Traumatic Brain Injury (TBI) night fear happy end. G. Adam, R. Radeva, G. Kirova
|
|
|
- Roberta Parker
- 5 years ago
- Views:
Transcription

")


1 Traumatic Brain Injury (TBI) night fear happy end G. Adam, R. Radeva, G. Kirova
2 Chapter 1 Night
3 10 th June hot summer night resident on call for 12 h Saturday Night 22:00 h call from the emergency department shouting... WE NEED A RADIOLOGIST FOR A CT IMMEDIATELY
4 Chapter 2 Fear Everything worth doing starts with being scared



5 While driving I wondered about several questions 1. What have happened? 2. Is it a child? 3. Is it going to be CT of: head abdomen /ileus/ aortic dissecation or? 4. Am I going to spot everything quickly? pexels


6 no information in the hospital system his name wasn t written > Unknown In the diagnostic imaging department (because no identity was presented) 10 people personnel came to the CT unit a little nightmare... Amazon.com
7 car accident 2 victims: 1 st conscious; 2 nd unconscious random people saw crashed car & stopped to help The story Patient (man, 23 y) was taken in car s truck & brought up in the nearest hospital Tokuda He was in coma, unstable hemodynamics, If you can t beat fear do it scared! non effective breathing, hematemesis GCS 3: wide nonreactive pupils; NO verbal/motor response Anesthesiologist intubated him
8 CT protocol traumatic patient Banksy 1. Head NATIVE 2.5 mm & mm reconstruction for bones VR (Volume Rendering) bones identify any focal intracranial lesions for neurosurgical intervention! 2. Cervical spine NATIVE From above C1 to T1 bottom + axial/sagittal/coronal view analysis 3. Chest /Abdomen/Pelvis (+ to knees in hemod. unstable) 2.5 mm CT + Contrast (because non contrast is of NO value) ALL (soft tissue/lung/bone) windows + Cor/Sag reconstruction for thoracic & lumbar spine
9 CT protocol traumatic patient Banksy Chest /Abdomen/Pelvis 1. NATIVE 2. + CONTRAST 1 st inject 70 ml 2 nd wait 20 sec. 3 rd inject 60 ml 4 th Scan In this way we have 2 in 1 (both arterial & venous phase)
10 Parents came & wanted to transfer their son in another hospital Police was expected to investigate the case Continued in the radiology department If the patient was going in another hospital than he needed CD with the CT examination Residents could not finish or sign examinations! And what if the patient died & the CT examination is confirmed & signed by a specialist on Monday (2 days later)?!

11 Then Or The Boss HELP call a friend the toast.net
12 Meanwhile what did I see?
13 Head CT of patient 10/06 Fractures calvaria & base: R parietal/temporal bone bilateral pyramid fractures sphenoidal bone clivus occpital bones sphenoidal sinus, ethmoidal cells & nose cavity with blood Intracranial changes: Pneumocephally Subarachnoid hemorrhage Brain edema; Mass effect

14 Fractures linear fracture R parietal bone


15 Fractures linear fracture R parietal/temporal bone


16 Fractures linear fracture R mastoid



17 Fractures linear fracture Left mastoid


18 Fractures multiple shpenoid bone


19 Fractures occipital till foramen magnum





20 Pneumocephally



21 lood content thmoid cells axillar sinus phenoid sinus

22 Blood content Mastoid cells
23 Subarachnoid hemorrhage

24 Brain edema



25 Mass effect effacement of basal cisterns

26 Neck CT C1 air in vert. canal T1
27 Control Head CT 1 day after 11/06 In comparison with the previous CT Better depicted fracture lines of calvaria, cranium s base bilaterally, through the mastoid processes to foramen magnum Blood dense content in sphenoid, maxillar sinuses & ethmoid cells Reduction of pneumocephally (frontal; sellar) Insignificant hemorrhage subarachnoid over tentorium & intraventricular under 3 rd ventricle Reduction of brain edema




