04/13/2017. Sinonasal Pathology. Sinonasal Tract Pathology Outline. 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017
|
|
|
- Kristin Williams
- 5 years ago
- Views:
Transcription
 papillomas Glandular neoplasms")
1 Sinonasal Pathology 24 th Annual Seminar in Pathology Pittsburgh, PA April 27, 2017 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL Sinonasal Tract Pathology Outline Sinonasal (Schneiderian) papillomas Glandular neoplasms Small round cell malignant neoplasms 1
2 Sinonasal Papillomas Definition Group of benign neoplasms arising from the sinonasal (Schneiderian) mucosa and composed of squamous or columnar epithelial proliferation with associated mucous cells Sinonasal Papillomas Classification Inverted type Exophytic (fungiform, septal) type Oncocytic (cylindrical or columnar cell) type Sinonasal Papillomas: Clinicopathologic Features Exophytic Inverted Oncocytic Percentage 20-50% 47-73% 3-8% Gender/Age M>F; yrs M>F; yrs M=F; >50 yrs Location Nasal septum Lateral nasal wall in region of middle turbinates with extension into sinuses Focality Unilateral Typically unilateral; rarely, bilateral Incidence of HPV Approximately 50% positive; HPV 6 and 11; less frequently HPV 16, 18; rarely HPV 57 Incidence of Malignant Transformation Approximately 38% positive; HPV 6 and 11; less frequently HPV 16, 18; rarely HPV 57 Lateral nasal wall and sinuses (maxillary or ethmoid) Unilateral Rare 2-27% 4-17% Typically absent 2


3 Sinonasal Papillomas Clinical Features Typically, unilateral; bilateral papillomas, in particular the inverted subtype, may occur with reported incidence of up to 10%: Symptoms: airway obstruction, epistaxis, an asymptomatic mass and pain May occur simultaneously with nasal inflammatory polyps Radiology - varies with extent of disease: soft tissue density is seen early in the disease; opacification and mucosal thickening are present with more extensive disease; evidence of pressure erosion of bone may be seen. 3



4 4



5 5



6 6

")
7 DPAS Sinonasal Papilloma, Inverted Type Differential Diagnosis Sinonasal inflammatory polyps Non-keratinizing respiratory ( transitional ) carcinoma 7



8 8



9 9



10 10



11 11



12 12



13 13



14 14



15 15



16 16
17 Sinonasal Papilloma, Septal Type Differential Diagnosis Squamous papilloma Sinonasal Papilloma, Oncocytic Type Differential Diagnosis Rhinosporidiosis Low-grade papillary adenocarcinoma Sinonasal Papillomas: Clinicopathologic Features Exophytic Inverted Oncocytic Percentage 20-50% 47-73% 3-8% Gender/Age M>F; yrs M>F; yrs M=F; >50 yrs Location Nasal septum Lateral nasal wall in region of middle turbinates with extension into sinuses Focality Unilateral Typically unilateral; rarely, bilateral Incidence of HPV Approximately 50% positive; HPV 6 and 11; less frequently HPV 16, 18; rarely HPV 57 Incidence of Malignant Transformation Approximately 38% positive; HPV 6 and 11; less frequently HPV 16, 18; rarely HPV 57 Lateral nasal wall and sinuses (maxillary or ethmoid) Unilateral Rare 2-27% 4-17% Typically absent 17
18 Sinonasal Papillomas Treatment and Prognosis Complete surgical excision, including adjacent uninvolved mucosa; the latter is necessary as growth and extension along the mucosa results from the induction of squamous metaplasia in the adjacent sinonasal mucosa Adequate surgery includes a lateral rhinotomy or medial maxillectomy with en bloc excision Schneiderian papillomas of all histologic types will recur if incompletely resected: recurrence probably represents persistence of disease rather than multicentricity of the neoplasm In general, prognosis is good following complete surgical excision; however, if left unchecked, these neoplasms have the capability of continued growth with extension along the mucosal surface with destruction of bone and invasion of vital structures Sinonasal Papillomas Treatment and Prognosis Adjuvant therapy (chemo-and radiotherapy) has not been shown to be of benefit in sinonasal papilloma Complications include recurrence and malignant transformation: majority of the malignancies are squamous cell carcinomas (keratinizing and non-keratinizing), varying in appearance from well to poorly differentiated; less frequently, other carcinomas may occur including verrucous carcinoma, mucoepidermoid carcinoma, small cell carcinoma, adenocarcinoma and sinonasal undifferentiated carcinoma may occur synchronously or metachronously Sinonasal Papillomas Treatment and Prognosis No reliable histologic features that predict which papillomas are likely to become malignant: papillomas with increased cellularity, pleomorphism, and increased mitotic activity do not necessarily become malignant; the presence of moderate to severe epithelial dysplasia is a potential indicator of malignant transformation; surface keratinization and dyskeratosis have anecdotally been considered as possible predictors of malignant transformation; any sinonasal papilloma that shows moderate to severe dysplasia or has surface keratinization should prompt thorough histologic examination of all resected tissue to exclude the presence of malignancy; No correlation between the number of recurrences and the development of carcinoma 18

