong ER and PR + Bcl-2 +, cyclin D1 + HER2 Low Mib-1 proliferation index (mean ~8%) Profile Similar to adjacent low-grade invasive ca Low-grade DCIS and LCIS: 10x risk Genetic changes in FEA Clonal chromosomal alterations Share similar, but less, genetic changes when compared with adjacent DCIS and invasive cancer Changes different than those seen in HG DCIS and IDC FEA and LG DCIS/Invasive ca Physical proximity in the breast Similar biomarker profile Similar genetic alterations Clinical follow-up studies Moinfar et al: 2000 Cancer Simpson et al: 2005 AJSP Simpson et al: J Pathol Earliest recognizable, but non-obligate precursor of low grade breast cancer pathway 2. Progression slow 25
 tissue Regular clinical and")
26 Management of FEA-- Found on CNB as most advanced lesion Additional level sections Most: recommend conservative excision Some: close follow-up with repeat mammogram Follow-up excision: 0-38% upgraded to DCIS and/or invasive ca Management of FEA-- Found on excision as most advanced lesion Levels to look for features diagnostic of ADH or DCIS Submit all (parenchymal) tissue Regular clinical and mammographic followup *Lee et al: 2010 Breast J *Chivukula et al: 2009 Am J Clin Pathol Piubello et al: 2009 AJSP Datrice et al: 2007 Am Surg *Ingegnoli et al: 2010 Breast J *Senetta et al: 2009 Mod Pathol *Martel et al: 2007 Virchows Arch * Kunju et al: 2007 Hum Pathol Management of FEA-- Found on excision with concomitant DCIS Should FEA be taken into consideration in: -determining DCIS size? -margin evaluation? Unanswered questions, however, current recommendation is No FEA: Take-home message (I) Diagnosis based on low-grade cytologic atypia Distinction from ADH based on architecture High risk factor for concomitant cancer, but mildly increased risk for subsequent cancer Likely early, but non-obligate precursor for low grade breast ca 26

 A wide spectrum similar to")


27 FEA: Take-home message (II) Excision is generally recommended if found on CNB Regular follow-up if found on excision Apocrine lesions Papillary apocrine change (simple and complex) A wide spectrum similar to non-apocrine ductal lesions Normal apocrine cells have large nuclei and prominent nucleoli, so nuclear size cannot be used to distinguish apocrine change from atypical apocrine lesions Criteria: cytologic atypia, size, (architecture, necrosis) 27
 Apocrine DCIS Apocrine")

28 Apocrine lesions Cytologic atypia in apocrine lesions-- Normal apocrine cells as reference point A wide spectrum similar to non-apocrine ductal lesions Normal apocrine cells have large nuclei and prominent nucleoli, so nuclear size cannot be used to distinguish apocrine change from atypical apocrine lesions Criteria: cytologic atypia, size, (architecture, necrosis) Apocrine DCIS Apocrine metaplasia Markedly enlarged (>3x) variable nuclei Multiple irregular nucleoli or markedly enlarged single nucleolus Irregular nuclear membrane Coarse chromatin Large but uniform nuclei Prominent but uniform nucleoli Smooth nuclear membrane Fine chromatin Diagnosis of apocrine lesions Benign apocrine change: lack cytologic atypia Apocrine DCIS Most: obvious cytologic atypia, + necrosis, large Rare: less cytologic atypia, but arranged in cribriform pattern identical to that in cribriform DCIS Atypical apocrine lesions: cytologic atypia and limited extent (size cut off?) 28
Columnar Cell Lesions
 Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Question? Columnar cell lesions are: a) Annoying lesions
Columnar Cell Lesions. Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Columnar Cell Lesions Lesions characterized by columnar epithelial cells
Columnar Cell Lesions and Flat Epithelial Atypia
 Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Columnar Cell Lesions and Flat Epithelial Atypia Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA Terminology for Columnar Cell
Epithelial Columnar Breast Lesions: Histopathology and Molecular Markers
 29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
29th Annual International Conference Advances in the Application of Monoclonal Antibodies in Clinical Oncology and Symposium on Cancer Stem Cells 25 th -27t h June, 2012, Mykonos, Greece Epithelial Columnar
Proliferative Breast Disease: implications of core biopsy diagnosis. Proliferative Breast Disease
 Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Breast Disease: implications of core biopsy diagnosis Jean F. Simpson, M.D. Breast Pathology Consultants, Inc. Nashville, TN Proliferative Breast Disease Must be interpreted in clinical and
Proliferative Epithelial lesions of the Breast. Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London
 Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Proliferative Epithelial lesions of the Breast Sami Shousha, MD, FRCPath Charing Cross Hospital & Imperial College, London Amman, November2013 Proliferative Epithelial Lesions of the Breast Usual type