28 Mastoid Sphenoid Clivus Occipital Control CT



29 Sinuses Blood content Control CT




30 Reduced: - brain edema - mass-effect - pneumocephally -SAH Control CT
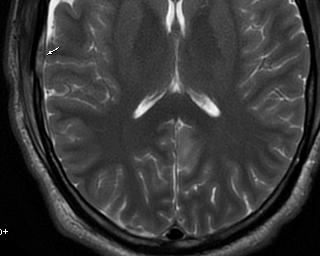
31 MRI 3 days after 13/06/17 Post contusion brain parenchyma changes Hemorrhagic changes in subacute phase Contusion: changed SI, restriction of diffusion Small SAH Hemorrhage: mesencephalon pons hypophysis suspicious (T1 high SI; T2 loss of SI) Reduced brain edema





32 frontal MRI parietal Postcontusion changes in brain parenchyma + Reduced brain edema occipital



33 MRI SAH tentor. R subdural



34 MRI SWI Hemorrhage Black mesencephalon pons Sonypictures.com hypophysis

35 MRI Blood content mastoid cells

36 Tonsillar position normal
37 Follow-up after 3 months 28/09/17 EEG Severe partial axonal damage of 3rd & 7th cranial nerve L

38 Chapter 3 Happy End
39 Follow-up after 1 month 03/10/17 EEG In norm for the age Small diffuse non specific changes
40 Follow-up after 1 month 15/11/17 Neurological examination control because of 3 rd & 7 th L cranial nerves deficit mouth angle is going upright persistence of left eye ptosis & double vision with subjective improvement GCS 15 Coordination & gait in norm No incontinence... for control MRI after 1 year

41 Don t stop dreaming just because you had a nightmare
42 Causes of TBI alteration in brain function or other evidence of brain pathology caused by an external force 1. falls 0 14 y; y 2. traffic acidents y 3. sports 4. military conflict situations (terrorist attacks) rise; blast injuries = complex injuries The Lancet Neurology Commission online Nov. 6, (17)30371 X
43 TBI Fall more often cause bruises (contusions) Traffic related injuries result in immediate shearing of connecting nerve fibres or progressive loss of connectivity over time 1. primary damage at the time of injury 2. secondary damage evolves over hours months/years; driven by host responses to the primary injury The Lancet Neurology Commission

44 15 (max.) GOOD Goergen S, Varma D, Tavender E, Rosenfeld JV, Cho S M, Whiteman I, et al. Adult Head Trauma. Education Modules for Appropriate Imaging Referrals: Royal Australian and New Zealand College of Radiologists; 2015
 BAD Goergen S, Varma D, Tavender E, Rosenfeld JV, Cho S M,")

45 In our patient GCS 3 3 (min.) BAD Goergen S, Varma D, Tavender E, Rosenfeld JV, Cho S M, Whiteman I, et al. Adult Head Trauma. Education Modules for Appropriate Imaging Referrals: Royal Australian and New Zealand College of Radiologists; 2015
 risk factor for epilepsy, stroke, late life neurodegenerative disease The Lancet Neurology Commission www.")
46 1. Mild (70 90% of pts) do not require surgery 2. Moderate 3. Severe high mortality rate (57,000/y in EU) risk factor for epilepsy, stroke, late life neurodegenerative disease The Lancet Neurology Commission online Nov. 6, (17)30371 X
47 Modality of choice for brain trauma in adults & children! Head CT in TBI NATIVE LOOK for: 1. Fractures 2. Hematomas 3. Mass effect
48 Head CT in TBI angiography only in cases: To diagnose blunt injury to vertebral or carotid arteries following: evidence of acute stroke on native CT scan fractures involving vertebral foramen transversarium
49 Acute trauma approach Outside in: (subcutaneous fractures hematomas brain) Fluid in sinuses > think of fractures Repeat CT when needed MRI after 1 week for DAI check
")
50 Gives greater anatomic detail of brain! DAI/TAI MRI (Diffuse axonal injury/traumatic axonal injury) Contusions Ischemia MRI CT VS.