19 Sinonasal Papillomas Treatment and Prognosis Treatment for malignant transformation of a sinonasal papilloma includes surgery and radiotherapy Prognosis for patients with malignant transformation varies: In some patients the carcinomas are only locally invasive with favorable prognosis following treatment; In other patients there may be extensive invasion with involvement of vital structures and/or metastatic disease; these patients generally have a poor clinical outcome irrespective of therapeutic intervention Sinonasal Adenocarcinoma Heterogenous group of tumor types, including minor salivary gland origin and surface-derived 19
20 Sinonasal Glandular Neoplasms Classification Benign (Adenomas): Minor salivary gland neoplasms Malignant (Adenocarcinomas): Minor salivary gland neoplasms Non-salivary gland, non-intestinal type Intestinal type (ITACs) Sinonasal Adenocarcinoma Represent 10-20% of all malignant sinonasal tract tumors Nonintestinal and Intestinal types Salivary gland types (adenoid cystic carcinoma >> others (acinic cell adenocarcinoma, adenocarcinoma, NOS, mucoepidermoid carcinoma, others) Sinonasal Adenocarcinoma Non-Intestinal Type No gender predilection Most often occur in 5 th -7 th decades of life Most common in ethmoid sinus but may occur anywhere in the SNT Nasal obstruction and/or epistaxis No occupational or environmental exposure 20


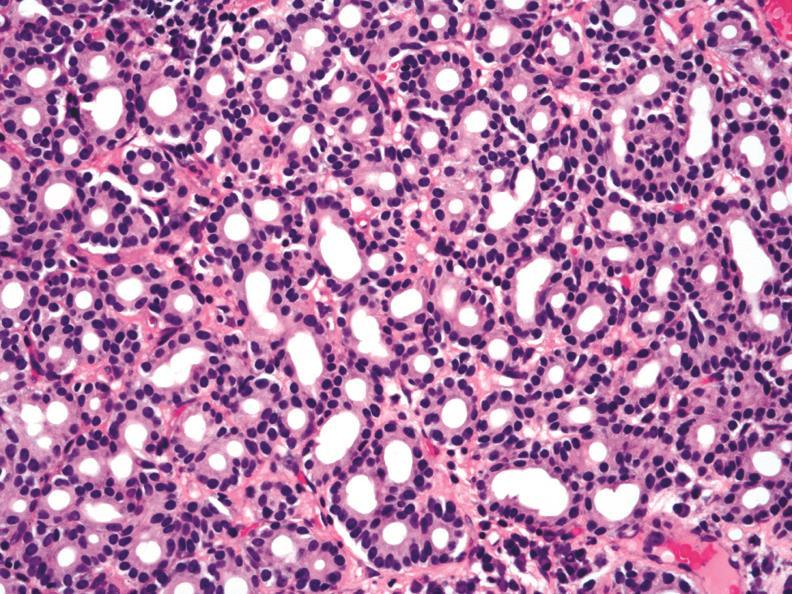
21 Sinonasal Adenocarcinoma, Nonintestinal Type Pathologic Features Low-grade: circumscribed but unencapsulated glandular and papillary growth uniform appearing glands or acini with back-to-back growth devoid of intervening stroma; single layer of nonciliated cuboidal to columnar cells with pleomorphism and mitotic activity; no atypical mitoses or necrosis 21


22 p63 22



23 p63 23


24 Sinonasal Adenocarcinoma, Nonintestinal Type Pathologic Features High-grade: invasive; predominantly solid but may have glandular and papillary growth back-to-back growth devoid of intervening stroma; single layer of nonciliated cuboidal to columnar cells with moderate to marked pleomorphism and increased mitotic activity, including atypical mitoses, and necrosis 24


25 Sinonasal Adenocarcinoma Immunohistochemistry Consistently and intensely CK7 reactive Basal/myoepithelial markers negative Non-reactive for CK20, CDX2, villin, claudins, chromogranin or synaptophysin 25
")

26 Sinonasal Adenocarcinoma, Nonintestinal Type Differential Diagnosis Reactive glandular proliferation (setting of chronic rhinosinusitis) Sinonasal hamartomas Sinonasal papillomas Intestinal-type adenocarcinomas Salivary gland neoplasms: Adenomas (Pleomorphic; monomorphic) Adenocarcinomas 26
 hamartoma Seromucinous")
 hamartoma Nasal")
27 Sinonasal Hamartomas Respiratory epithelial adenomatoid (READ) hamartoma Seromucinous hamartoma Chondroosseous and respiratory epithelial (CORE) hamartoma Nasal chondromesenchymal hamartoma 27



28 28



29 29
 More common in men than women Most often occur in 5 th -7 th decades of life Most common in ethmoid")
30 Sinonasal Adenocarcinoma Treatment and Prognosis Complete surgical resection XRT may be used for extensive disease and/or higher grade tumors Prognosis depends on histologic type: low-grade: 70-82% 3-year survival high-grade: 20% 3-year survival Sinonasal Adenocarcinoma Intestinal Type (ITAC) More common in men than women Most often occur in 5 th -7 th decades of life Most common in ethmoid sinus > nasal cavity (inferior and middle turbinates) and maxillary sinus; may arise anywhere in sinonasal tract Early symptoms tend to be non-specific and vary from nasal stuffiness to obstruction; with persistence, may be associated with epistaxis Due to the delay in diagnosis, tumors may reach a large size with extensive invasion at the time of presentation 30

31 Sinonasal Adenocarcinoma Intestinal Type (ITAC) Advanced tumors present with pain, cranial nerve deficits, visual disturbances and exophthalmos May be associated with occupational or environmental exposures: hardwood dust, leather and softwood; increased incidences of adenocarcinoma are seen in woodworkers and workers in the shoe and furniture industries Sporadic ITACs unassociated with occupational exposure occur; tend to affect women> men; most tumors involve the maxillary antrum Barnes Classification Sinonasal Tract Intestinal-type Adenocarcinoma (ITACs) Papillarytype Colonictype Kleinsasser and Schroeder Percentage of Cases PTCC-I 18% 82% PTCC-II 40% 54% Solid-type PTCC-III 20% 36% 3-year cumulative survival Mucinous type Alveolar goblet Uncommon 48% Signet-ring Uncommon 0% Mixed Transitional Rare 71% 31