Flat Epithelial Atypia
 Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Flat Epithelial Atypia Richard Owings, M.D. University of Arkansas for Medical Sciences Department of Pathology Flat epithelial atypia can be a difficult lesion May be a subtle diagnosis Lots of changes
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly
 Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
Ductal Proliferations of the Breast: The Good, the Bad, and the Ugly Melinda F. Lerwill, MD CRITERIA FOR DISTINGUISHING LOW-GRADE DUCTAL CARCINOMA IN SITU FROM USUAL DUCTAL HYPERPLASIA CYTOLOGY Low-grade
Benign Breast Disease and Breast Cancer Risk
 Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Benign Breast Disease and Breast Cancer Risk Jean F. Simpson, M.D. Vanderbilt University Nashville, Tennessee December 1, 2011 Nashville Nashville Lebanon 1 Cedars of Lebanon State Park The American University
Disclosures 5/27/2012. Outline of Talk. Outline of Talk. When Is LCIS Clinically Significant? Classic LCIS. Classic LCIS
 When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
When Is LCIS Clinically Significant? Disclosures I have nothing to disclose Yunn-Yi Chen, MD, PhD Professor Outline of Talk Outline of Talk Classic LCIS Classic LCIS Definition of lobular differentiation
04/10/2018 HIGH RISK BREAST LESIONS. Pathology Perspectives of High Risk Breast Lesions ELEVATED RISK OF BREAST CANCER HISTORICAL PERSPECTIVES
 Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Flat Epithelial Atypia: A Review of Current Concepts
 90 The Open Breast Cancer Journal, 2010, 2, 90-94 Flat Epithelial Atypia: A Review of Current Concepts Amy L. Adams * Open Access Department of Pathology and Laboratory Medicine, Emory University School
90 The Open Breast Cancer Journal, 2010, 2, 90-94 Flat Epithelial Atypia: A Review of Current Concepts Amy L. Adams * Open Access Department of Pathology and Laboratory Medicine, Emory University School
Cytyc Corporation - Case Presentation Archive - March 2002
 FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
FirstCyte Ductal Lavage History: 68 Year Old Female Gail Index: Unknown Clinical History: Negative Mammogram in 1995 6 yrs. later presents with bloody nipple discharge Subsequent suspicious mammogram Suspicious
CLINICAL SIGNIFICANCE OF BENIGN EPITHELIAL CHANGES
 Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillomas. Papillomas are composed of multiple branching fibrovascular cores, each having a connective tissue axis lined by luminal and myoepithelial cells ( Fig. 23-11 ). Growth occurs within a dilated
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Pathology of Lobular & Ductal Preneoplasia. Syed A Hoda, MD Weill-Cornell, New York, NY
 Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Breast pathology. 2nd Department of Pathology Semmelweis University
 Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
Breast pathology 2nd Department of Pathology Semmelweis University Breast pathology - Summary - Benign lesions - Acute mastitis - Plasma cell mastitis / duct ectasia - Fat necrosis - Fibrocystic change/
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
6/3/2010. Outline of Talk. Lobular Breast Cancer: Definition of lobular differentiation. Common Problems in Diagnosing LCIS in Core Biopsies
 Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Outline of Talk Lobular Breast Cancer: Common Problems in Diagnosing LCIS in Core Biopsies Definition of lobular differentiation Variants of LCIS that: carry risk for unsampled invasive cancer mimic DCIS
Treatment options for the precancerous Atypical Breast lesions. Prof. YOUNG-JIN SUH The Catholic University of Korea
 Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Treatment options for the precancerous Atypical Breast lesions Prof. YOUNG-JIN SUH The Catholic University of Korea Not so benign lesions? Imaging abnormalities(10% recall) lead to diagnostic evaluation,
Diseases of the breast (1 of 2)
") Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Diseases of the breast (1 of 2) Introduction A histology introduction Normal ducts and lobules of the breast are lined by two layers of cells a layer of luminal cells overlying a second layer of myoepithelial
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Significance of flat epithelial atypia on mammotome core needle biopsy: should it be excised? B
 Human Pathology (2007) 38, 35 41 www.elsevier.com/locate/humpath Original contribution Significance of flat epithelial atypia on mammotome core needle biopsy: should it be excised? B Lakshmi P. Kunju MD,
Human Pathology (2007) 38, 35 41 www.elsevier.com/locate/humpath Original contribution Significance of flat epithelial atypia on mammotome core needle biopsy: should it be excised? B Lakshmi P. Kunju MD,
Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting
 PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
PATHOLOGY IN-SITU CARCINOMA, ROHIT BHARGAVA, MD 1 Good afternoon everyone. First of all many thanks to Dr. Bonaventura and Dr. Arn for inviting me here, it s great to be here and I m going to talk about
1 NORMAL HISTOLOGY AND METAPLASIAS
 1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
1 NORMAL HISTOLOGY AND METAPLASIAS, MD Anatomy and Histology 1 Metaplasias 2 ANATOMY AND HISTOLOGY The female breast is composed of a branching duct system, which begins at the nipple with the major lactiferous
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening.
 The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
The Hot Topic for today is a biopsy from a 58-year-old woman who had worrisome mammographic calcifications on screening. 1 My name is Dan Visscher; I am a consultant in the Division of Anatomic Pathology
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise)
") Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
Controversies and Problematic Issues in Core Needle Biopsies (To excise or not to excise) Laura C. Collins, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Schematic Representation
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
The Diagnosis and Management of Pre-invasive Breast Disease: Flat Epithelial Atypia Classification, Pathologic Features and Clinical Significance
 The Diagnosis and Management of Pre-invasive Breast Disease: Flat Epithelial Atypia Classification, Pathologic Features and Clinical Significance The Harvard community has made this article openly available.
The Diagnosis and Management of Pre-invasive Breast Disease: Flat Epithelial Atypia Classification, Pathologic Features and Clinical Significance The Harvard community has made this article openly available.
Breast Pathology. Breast Development
 Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
Breast Pathology Lecturer: Hanina Hibshoosh, M.D. Reading: Kumar, Cotran, Robbins, Basic Pathology, 6th Edition, pages 623-635 Breast Development 5th week - thickening of the epidermis - milk line 5th
High risk lesions of the breast : Review of the current diagnostic and management strategies
 High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
High risk lesions of the breast : Review of the current diagnostic and management strategies Poster No.: C-1204 Congress: ECR 2016 Type: Educational Exhibit Authors: P. Jagmohan, F. J. Pool, P. G. Pillay,
Evaluation of Breast Specimens Removed by Needle Localization Technique
 Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
Evaluation of Breast Specimens Removed by Needle Localization Technique Specimen Handling: The breast specimen when received should be measured and grossly inspected for any orientation designated by the
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
3/27/2017. Disclosure of Relevant Financial Relationships. Papilloma???
 Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Ana Sofia Preto 19/06/2013
 Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
Ana Sofia Preto 19/06/2013 Understanding the underlying pathophysiologic processes leading to the various types of calcifications Description and illustration of the several types of calcifications, according
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
In Situ Breast Carcinoma. James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA
 In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
In Situ Breast Carcinoma James L. Connolly, M.D Beth Israel Deaconess Medical Center Professor of Pathology Harvard Medical School Boston, MA Content In Situ Ductal Carcinoma In Situ Lobular Carcinoma
Macro- and microacinar proliferations of the prostate
 Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
Macro- and microacinar proliferations of the prostate (with emphasis on cancer mimics) Rodolfo Montironi, MD (IT), FRCPath (UK), IFCAP (USA) Polytechnic University of Marche Region (Ancona) School of Medicine,
LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR
 INTERNAL MAMMARY SUPRACLAVICULAR") BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
BREAST LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR HISTOLOGY LOBE: (10 in whole breast) LOBULE: (many per lobe) ACINUS/I, aka ALVEOLUS/I: (many per lobule) DUCT(S): INTRA- or
Breast: Difficulties in Core Biopsies
 Breast: Difficulties in Core Biopsies Anna Marie Mulligan, MB, MSc, FRCPath University Health Network and University of Toronto E-mail: annamarie.mulligan@uhn.ca No conflicts of interest Role of Core Needle
Breast: Difficulties in Core Biopsies Anna Marie Mulligan, MB, MSc, FRCPath University Health Network and University of Toronto E-mail: annamarie.mulligan@uhn.ca No conflicts of interest Role of Core Needle
ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY. Jonathan I. Epstein.