51 Outside In Subcutaneous emphysema Subcutaneous hematoma
52 Outside In Fractures calvaria/base
 can expand rapidly Subdural venous (crescent)")
53 Outside In Hematomas 1.Extra-axial Epidural arterial (LEns) can expand rapidly Subdural venous (crescent) +bruised underlying brain Subarachnoid hemorrhage (Intraventricular)


")



54 1. Contusion: a focal area of parenchymal disruption (frontal & temporal) Intra-axial brain injury 2. Intraparenchymal hemorrhage 3. Diffuse Axonal Injury (MRI SWI) detecting scattered small hemorrhagic/nonhemor. lesions


55 1. Midline shift Mass effect 2. Cisternal compression 3. Stem compression
56 Take Home Messages Traumatic Brain Injury Be informed about the patient = Be well prepared! CT protocol: NATIVE: head Reconstruct in 0,625 & VR; cervical spine head+c only in suspicious carotid/vertebral pathology NATIVE + C: chest+abdomen+pelvis Reconstruct spine Don t forget to send the reconstructions in PACS Act quickly BUT think carefully
57 Have an approach for head injury Outside In Take Home Messages Traumatic Brain Injury 1. Fractures? 2. Hematomas/Hemorrhages? 3. Edema? 4. Mass effect? (hemorrhage/mass/edema) Look for SUBTLE changes Analyze in different windows & planes!
58 Take Home Messages Traumatic Brain Injury Do FOLLOW UP examinations: Head CT to notice changes Head MRI SWI after 1 week to detect DAI
59 Take Home Messages Traumatic Brain Injury Do NOT panic it won t help ;) patient s management is a complex process with many people involved > you are not alone in the decision making To err is human! Call a specialist when you hesitate better to share the nightmare Believe in yourself!