32 32



33 33



34 34
 and variably CK7 reactivity (43% to 93% of cases); CDX-2, a nuclear transcription factor involved in")

35 Sinonasal ITACs Immunohistochemistry Diffusely positive for epithelial markers pancytokeratins, EMA, B72.3, Ber-EP4 CEA staining is variable CK20 positivity (73% to 86%) and variably CK7 reactivity (43% to 93% of cases); CDX-2, a nuclear transcription factor involved in the differentiation of intestinal epithelial cells and diffusely expressed in intestinal adenocarcinomas, can be found in ITACs Expression of villin and claudins also present Neoplastic cells may express a variety of hormone peptides, including serotonin, cholecystokinin, gastrin, somatostatin and leu-enkephalin Chromogranin and synaptophysin positive cells can be identified CDX2 CK20 35

 Nasopharyngeal papillary low-grade")
36 Villin Sinonasal ITACs Differential Diagnosis Papillary sinusitis Metastatic adenocarcinoma of GIT: rare occurrence to the sinonasal tract; clinical history is critical in establishing a diagnosis of ITAC and in excluding a metastasis to the sinonasal tract from a gastrointestinal tract primary neoplasm; histology, histochemistry and IHC of ITACs and GIT adenocarcinomas are identical Non-intestinal, non-salivary gland adenocarcinoma Salivary gland type adenocarcinoma Sinonasal renal cell-like adenocarcinoma (CAIX+) Nasopharyngeal papillary low-grade adenocarcinoma 36


37 Sinonasal ITACs Treatment and Prognosis Complete surgical excision, generally via a lateral rhinotomy; depending on the extent and histology of the neoplasm surgery varies from local excision to more radical procedures (maxillectomy, ethmoidectomy and additional exenterations) Radiotherapy may be utilized for extensive disease or for higher grade neoplasms All considered potentially aggressive, lethal tumors Metastasis to cervical lymph nodes and spread to distant sites are infrequent occurring in about 10% and 20%, respectively 37
38 Classification Sinonasal Tract Intestinal-type Adenocarcinoma (ITACs) Barnes Papillarytype Colonictype Kleinsasser and Schroeder Percentage of Cases PTCC-I 18% 82% PTCC-II 40% 54% Solid-type PTCC-III 20% 36% 3-year cumulative survival Mucinous type Alveolar goblet Uncommon 48% Signet-ring Uncommon 0% Mixed Transitional Rare 71% SNT/NP Undifferentiated Malignant Neoplasms Squamous Cell Carcinoma Sinonasal Undifferentiated Carcinoma (SNUC) NP Carcinoma, Nonkeratinizing Undifferentiated NUT Midline Carcinoma SMARCB1 (INI1)-Deficient Carcinoma Olfactory Neuroblastoma Mucosal Malignant Melanoma Small Cell Neuroendocrine Carcinoma Malignant Lymphoma Rhabdomyosarcoma Ewing Family of Tumors Others 38
39 Sinonasal Undifferentiated Carcinoma (SNUC) Definition A high-grade malignant epithelial neoplasm of the nasal cavity and paranasal sinuses of uncertain histogenesis with or without neuroendocrine differentiation but without evidence of squamous or glandular differentiation (Frierson et al. AJSP 1986) SNUC Definition A highly aggressive and clinicopathologically distinctive carcinoma of uncertain histogenesis that typically presents with locally extensive disease; it is composed of pleomorphic tumor cells with frequent necrosis, and should be differentiated from other carcinomas or olfactory neuroblastoma (WHO 2004) SNUC Clinical Findings Rare tumor Male predominance (2-3:1) Broad age range (3 rd -9 th decades); median age at presentation 6th decade Presents as large mass involving multiple sites with extensive invasive growth Multiple symptoms: nasal obstruction, epistaxis, proptosis, cranial nerve palsies, visual disturbances, pain, other Symptoms are usually of short duration (weeks to months) 39
: HPV (p16 immunohistochemistry and molecular analysis) identified in a limited")
40 SNUC Etiology No known etiologic agents Negative for Epstein-Barr virus (EBER) Some associated with high risk Human papillomavirus (HPV) Some cases reported to develop after radiation therapy for nasopharyngeal carcinoma Deletion of RB gene SNUC Etiology Some associated with high risk human papillomavirus (HPV): HPV (p16 immunohistochemistry and molecular analysis) identified in a limited number of cases uncertain relationship between HPV and SNUC 40



41 41



42 CK p63 42
43 SNUC Special Stains/Studies Histochemistry: noncontributory IHC: consistently immunoreactive with epithelial markers: pan-cytokeratins, simple keratins, (CK 7, CK8 and CK19); not CK4, CK5/CK6, CK14 p63 and p40 variably positive EMA, NSE, p53 reactive < 50% cases SYN, CHR, S100 protein, Leu-7 rarely + vimentin, muscle markers, hematolymphoid markers, melanocytic cell markers absent SNUC Treatment and Prognosis Multimodality therapy considered best treatment approach to provide best chance for survival and includes radical surgery and postoperative chemoradiotherapy Highly aggressive neoplasm with poor survival 5-year overall and disease-free survival rates of 45.2% and 50.7%, respectively overall survival 32% SNUC Treatment and Prognosis Metastatic spread occurs to bone, brain, liver and cervical lymph nodes Causes of death primarily related to distant metastases and local invasion HPV-positive SNUCs may benefit from improved survival but this finding requires further substantiation 43