 1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
1 ARTHUR PURDY STOUT SOCIETY COMPANION MEETING: DIFFICULT NEW DIFFERENTIAL DIAGNOSES IN PROSTATE PATHOLOGY Jonathan I. Epstein Professor Pathology, Urology, Oncology The Reinhard Professor of Urological
Benign Mimics of Malignancy in Breast Pathology
 Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Benign Mimics of Malignancy in Breast Pathology Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School,
Arthur Purdy Stout Society of Surgical Pathologists Companion Meeting Benign Mimics of Malignancy in Breast Pathology Stuart J. Schnitt, M.D. Beth Israel Deaconess Medical Center and Harvard Medical School,
Immunohistochemical studies (ER & Ki-67) in Proliferative breast lesions adjacent to malignancy
 in Proliferative breast lesions adjacent to malignancy") IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 84-89 Immunohistochemical studies (ER & Ki-67) in Proliferative
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 84-89 Immunohistochemical studies (ER & Ki-67) in Proliferative
The management of B3 lesions with emphasis on lobular neoplasia
 The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
3/28/2017. Disclosure of Relevant Financial Relationships. GU Evening Subspecialty Case Conference. Differential Diagnosis:
 GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
GU Evening Subspecialty Case Conference Rajal B. Shah, M.D. VP, Medical Director, Urologic Pathology Miraca Life Sciences, Irving, Texas Clinical Associate Professor of Pathology Baylor College of Medicine,
Current issues in diagnostic breast pathology
 1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
1 Cancer Studies and Molecular Medicine, University of Leicester, Leicester, UK 2 Academic Unit of Pathology, Leeds University, Leeds, UK 3 Academic Oncology/Breast Pathology, King s College London, London,
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Title malignancy. Issue Date Right 209, 12, (2013)
") NAOSITE: Nagasaki University's Ac Title Author(s) A case of intracystic apocrine papi malignancy Hayashi, Hiroko; Ohtani, Hiroshi; Y Citation Pathology - Research and Practice, Issue Date 2013-12 URL Right
NAOSITE: Nagasaki University's Ac Title Author(s) A case of intracystic apocrine papi malignancy Hayashi, Hiroko; Ohtani, Hiroshi; Y Citation Pathology - Research and Practice, Issue Date 2013-12 URL Right
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Papillary Lesions of the Breast Texas Society of Pathologists 2013 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical
Atypical proliferative lesions diagnosed on core biopsy - 6 year review
 Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
IBCM 2, April 2009, Sarajevo, Bosnia and Herzegovina
 Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Preoperative diagnosis and treatment planning in breast cancer The pathologist s perspective L. Mazzucchelli Istituto Cantonale di Patologia Locarno, Switzerland IBCM 2, 23-25 April 2009, Sarajevo, Bosnia
Notice of Faculty Disclosure
 California Society of Pathology Diagnostic Problems in Surgical Pathology December 2015 Case 2 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director of Anatomic Pathology Beth Israel
California Society of Pathology Diagnostic Problems in Surgical Pathology December 2015 Case 2 Laura C. Collins, M.D. Associate Professor of Pathology Associate Director of Anatomic Pathology Beth Israel
Protocol for the Examination of Biopsy Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: BreastInvasive 1.0.0.0 Protocol Posting Date: February 2019 Accreditation Requirements The use of
Mammographic imaging of nonpalpable breast lesions. Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand
 Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
Mammographic imaging of nonpalpable breast lesions Malai Muttarak, MD Department of Radiology Chiang Mai University Chiang Mai, Thailand Introduction Contents Mammographic signs of nonpalpable breast cancer
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST
 COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
COMMON BENIGN DISORDERS AND DISEASES OF THE BREAST Aberrations of Normal Development and Involution (ANDI). The basic principles underlying the aberrations of normal development and involution (ANDI) classification
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall
 Malaysian J Pathol 2015; 37(3) : 281 285 CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall Hiroko HAYASHI, Hiroshi OHTANI,* Junzo YAMAGUCHI,** and Isao SHIMOKAWA Department