60 G. Adam, R. Radeva, G. Kirova
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
Imaging of Acute Cerebral Trauma
 July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
July, 2005 Imaging of Acute Cerebral Trauma Louis Rivera, Harvard Medical School, Year III 46 y/o Female s/p Trauma - Unrestrained? MVC requiring Med Flight - Facial bruising/swelling - DEEP COMA - SEIZURES
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
CASE 1. Female 21 years old DOL: November 28, 2016
 CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
CASE 1 Female 21 years old DOL: November 28, 2016 Injuries and Sequelae: GCS: 4 / 15 and coma for 3 weeks Multifocal intracranial hemorrhage at right thalamus and left frontal and temporal lobe Diffuse
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
TBI are twice as common in males High potential for poor outcome Deaths occur at three points in time after injury
 Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Head Injury Any trauma to (closed vs. open) Skull Scalp Brain Traumatic brain injury (TBI) High incidence Most common causes Falls Motor vehicle accidents Other causes Firearm- related injuries Assaults
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT
 The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
The Trauma Pan Scan A SYSTEMATIC APPROACH TO NOT KILLING THE PATIENT On-call duty Trauma patient Questions by ER doctors Questions by consultants What to do when you don t have time to think?! Questions
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Evaluation of Craniocerebral Trauma Using Computed Tomography
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 9 Ver. IV (Sep. 2014), PP 57-62 Evaluation of Craniocerebral Trauma Using Computed Tomography
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review
 Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
Neuroradiological Findings in Non- Accidental Trauma Educational Pictorial Review M B Moss, MD; L Lanier, MD; R Slater; C L Sistrom, MD; R G Quisling, MD; I M Schmalfuss, MD; and D Rajderkar, MD Contact:
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Introduction to Emergency Medical Care 1 OBJECTIVES 31.1 Define key terms introduced in this chapter. Slides 13 15, 17, 19, 28 31.2 Describe the components and function of the nervous system and the anatomy
Neuropathology Of Head Trauma. Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center
 Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
Neuropathology Of Head Trauma Mary E. Case, M.D. Professor of Pathology St. Louis University Health Sciences Center Nothing to disclose Disclosure Introduction 500,000 cases/year of serious head injury
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
PA SYLLABUS. Syllabus for students of the FACULTY OF MEDICINE No.2
 Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
Approved At the meeting of the Faculty Council Medicine No. of Approved At the meeting of the chair of Neurosurgery No. of Dean of the Faculty Medicine No.2 PhD, associate professor M. Betiu Head of the
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
THE ESSENTIAL BRAIN INJURY GUIDE
 THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
THE ESSENTIAL BRAIN INJURY GUIDE Neuroanatomy & Neuroplasticity Section 2 Contributors Erin D. Bigler, PhD Michael R. Hoane, PhD Stephanie Kolakowsky-Hayner, PhD, CBIST, FACRM Dorothy A. Kozlowski, PhD
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Louisiana State University Health Sciences Center
 Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Louisiana State University Health Sciences Center Department of Neurosurgery Student Clerkship Guide 2017 2018 Introduction Welcome to LSUHSC New Orleans neurosurgery rotation. Our department is dedicated
Medical Review Guidelines Magnetic Resonance Angiography
 Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
Medical Review Guidelines Magnetic Resonance Angiography Medical Guideline Number: MRG2001-05 Effective Date: 2/13/01 Revised Date: 2/14/2006 OHCA Reference OAC 317:30-5-24. Radiology. (f) Magnetic Resonance
41 year old female with headache. Elena G. Violari MD and Leo Wolansky MD
 41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
41 year old female with headache Elena G. Violari MD and Leo Wolansky MD ? Dural Venous Sinus Thrombosis with Hemorrhagic Venous Infarct Acute intraparenchymal hematoma measuring ~3 cm in diameter centered
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
North Oaks Trauma Symposium Friday, November 3, 2017
 + Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
+ Evaluation and Management of Facial Trauma D Antoni Dennis, MD North Oaks ENT an Allergy November 3, 2017 + Financial Disclosure I do not have any conflicts of interest or financial interest to disclose
Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience
 80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
80 Original Article THIEME Management Strategies for Communited Fractures of Frontal Skull Base: An Institutional Experience V. Velho 1 Hrushikesh U. Kharosekar 1 Jasmeet S. Thukral 1 Shonali Valsangkar
STROKE - IMAGING. Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli.
 STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
STROKE - IMAGING Dr RAJASEKHAR REDDY 2nd Yr P.G. RADIODIAGNOSIS KIMS,Narkatpalli. STROKE Describes a clinical event that consists of sudden onset of neurological symptoms Types Infarction - occlusion of
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Introduction to Neuroimaging spine. John J. McCormick MD
 Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #3 Penetrating Neck Trauma Penetrating neck injury (PNI) comprises 5 to 10 percent of traumatic injuries
Anatomy and Physiology 1 Chapter 7 self quiz Pro, Dima Darwish,MD.
 Anatomy and Physiology 1 Chapter 7 self quiz Pro, Dima Darwish,MD. 1) How many bones make up the axial skeleton? A) 50 B) 60 C) 70 D) 80 E) 90 2) Which of the following is a function of the axial skeleton?
Anatomy and Physiology 1 Chapter 7 self quiz Pro, Dima Darwish,MD. 1) How many bones make up the axial skeleton? A) 50 B) 60 C) 70 D) 80 E) 90 2) Which of the following is a function of the axial skeleton?
Head Injury כל הזכויות שמורות למד"א מרחב ירושלים. Dan Drory, EMT-P, Instructor
 Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
Head Injury Dan Drory, EMT-P, Instructor Anatomy on a fingertip The brain is a soft and gentle tissue. The brain is the most important organ. כל הזכויות שמורות למד"א מרחב ירושלים Protective layers of the
DR. SAAD AL-MUHAYAWI, M.D., FRCSC. ORL Head & Neck Surgery
 TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
TRAUMA IN ORL DR. SAAD AL-MUHAYAWI, M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgery TYPES OF TRAUMA EAR & TEMPORAL BONE TRAUMA NOSE & FACIAL BONES TRAUMA LARYNGEAL TRAUMA NECK TRAUMA
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Chapter 7: Head & Neck
 Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
Chapter 7: Head & Neck Osteology I. Overview A. Skull The cranium is composed of irregularly shaped bones that are fused together at unique joints called sutures The skull provides durable protection from
SUPPLEMENTARY FIG. S2. (A) Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as
 Risk of bias and applicability concerns graph by marker. Review authors judgments about each domain presented as") Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
Supplementary Data SUPPLEMENTARY FIG. S1. Graphical depiction of (A) influence and (B) outlier detection analyses of S100 calcium binding protein B (S100B) 0.10 0.11lg/L cutoff value studies. (C) Summary
A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage
 July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
July 2013 A Guide to the Radiologic Evaluation of Extra-Axial Hemorrhage John Dickson, Harvard Medical School Year III Agenda 1. Define extra-axial hemorrhage and introduce its subtypes 2. Review coup
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Pediatric CT Protocols (18 years old or less)
") Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
Pediatric CT Protocols (18 years old or less) Ped1: Head CT Ped2: Cervical spine CT Ped3: Sinus CT Ped4: Neck CT Ped5: Chest CT Ped6: Abdomen and pelvis CT Ped7: Thoracic or lumbar spine CT Ped8: Extremity
Mild Traumatic Brain Injury
 Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
Mild Traumatic Brain Injury Concussions This presentation is for information purposes only, not for any commercial purpose, and may not be sold or redistributed. David Wesley, M.D. Outline Epidemiology
ORIGINAL ARTICLE. Temporal Lobe Injury in Temporal Bone Fractures. imaging (MRI) to evaluate lesions of the temporal
 to evaluate lesions of the temporal") ORIGINAL ARTICLE Temporal Lobe Injury in Temporal Bone Fractures Richard M. Jones, MD; Michael I. Rothman, MD; William C. Gray, MD; Gregg H. Zoarski, MD; Douglas E. Mattox, MD Objective: To determine the
ORIGINAL ARTICLE Temporal Lobe Injury in Temporal Bone Fractures Richard M. Jones, MD; Michael I. Rothman, MD; William C. Gray, MD; Gregg H. Zoarski, MD; Douglas E. Mattox, MD Objective: To determine the
Trauma Overview. Chapter 1. Introduction. Epidemiology of Head Trauma. Etiology and Mechanisms of Injury
 Chapter 1 5 Overview is one of the most frequent indications for emergent neuroimaging. Because imaging plays such a key role in patient triage and management, we begin this book by discussing skull and
Chapter 1 5 Overview is one of the most frequent indications for emergent neuroimaging. Because imaging plays such a key role in patient triage and management, we begin this book by discussing skull and
Chapter 31. Objectives. Objectives 01/09/2013. Head Trauma
 Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 31 Head Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Correspondence should be addressed to Sorayouth Chumnanvej;
 Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
Neurology Research International Volume 2016, Article ID 2737028, 7 pages http://dx.doi.org/10.1155/2016/2737028 Research Article Assessment and Predicting Factors of Repeated Brain Computed Tomography
Benign brain lesions
 Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
Benign brain lesions Diagnostic and Interventional Radiology Hung-Wen Kao Department of Radiology, Tri-Service General Hospital, National Defense Medical Center Computed tomography Hounsfield unit (HU)
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
Pediatric Abusive Head Trauma
 Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Pediatric Abusive Head Trauma Rebecca Girardet Associate Professor of Pediatrics Director, Division of Child Protection Pediatrics McGovern Medical School at The University of Texas Health Science Center
Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2017/300 Clinical Outcome of Borderline Subdural Hematoma with 5-9 mm Thickness and/or Midline Shift 2-5 mm Raja S Vignesh
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of
 L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
L M Thornton, MD; L Lanier, MD; C L Sistrom, MD; D Rajderkar, MD; A Mancuso, MD; IM Schmalfuss, MD University of Florida, Gainesville Department of Radiology RSNA Annual Meeting 2016 Trainee call readiness