44 NUT Midline Carcinoma NUT = Nuclear protein in Testis NUT Midline Carcinoma (NMC)* Aggressive carcinoma genetically defined by rearrangement of balanced chromosomal translocation t(15;19) resulting in BRD4-NUT oncogene NMC vastly under-recognized and under-diagnosed Most NMCs are squamous cell carcinomas and can only be identified by molecular or IHC testing Diagnosis of NMC should be considered in any nonsmoking patient with poorly-differentiated squamous cell carcinoma *French CA, et al. J Clin Oncol 2010;63:



45 CK 45

 Death due to: Local effects of tumor Complications of therapy")
46 p63 NUT NUT Midline Carcinoma (NMC)* 22 cases Aggressive chemotherapy and radiation treatment With exception of 1 case, all patients DOD: Mean survival less than 1 year (9.5 months) Death due to: Local effects of tumor Complications of therapy *French CA, et al. J Clin Oncol 2010;63:

 SMARCB1 deletions by FISH do not harbor")


47 SMARCB1 (INI-1) Deficient Carcinoma of the Sinonasal Tract* Definition Rare carcinoma characterized by: basaloid and rhabdoid cells loss of IHC expression of SMARCB1 (INI1) SMARCB1 deletions by FISH do not harbor HPV or NUT-1 alterations Apparent aggressive clinical course including increased incidence of tumor-related mortality *Agaimy A, et al. Am J Surg Pathol 2014;38: *Bishop J, et al. Am J Surg Pathol 2014;38: INI1 47

48 Olfactory Neuroblastoma (ONB) Definition Malignant neoplasm arising from olfactory cells which are bipolar neurons that differentiate from olfactory epithelium in the roof of the nasal cavity Olfactory Neuroblastoma Clinical Findings Uncommon neoplasm F > M; bimodal age distribution 2 nd and 6 th decades of life Symptoms: nasal obstruction, epistaxis, mass, pain, headaches, cranial nerve deficits Site: above the middle turbinate high in the nasal fossa; rarely, lower nasal cavity or paranasal sinuses Etiology: No known etiologic factors in humans; t(11;22) translocation reported 48


49 Olfactory Neuroblastoma Pathologic Features Gross: variably sized, mucosal covered, soft, polypoid mass Histology (Hyams grading): Grades I, II better differentiated Grades III, IV less differentiated 49



50 50



51 51



52 52



53 53


54 54

55 Olfactory Neuroblastoma IHC Neuroendocrine markers positive: NSE Synaptophysin, CD56, chromogranin S100 protein and SOX10 positive: Peripheral sustentacular cell-like pattern Calretinin positive GFAP, NFP variably positive Epithelial markers typically negative: Cytokeratins p63 Hematolymphoid and mesenchymal markers negative S100 protein Olfactory Neuroblastoma Wooff JC et al. Am J Surg Pathol 2011;35: ONB: Calretinin positive in 95% (20/21) p63 negative in all cases Other SRBCT (MM, DLBCL, SNUC, NEC, alveolar RMS, ES/PNET, PA, TCS, NKSCC): Calretinin negative (except for PA, 1 case DLBCL) p63 variably positive 55
")
56 CALR Olfactory Neuroblastoma Treatment and Prognosis Radical surgery plus chemotherapy Chemotherapy for advanced (unresectable) disease Majority of tumors are locally aggressive 20-40% metastasize to regional lymph nodes and to bone Survival dependent on clinical (Kadish) staging 56

57 Malignant Melanoma (MM) MMM neural crest-derived neoplasms originating from melanocytes and demonstrating melanocytic differentiation 15-20% of MM occur in the H&N: > 80% cutaneous orbital > oral > other upper aerodigestive tract Sinonasal Mucosal Malignant Melanoma Clinical Findings Represent approx. 1% of all MM and 2-8% of SNT malignancies More common in men; 6 th -8 th decades Sites: Nasal cavity > paranasal sinuses: septum, lateral nasal wall maxillary > ethmoid, frontal, sphenoid Nasal obstruction, epistaxis, pain No known risk factors (? melanosis) 57



58 58



59 59



60 60



61 61

, tyrosinase, MITF1, SOX10 vimentin")
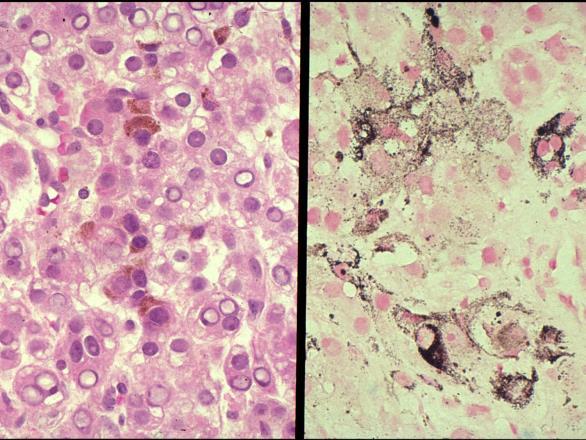
62 Sinonasal Mucosal Malignant Melanoma Special Studies Histochemistry: argentaffin and argyrophil positive; PAS+/DPAS- IHC: S100 protein, HMB45, Melan-A (A103), tyrosinase, MITF1, SOX10 vimentin Fontana C S 62