Malaysian J Pathol 2015; 37(3) : 281 285 CASE REPORT Malignant transformation of breast ductal adenoma: a diagnostic pitfall Hiroko HAYASHI, Hiroshi OHTANI,* Junzo YAMAGUCHI,** and Isao SHIMOKAWA Department
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Enterprise Interest None
 Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
Enterprise Interest None B3 lesions of the breast What are they at surgery? Case 4 Edi Brogi MD PhD Attending Pathologist - Director of Breast Pathology Memorial Sloan Kettering Cancer Center New York
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
CINtec p16 INK4a Staining Atlas
 CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
CINtec p16 INK4a Staining Atlas Rating Rating Positive The rating positive will be assigned if the p16 INK4a -stained slide shows a continuous staining of cells of the basal and parabasal cell layers of
Segmental Breast Calcifications
 Residents Section Pattern of the Month Chen et al. Segmental reast Calcifications Residents Section Pattern of the Month Residents inradiology Po-Hao Chen 1 Erica T. Ghosh 1,2 Priscilla J. Slanetz 1,2
Residents Section Pattern of the Month Chen et al. Segmental reast Calcifications Residents Section Pattern of the Month Residents inradiology Po-Hao Chen 1 Erica T. Ghosh 1,2 Priscilla J. Slanetz 1,2
Prepared By Jocelyn Palao and Layla Faqih
 Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
Prepared By Jocelyn Palao and Layla Faqih The structure of the suspected atypical cell should always be compared to the structure of other similar, benign, cells which are present in the smears. The diagnosis
RSNA, /radiol Appendix E1. Methods
 RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
RSNA, 2016 10.1148/radiol.2016151097 Appendix E1 Methods US and Near-infrared Data Acquisition Four optical wavelengths (740 nm, 780 nm, 808 nm, and 830 nm) were used to sequentially deliver the light
COMPANION MEETING BREAST. Auditorium 11:15 1:00 am. Convenor: A/Professor Gelareh Farshid, SA Pathology, SA
 Australasian Division of the International Academy of Pathology Limited ABN 73 008 593 815 36 TH Annual Scientific Meeting Darling Harbour Convention Centre, Sydney, Australia June 3-5, 2011 COMPANION
Australasian Division of the International Academy of Pathology Limited ABN 73 008 593 815 36 TH Annual Scientific Meeting Darling Harbour Convention Centre, Sydney, Australia June 3-5, 2011 COMPANION
Management of B3 lesions
 Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
Management of B3 lesions Pathological view Abeer Shaaban Queen Elizabeth Hospital Birmingham FEA AIDP B3 lesions In situ Lobular neoplasia Papilloma Radial scar Fibroaepithelial lesion Mucocoele like lesion
Non-mass Enhancement on Breast MRI. Aditi A. Desai, MD Margaret Ann Mays, MD
 Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
Non-mass Enhancement on Breast MRI Aditi A. Desai, MD Margaret Ann Mays, MD Breast MRI Important screening and diagnostic tool, given its high sensitivity for breast cancer detection Breast MRI - Indications
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA
 PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA AND IMPORTANT MIMICKERS PROSTATIC ADENOCARCINOMA: DIAGNOSTIC CRITERIA 1 A good H & E helps! ADENOCARCINOMA DIAGNOSTIC CRITERIA Relatively uniform proliferation
A Practical Approach to the Evaluation of Fibroepithelial Lesions. Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology
 A Practical Approach to the Evaluation of Fibroepithelial Lesions Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Overview Fibroadenomas (FAs) Phyllodes Tumors (PTs) Morphology and
A Practical Approach to the Evaluation of Fibroepithelial Lesions Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Overview Fibroadenomas (FAs) Phyllodes Tumors (PTs) Morphology and
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature
 Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
Controversies on the Management of High Risk Breast Lesions on Core Biopsy: An Update on the Literature Dianne Georgian- Smith MD Brigham and Women s Hospital Associate Professor of Radiology, Harvard
In situ lobular neoplasia of the breast with marked myoepithelial proliferation
 In situ lobular neoplasia of the breast with marked myoepithelial proliferation Sami Shousha To cite this version: Sami Shousha. In situ lobular neoplasia of the breast with marked myoepithelial proliferation.