Attenuation value in HU From -500 To HU From -10 To HU From 60 To 90 HU. From 200 HU and above
 Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
Brain Imaging Common CT attenuation values Structure Air Fat Water Brain tissue Recent hematoma Calcifications Bone Brain edema and infarction Normal liver parenchyma Attenuation value in HU From -500
TRAUMATIC BRAIN INJURY. Moderate and Severe Brain Injury
 TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
TRAUMATIC BRAIN INJURY Moderate and Severe Brain Injury Disclosures Funded research: 1. NIH: RO1 Physiology of concussion 2016-2021, Co-PI, $2,000,000 2. American Medical Society of Sports Medicine: RCT
Post traumatic vertebro basilar dissection: case report and review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Post traumatic vertebro basilar dissection: case report and review of literature Karthikeyan Y.R., Sanjeev Chopra, Somnath Sharma,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Post traumatic vertebro basilar dissection: case report and review of literature Karthikeyan Y.R., Sanjeev Chopra, Somnath Sharma,
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Head injuries in children. Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead
 Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Head injuries in children Dr Jason Hort Paediatrician Paediatric Emergency Physician, June 2017 Children s Hospital Westmead Objectives Approach to minor head injury Child protection issues Concussion
Applicable Neuroradiology
 For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
For the Clinical Neurology Clerkship LSU Medical School New Orleans Amy W Voigt, MD Clerkship Director Introduction The field of Radiology first developed following the discovery of X-Rays by Wilhelm Roentgen
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas
 Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
Sanders: Mosby's Paramedic Textbook, Revised 3 rd Edition PowerPoint Lecture Notes Chapter 24: Head and Facial Traumas Chapter 24 Head and Facial Trauma Objectives Describe mechanism of injury, assessment,
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
PTA 106 Unit 1 Lecture 3
 PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
PTA 106 Unit 1 Lecture 3 The Basics Arteries: Carry blood away from the heart toward tissues. They typically have thicker vessels walls to handle increased pressure. Contain internal and external elastic
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
NEURO PROTOCOLS MRI NEURO PROTOCOLS (SIEMENS SCANNERS)
") Page 1 NEURO PROTOCOLS Brain Stroke Brain Brain with contrast Brain for seizures Brain for MS Brain for Pineal gland Sella FAST Scan for hydrocephalus MRA/MRV Brain MRA carotids 8 th nerve Cranial nerves
Page 1 NEURO PROTOCOLS Brain Stroke Brain Brain with contrast Brain for seizures Brain for MS Brain for Pineal gland Sella FAST Scan for hydrocephalus MRA/MRV Brain MRA carotids 8 th nerve Cranial nerves
How to Read a Head CT. Andrew D. Perron, MD, FACEP. Head CT. Head CT. Head CT. Head CT. EM Residency Program Director
 Blood Can Be Very Bad How to Read a Head CT EM Residency Program Director (or How I learned to stop worrying and love computed tomography ) Department of Emergency Medicine Maine Medical Center Portland,
Blood Can Be Very Bad How to Read a Head CT EM Residency Program Director (or How I learned to stop worrying and love computed tomography ) Department of Emergency Medicine Maine Medical Center Portland,
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017
 Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Neuroimaging of TBI: Current Clinical Guidelines and Future Direction Brain Injury Alliance of Colorado 2017 Peter E. Ricci, M.D. Staff Neuroradiologist Radiology Imaging Associates OBJECTIVES 1. Understand
Index. aneurysm, 92 carotid occlusion, 94 ICA stenosis, 95 intracranial, 92 MCA, 94
 A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
A ADC. See Apparent diffusion coefficient (ADC) Aneurysm cerebral artery aneurysm, 93 CT scan, 93 gadolinium, 93 Angiography, 13 Anoxic brain injury, 25 Apparent diffusion coefficient (ADC), 7 Arachnoid
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
ARTERIOVENOUS MALFORMATION OR CONTUSION : A DIAGNOSTIC DILEMMA. Yong Pei Yee, Ibrahim Lutfi Shuaib, Jafri Malin Abdullah*
 Malaysian Journal of Medical Sciences, Vol. 8, No. 2, July 2001 (47-51) CASE REPORT ARTERIOVENOUS MALFORMATION OR CONTUSION : A DIAGNOSTIC DILEMMA Yong Pei Yee, Ibrahim Lutfi Shuaib, Jafri Malin Abdullah*
Malaysian Journal of Medical Sciences, Vol. 8, No. 2, July 2001 (47-51) CASE REPORT ARTERIOVENOUS MALFORMATION OR CONTUSION : A DIAGNOSTIC DILEMMA Yong Pei Yee, Ibrahim Lutfi Shuaib, Jafri Malin Abdullah*
CT - the prime instrument for the critical. Critical Decisions & Critical Bleeds
 Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
Intracranial air on computerized tomography ANNE G. OSBORN, M.D., JONATHAN H. DAINES, M.D., S. DOUGLAS WING, M.D., AND ROBERT E. ANDERSON, M.D.
 J Neurosurg 48:355-359, 1978 Intracranial air on computerized tomography ANNE G. OSBORN, M.D., JONATHAN H. DAINES, M.D., S. DOUGLAS WING, M.D., AND ROBERT E. ANDERSON, M.D. Department of Radiology, University
J Neurosurg 48:355-359, 1978 Intracranial air on computerized tomography ANNE G. OSBORN, M.D., JONATHAN H. DAINES, M.D., S. DOUGLAS WING, M.D., AND ROBERT E. ANDERSON, M.D. Department of Radiology, University
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in