63 PAS DPAS Fontana 63



64 S100 protein HMB45 MELAN A 64



65 MITF1 Tyrosinase SOX10 65

66 VIM Sinonasal Mucosal Malignant Melanoma Molecular Studies BRAF mutations: present in 50-60% of cutaneous malignant melanoma uncommon in SMMM (<20% of cases) c-kit: somatic mutations of c-kit with oncogenic point mutations in less than 20% of SMMM NRAS mutations: appear to be relatively more frequent than BRAF and c-kit Sinonasal Mucosal Malignant Melanoma Differential Diagnosis Other undifferentiated malignancies Rule Out: metastasis from a cutaneous MM 66
 metastasis: 10-30% Histopathologic determination of anatomic level of invasion (Clark level) and thickness of tumor (Breslow thickness) utilized for cutaneous malignant melanomas and")
67 Sinonasal Mucosal Malignant Melanoma Treatment and Prognosis Surgery plus adjuvant therapy Poor prognosis: 5-year: <30%; median 2-yr survival local recurrence: 40-85% distant metastasis: 30-70% regional (nodal) metastasis: 10-30% Histopathologic determination of anatomic level of invasion (Clark level) and thickness of tumor (Breslow thickness) utilized for cutaneous malignant melanomas and are not applicable to MMM Rhabdomyosarcoma (RMS) Definition Malignant mesenchymal neoplasm of skeletal muscle cells (rhabdomyoblasts) 67
68 Head & Neck RMS General Considerations Most common sarcoma of the H&N: All ages: represents up to 50% of H&N sarcomas; Pediatric RMS: represents up to 75% of H&N sarcomas Sites: orbit > nasopharynx > ME/mastoid > SNT Symptoms dependent on site of occurrence Sinonasal Tract RMS Clinical Findings M=F; 1 st and 2 nd decades of life but occurs in adults Symptoms: nasal obstruction, rhinorrhea, epistaxis, sinusitis, pain, otalgia, headache, proptosis, visual disturbances, cranial nerve deficits Polypoid appearing mass that clinically may simulate the appearance of a nasal polyp (25% of RMS in the SNT are botryoid type) No known etiologic factors 68



69 69
 Botryoid type spindle cell type")

70 Rhabdomyosarcoma (RMS) Histologic Types Embryonal: most common type (80-85%) Botryoid type spindle cell type Alveolar: 10-15% more frequent in adult population Pleomorphic RMS RMS with ganglion cells (malignant ectomesenchymoma) 70



71 71



72 72



73 73



74 74



75 75



76 76

,")
77 RMS Special Stains Histochemistry: diastase-sensitive, PAS-positive (glycogen) IHC: Myogenic markers: desmin, HHF35, myogenin (myf-4), myoglobin Vimentin 77



78 DES Myogenin VIM 78
 on chromosome 13")

79 DES Myogenin RMS Genetic Abnormalities Alveolar RMS: t(2;13)(q36;q14) translocation 60% of cases: breakpoints occur in PAX3 gene at chromosome 2 and FOXO1A gene (formerly FKHR) on chromosome 13 results in a PAX3- FOXO1A fusion gene on chromosome 13 and a FOXO1A-PAX3 fusion gene on chromosome 2; PAX3-FOXO1A fusion appears to be more sensitive and specific than FOXO1A-PAX3 in detecting RMS 79
80 RMS Genetic Abnormalities Alveolar RMS: t(1;13)(p36;q14) translocation 20% of cases; juxtaposes PAX7 gene on 1p36 with FOXO1A gene on 13q14; approximately 80% have PAX3-FOXO1A fusion or PAX7-FOXO1A fusion approximately 20% lack either of these fusions RMS Treatment and Prognosis Multimodality therapy (surgery, radiotherapy, chemotherapy) Intergroup Rhabdomyosarcoma Study (IRS): orbit: 92% 5-year survival H&N, non-prostate bladder: 80% 5-year survival parameningeal, bladder, prostate, extremities: 70% 5-year survival poorest prognosis seen in association with RMS of retroperitoneum, biliary tract and peritoneum SNT Pathology Conclusions Discussed histologic spectrum and differential diagnosis of: Sinonasal papillomas Sinonasal Adenocarcinomas: Non-intestinal, non-salivary gland ITACs 80


81 SNT Pathology Conclusions SCC is the most common malignant neoplasm SNT is host to neoplasms of varied histogenesis Many of these other neoplasms are undifferentiated and share overlapping clinical and histopathologic features Differentiation may require IHC and molecular analysis Therapy and prognosis may vary per tumor type p63 81