In situ lobular neoplasia of the breast with marked myoepithelial proliferation Sami Shousha To cite this version: Sami Shousha. In situ lobular neoplasia of the breast with marked myoepithelial proliferation.
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues
- Test slide, Breast cancer tissues with corresponding normal tissues") A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
A712(19)- Test slide, Breast cancer tissues with corresponding normal tissues (formalin fixed) For research use only Specifications: No. of cases: 12 Tissue type: Breast cancer tissues with corresponding
Leonard M. Glassman MD Analysis of Breast Calcifications
 Importance of Calcification Leonard M. Glassman MD FACR American Institute for Radiologic Pathology Washington Radiology Associates, PC Washington DC 45% of all breast cancers present as calcification
Importance of Calcification Leonard M. Glassman MD FACR American Institute for Radiologic Pathology Washington Radiology Associates, PC Washington DC 45% of all breast cancers present as calcification
Diagnostic Problems in Breast Pathology How to avoid the pitfalls
 FORUM OF PATHOLOGY Diagnostic Problems in Breast Pathology How to avoid the pitfalls Professor C W Elston City Hospital Nottingham, United Kingdom Introduction Almost any breast lesion may produce diagnostic
FORUM OF PATHOLOGY Diagnostic Problems in Breast Pathology How to avoid the pitfalls Professor C W Elston City Hospital Nottingham, United Kingdom Introduction Almost any breast lesion may produce diagnostic
Outline 11/2/2017. Pancreatic EUS-FNA general aspects. Cytomorphologic features of solid neoplasms/lesions of the pancreas
 ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
ENDOSCOPIC ULTRASOUND GUIDED-FINE NEEDLE ASPIRATION CYTOLOGY OF PANCREAS Khalid Amin M.D. Assistant Professor Department of Laboratory Medicine and Pathology University of Minnesota Outline Pancreatic
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
CNB vs Surgical Excision
 Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Update on Core Needle Biopsy of Non-palpable Breast Lesions Nour Sneige, M.D. UT MD Anderson Cancer Center Houston, Tx Image-Guided CNB of Breast Lesions An alternative to surgical biospy CNB vs Surgical
Image guided core biopsies:
 Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
Recommendations on the Surgical, Radiologic and Pathologic Approaches to Breast Disease: Using best practices based on multidisciplinary methodologies developed through the Allina Breast Committee. Image
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Benign breast disease and cancer risk
 Critical Reviews in ONCOLOGY1 HEMA TOLOG Y Critical Reviews in Oncology/Hematology 15 ( 1993) 22 I-242 Benign breast disease and cancer risk Simonetta Bianchi*, Domenico Palli b, Monica Galli, Giancarlo
Critical Reviews in ONCOLOGY1 HEMA TOLOG Y Critical Reviews in Oncology/Hematology 15 ( 1993) 22 I-242 Benign breast disease and cancer risk Simonetta Bianchi*, Domenico Palli b, Monica Galli, Giancarlo
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Lower-Category Benign Breast Disease and the Risk of Invasive Breast Cancer
 Lower-Category Benign Breast Disease and the Risk of Invasive Breast Cancer Jiping Wang, Joseph P. Costantino, Elizabeth Tan-Chiu, D. Lawrence Wickerham, Soonmyung Paik, Norman Wolmark Background: The
Lower-Category Benign Breast Disease and the Risk of Invasive Breast Cancer Jiping Wang, Joseph P. Costantino, Elizabeth Tan-Chiu, D. Lawrence Wickerham, Soonmyung Paik, Norman Wolmark Background: The
Demystifying Endometrial Hyperplasia
 Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate
Demystifying Endometrial Hyperplasia A review from Diagnostic Histopathology 19:7 Dr R Hadden ST5 Histopathology Derriford Hospital Plymouth Endometrium Target for sex-steroid hormones Glands Stroma Proliferate