82 CD20 EBER 82
Small (and large) Blue Cell Tumors of the Skull Base
 Blue Cell Tumors of the Skull Base") Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Small (and large) Blue Cell Tumors of the Skull Base Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Sinonasal Tumors. Objectives. Objectives. Incidence of Paranasal Sinus Tumors. Demographics of Paranasal Sinus Tumors. Paranasal Sinus Tumors
 Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Sinonasal Tumors Objectives Incidence and demographics of sinonasal tumors Separating tumors from inflammatory changes Common and notable histologic types of sinonasal tumors Staging of sinonasal tumors
Head and Neck Squamous Subtypes
 1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract
 California Society of Pathology Saturday Slide Seminar Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract Lester D. R. Thompson www.lester-thompson.com Learning Objectives
California Society of Pathology Saturday Slide Seminar Nutn but a Small Biopsy How to approach small biopsy samples of the sinonasal tract Lester D. R. Thompson www.lester-thompson.com Learning Objectives
Nasal Cavity and Paranasal Sinuses
 Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Chapter 2 Nasal Cavity and Paranasal Sinuses Introduction Included in this chapter are nasal cavities, frontal sinus, ethmoid complex, sphenoid sinus, and maxillary sinuses. These cavities and sinuses
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Pitfalls in Sinonasal Pathology
 Pitfalls in Sinonasal Pathology Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences jhunt2@uams.edu
Pitfalls in Sinonasal Pathology Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences jhunt2@uams.edu
Nasal Cavity and Paranasal Sinuses
 2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
2017 Head and Neck Tumors Selected Topics Lester D. R. Thompson 1 2 Inclusion Criteria Nasal Cavity and Paranasal Sinuses 2005 edition: 76 diagnoses 2017 edition: 39 diagnoses 3 1. The tumor occurs exclusively
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Mojca Velikonja Jože Pižem
 Mojca Velikonja Jože Pižem An 81-year old woman presented with an exophytic, wart-like skin lesion on her neck that she had observed for one year. Cryotherapy had been applied twice, but proved unsuccessful.
Mojca Velikonja Jože Pižem An 81-year old woman presented with an exophytic, wart-like skin lesion on her neck that she had observed for one year. Cryotherapy had been applied twice, but proved unsuccessful.
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
A CONTRIBUTION TO THE ETIOPATHOGENESIS, DIAGNOSIS AND MANAGEMENT OF SINONASAL INVERTED PAPILLOMAS
 UNIVERSITY OF MEDICINE AND PHARMACY OF TÂRGU MUREȘ ROMANIA A CONTRIBUTION TO THE ETIOPATHOGENESIS, DIAGNOSIS AND MANAGEMENT OF SINONASAL INVERTED PAPILLOMAS PhD THESIS ABSTRACT PhD Student Viorel Emanoil
UNIVERSITY OF MEDICINE AND PHARMACY OF TÂRGU MUREȘ ROMANIA A CONTRIBUTION TO THE ETIOPATHOGENESIS, DIAGNOSIS AND MANAGEMENT OF SINONASAL INVERTED PAPILLOMAS PhD THESIS ABSTRACT PhD Student Viorel Emanoil
Undifferentiated Sinonasal Carcinoma Case Report
 Journal of Pharmacy and Pharmacology 7 (2017) 434-438 doi: 10.17265/2328-2150/2017.07.007 Undifferentiated Sinonasal Carcinoma Case Report Miroljub Todorovic 1 and Tanja Boljevic 2 1. Department of Ear,
Journal of Pharmacy and Pharmacology 7 (2017) 434-438 doi: 10.17265/2328-2150/2017.07.007 Undifferentiated Sinonasal Carcinoma Case Report Miroljub Todorovic 1 and Tanja Boljevic 2 1. Department of Ear,
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Founders Seminar. Handout material. Challenging Cases in Head and Neck Surgical Pathology
 Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
Founders Seminar Handout material Challenging Cases in Head and Neck Surgical Pathology Robert A. Robinson Department of Pathology University of Iowa American Academy of Oral and Maxillofacial Pathology
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
Inverted papilloma of the nasal cavity and paranasal sinuses: a study of 20 cases
 Original article: Inverted papilloma of the nasal cavity and paranasal sinuses: a study of 20 cases 1 Dr. Vijay Kumar Kalra, 2 Dr. Samar Pal Singh Yadav, 3 Dr. Swati 1Assistant Professor, 2 Senior Professor
Original article: Inverted papilloma of the nasal cavity and paranasal sinuses: a study of 20 cases 1 Dr. Vijay Kumar Kalra, 2 Dr. Samar Pal Singh Yadav, 3 Dr. Swati 1Assistant Professor, 2 Senior Professor
04/09/2018. Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances
 Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
Salivary Gland Pathology in the Molecular Era Old Friends, Old Foes, & New Acquaintances Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory
CASE REPORT Adult onset sinonasal rhabdomyosarcoma - a rare case report with cytohistological features
 Malaysian J Pathol 2016; 38(2) : 169 173 CASE REPORT Adult onset sinonasal rhabdomyosarcoma - a rare case report with cytohistological features Neelam SOOD MD Pathology and Nisha SEHRAWAT MD Pathology
Malaysian J Pathol 2016; 38(2) : 169 173 CASE REPORT Adult onset sinonasal rhabdomyosarcoma - a rare case report with cytohistological features Neelam SOOD MD Pathology and Nisha SEHRAWAT MD Pathology
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT
 NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Differential Diagnosis of Oral Masses. Palatal Lesions
 Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Differential Diagnosis of Oral Masses Palatal Lesions Palatal Masses Periapical Abscess Torus Palatinus Mucocele Lymphoid Hyperplasia Adenomatous Hyperplasia Benign Salivary Neoplasms Malignant Salivary
Scotland and Northern Ireland EQA Scheme. Circulation 46
 Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Scotland and Northern Ireland EQA Scheme Circulation 46 Special Educational Cases E1 and E2 Presented by Dr K Robertson Case E1 Female 42 year old with heavy menstrual and intermenstrual bleeding. IUS
Case 1. Disclosure. Imaging. Clinical history 5/10/2016. USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology
 Disclosure Dr. Agaram has nothing to disclose Case 1 Narsi Agaram, MBBS USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology Clinical history Imaging 1998 A three month
Disclosure Dr. Agaram has nothing to disclose Case 1 Narsi Agaram, MBBS USCAP 2016 Annual Meeting Evening Specialty Conference Bone and Soft tissue Pathology Clinical history Imaging 1998 A three month
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology
 David M. Parham, MD Chief of Anatomic Pathology") Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
Paranasal Sinuses: Neoplastic Lesions
 Pravin Mundada Department of Radiology, Geneva University Hospital, Switzerland Paranasal Sinuses: Neoplastic Lesions ESHNR 2017 Lisbon, Portugal Layout of the presentation Clinical & imaging features
Pravin Mundada Department of Radiology, Geneva University Hospital, Switzerland Paranasal Sinuses: Neoplastic Lesions ESHNR 2017 Lisbon, Portugal Layout of the presentation Clinical & imaging features
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
J of Evolution of Med and Dent Sci/ eissn , pissn / Vol. 3/ Issue 30/July 28, 2014 Page 8403
 BENIGN TUMOR OF NOSE AND PARANASAL SINUS IN A CHILD: A CASE REPORT Mujtaba Khan 1, S. Muneeruddin Ahmed 2, A. Sesha Prasad 3, M. Mahendra Kumar 4, G. Shahul Hameed 5 HOW TO CITE THIS ARTICLE: Mujtaba Khan,
BENIGN TUMOR OF NOSE AND PARANASAL SINUS IN A CHILD: A CASE REPORT Mujtaba Khan 1, S. Muneeruddin Ahmed 2, A. Sesha Prasad 3, M. Mahendra Kumar 4, G. Shahul Hameed 5 HOW TO CITE THIS ARTICLE: Mujtaba Khan,
PLEOMORPHIC ADENOMA OF LATERAL WALL OF NOSE A RARE PRESENTATION
 ISSN: 2250-0359 Volume 4 Issue 1 2014 PLEOMORPHIC ADENOMA OF LATERAL WALL OF NOSE A RARE PRESENTATION *USHA KUMAR MAHESH *RATNAKAR MADHAVARAO POTEKAR * B.L.D.E UNIVERSITY ABSTRACT: The aim of the article
ISSN: 2250-0359 Volume 4 Issue 1 2014 PLEOMORPHIC ADENOMA OF LATERAL WALL OF NOSE A RARE PRESENTATION *USHA KUMAR MAHESH *RATNAKAR MADHAVARAO POTEKAR * B.L.D.E UNIVERSITY ABSTRACT: The aim of the article
Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity
-deficient sinonasal carcinoma: a newly described entity") Int J Clin Exp Pathol 2016;9(3):3454-3458 www.ijcep.com /ISSN:1936-2625/IJCEP0024095 Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity Ming Zeng 1*, Changrong Chen 2*,
Int J Clin Exp Pathol 2016;9(3):3454-3458 www.ijcep.com /ISSN:1936-2625/IJCEP0024095 Case Report SMARCB1 (INI1)-deficient sinonasal carcinoma: a newly described entity Ming Zeng 1*, Changrong Chen 2*,
Disclosures. The Thin Red Line Between Neuropathology and Head & Neck Pathology. Introduction CASE 1. Current Issues Tihan
 Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
Disclosures I have nothing to disclose The Thin Red Line Between Neuropathology and Head & Neck Pathology Tarik Tihan, MD, PhD UCSF, Department of Pathology Neuropathology Division Introduction Three cases
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
Update in Salivary Gland Pathology. Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016
 Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Update in Salivary Gland Pathology Benjamin L. Witt University of Utah/ARUP Laboratories February 9, 2016 Objectives Review the different appearances of a selection of salivary gland tumor types Establish
Erica B. Wolfish Brenda L. Nelson Lester D. R. Thompson
 DOI 10.1007/s12105-011-0320-9 ORIGINAL PAPER Sinonasal Tract Mucoepidermoid Carcinoma: A Clinicopathologic and Immunophenotypic Study of 19 Cases Combined with a Comprehensive Review of the Literature
DOI 10.1007/s12105-011-0320-9 ORIGINAL PAPER Sinonasal Tract Mucoepidermoid Carcinoma: A Clinicopathologic and Immunophenotypic Study of 19 Cases Combined with a Comprehensive Review of the Literature
Salivary Gland FNA ATYPICAL : Criteria and Controversies
 Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
Salivary Gland FNA ATYPICAL : Criteria and Controversies W.C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital Massachusetts Eye and Ear Infirmary Harvard Medical School
CNS TUMORS. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
CNS TUMORS D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) CNS TUMORS The annual incidence of intracranial tumors of the CNS ISmore than intraspinal tumors May be Primary or Secondary
Experience with malignant tumours of the maxillary sinus in the Department of Otolaryngology Universiti Kebangsaan Malaysia, Kuala Lumpur
 Med. J. Malaysia Vol. 44 No. 1 March 1989 Experience with malignant tumours of the maxillary sinus in the Department of Otolaryngology Universiti Kebangsaan Malaysia, Kuala Lumpur S. Lokman, MD (UKMalaysia)
Med. J. Malaysia Vol. 44 No. 1 March 1989 Experience with malignant tumours of the maxillary sinus in the Department of Otolaryngology Universiti Kebangsaan Malaysia, Kuala Lumpur S. Lokman, MD (UKMalaysia)
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain
 December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
December 2016 59 yo male with past medical history of prostate carcinoma, presented with upper abdominal pain Contributed by: Divya Sharma, MD. Fellow, Gastrointestinal Pathology, Department of Pathology
PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies CYTOLOGIC DIAGNOSIS:
 1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
1 PRELIMINARY CYTOLOGIC DIAGNOSIS: Suspicious for Acinic Cell Carcinoma. Cell Block: Immunohistochemical Studies GCDFP-15 S-100 CYTOLOGIC DIAGNOSIS: Consistent with mammary analogue secretory carcinoma.
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Pathology of Selected Head and Neck Lesions. Adel Assaad MD Department of Pathology
 Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Pathology of Selected Head and Neck Lesions Adel Assaad MD Department of Pathology 1 NOSE Infections 2 Zygomycosis (Mucormycosis) Opportunistic infection caused by "bread mold fungi," including Rhizopus,
Pediatric Soft-Tissue Sarcomas. Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn
 Pediatric Soft-Tissue Sarcomas Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn Overview Histologic classifications Characteristic imaging features Helpful clinical characteristics
Pediatric Soft-Tissue Sarcomas Beth McCarville, MD St. Jude Children s Research Hospital Memphis, Tn Overview Histologic classifications Characteristic imaging features Helpful clinical characteristics
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Clinical analysis of 29 cases of nasal mucosal malignant melanoma
 1166 Clinical analysis of 29 cases of nasal mucosal malignant melanoma HUANXIN YU and GANG LIU Department of Otorhinolaryngology Head and Neck Surgery, Tianjin Huanhu Hospital, Tianjin 300060, P.R. China
1166 Clinical analysis of 29 cases of nasal mucosal malignant melanoma HUANXIN YU and GANG LIU Department of Otorhinolaryngology Head and Neck Surgery, Tianjin Huanhu Hospital, Tianjin 300060, P.R. China
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22
 Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
Squamous Cell Carcinoma of Thyroid: possible thymic origin, so-called ITET/CASTLE 2012/03/22 History of ITET/CASTLE First Report Gross Appearance and Prognosis 1) Miyauchi A et al: Intrathyroidal epithelial
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
SINONASAL RESPIRATORY EPITHELIAL ADENOMATOID HAMARTOMA: A REPORT ON THREE CASES.
 EUROMEDITERRANEAN BIOMEDICAL JOURNAL 2018,13 (12) 060 064 (FORMERLY: CAPSULA EBURNEA) Original article SINONASAL RESPIRATORY EPITHELIAL ADENOMATOID HAMARTOMA: A REPORT ON THREE CASES. Carmelo Saraniti
EUROMEDITERRANEAN BIOMEDICAL JOURNAL 2018,13 (12) 060 064 (FORMERLY: CAPSULA EBURNEA) Original article SINONASAL RESPIRATORY EPITHELIAL ADENOMATOID HAMARTOMA: A REPORT ON THREE CASES. Carmelo Saraniti
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Carcinoma mammario: le istologie non frequenti. Valentina Guarneri Università di Padova IOV-IRCCS
 Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Carcinoma mammario: le istologie non frequenti Valentina Guarneri Università di Padova IOV-IRCCS Histological diversity of breast adenocarcinomas Different histological types are defined according to specific
Human Papillomavirus and Head and Neck Cancer. Ed Stelow, MD
 Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Human Papillomavirus and Head and Neck Cancer Ed Stelow, MD No conflict of interest Declaration Cancer 1974 Lancet Oncol 2016; 17: e477-8 JAMA 1984; 252: 1857 JAMA 1988;259(13):1943-1944 Clin Cancer Res
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig
 Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Ocular Neoplasia What s Common? What s New? Richard R Dubielzig Orbit 288 6% Tumors of the globe make up 3225 out of 6110 total neoplasms = 53%. Tumors of the conjunctiva make up 1192 out of 6110 total
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY. F ZAHRA ALY, MD, PhD
 ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
ARIZONA SOCIETY OF PATHOLOGISTS 13 TH APRIL 2013 HEAD AND NECK CYTOPATHOLOGY F ZAHRA ALY, MD, PhD The main areas sites amenable for cytopathology include lymph nodes, thyroid, major salivary glands especially
Tumour Structure and Nomenclature. Paul Edwards. Department of Pathology and Cancer Research UK Cambridge Institute, University of Cambridge
 Tumour Structure and Nomenclature Paul Edwards Department of Pathology and Cancer Research UK Cambridge Institute, University of Cambridge Malignant Metastasis Core idea of cancer Normal Cell Slightly
Tumour Structure and Nomenclature Paul Edwards Department of Pathology and Cancer Research UK Cambridge Institute, University of Cambridge Malignant Metastasis Core idea of cancer Normal Cell Slightly
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Enterprise Interest None
 Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
Enterprise Interest None What are triple negative breast cancers? A synopsis of their histological patterns Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology,
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
HEAD AND NECK PATHOLOGY
 Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Bosnian-British School of Pathology November 2012 HEAD AND NECK PATHOLOGY Slide seminar: Oral Pathology Preferred Diagnoses Dr A Sandison, Slide seminar: Pathology of the Oral Cavity Page 1 of 5 1. Female
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome to Cutaneous Melanoma
 ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
WHO 2017: New Classification of Head and Neck Tumours
 WHO 2017: New Classification of Head and Neck Tumours Ilmo Leivo Department of Pathology University of Turku & Turku University Hospital FINLAND Suomen IAP Aulanko 18.05.2018 WHO 2017 New entities Simplification
WHO 2017: New Classification of Head and Neck Tumours Ilmo Leivo Department of Pathology University of Turku & Turku University Hospital FINLAND Suomen IAP Aulanko 18.05.2018 WHO 2017 New entities Simplification
Slide seminar. Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana
 Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Slide seminar Asist. Prof. Jože Pižem, MD, PhD Institute of Pathology Medical Faculty, University of Ljubljana Case 5 A 57-year-old man with a dermal/subcutaneous lesion on the scalp, which was interpreted
Basaloid neoplasms of the head and neck. Basaloid SCC. Clinico-pathologic features 5/5/11. Basaloid Tumors Head and Neck
 Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Basaloid neoplasms of the head and neck Richard Jordan DDS PhD FRCPath Professor & Director UCSF Oral Pathology Laboratory University of California San Francisco Basaloid Tumors Head and Neck Basaloid
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma
 Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
Keratinizing Dysplasia and Select Variants of Head & Neck Squamous Cell Carcinoma Napa Valley Pathology Conference Silverado Resort & Spa May 18, 2018 Bruce M. Wenig, MD Moffitt Cancer Center Tampa, FL
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification