ESC / EACTS new valvular guidelines- Update
|
|
|
- Cori Goodman
- 6 years ago
- Views:
Transcription


1 ESC / EACTS new valvular guidelines- Update Yaron Shapira, MD The Dan Sheingarten echocardiography & valve clinic Rabin Medical Center, Beilinson Hospital, Petah-Tiqva Tel-Aviv University
2

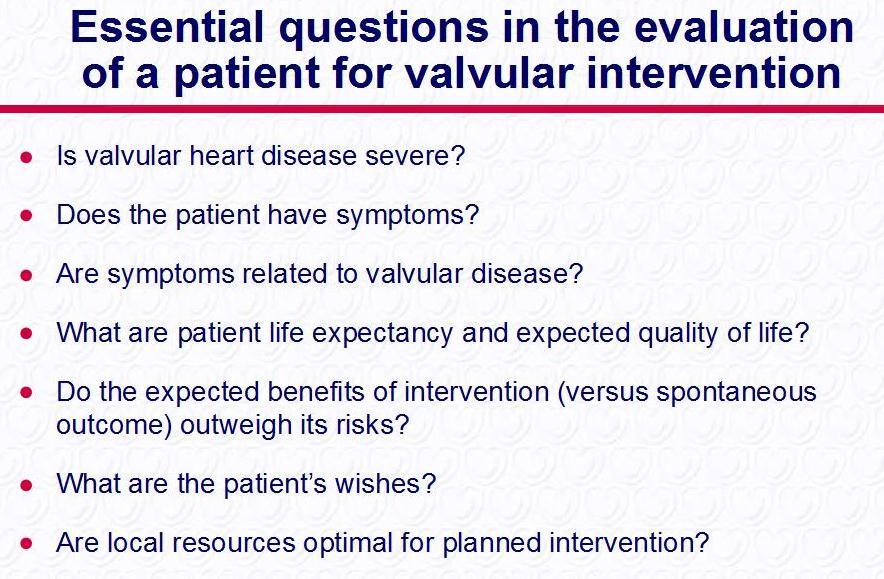
3 ESC valve guidelines 2007

4 AHA/ACC valve guidelines 2006/8
5
6
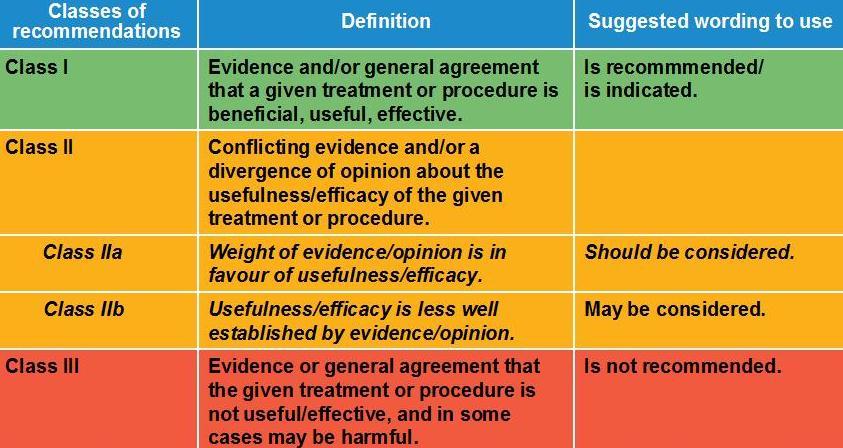
7 Level of evidence (LOE) LOE A Data derived from multiple RCTs or meta-analyses. # (in tables) 0 B C Data derived from a single RCT or large nonrandomized studies. Consensus of opinion of the experts and/ or small studies, retrospective studies, registries. 9 59
8
 Essential for TAV and mitraclip ESC/EACTS revascularization")
9 Heart team Heart team is encouraged (however unclassified for most entities) Essential for TAV and mitraclip ESC/EACTS revascularization 2010
10 Patient evaluation Diagnostic modalities Echo mainstay modality for the evaluation of VHD ndexing for BSA AS (>0.9 cm 2 /m 2 mild AS, <0.6 cm2/m 2 severe AS) AR (LVESD >25 mm/m 2 favors AVR) MR (LVESD >22 mm/m 2 favors MV repair) TR (Annulus >22 mm/m 2 favors TV annuloplasty) R/O inconsistencies between various echo parameters, mechanisms of disease, & clinical findings Exercise testing is encouraged
11 Patient evaluation Diagnostic modalities Exercise echo mainly for AS, MS, MR MR for LV Fx, valve regurgitation CTA for TAV
:1-25.")
12 Eur J Echocardiogr Jan;10(1):1-25.
13
14 ndications for TEE (TOE) When TTE is of suboptimal quality Susp. valve thrombosis Susp prosthetic dysfunction Susp endocarditis ntraprocedural in surgical valve repair or percutaneous procedures (incl. TAV, MitraClip, PMC) Assessment of aortic diameter for TAV Rarely helpful for AS quantification Exclude thrombi before PMC Detect SEC
15 Aortic stenosis
16 Aortic stenosis Severity AHA/ACC 2006/8 ESC 2007 ESC/EACTS 2012 Valve area (cm²) <1 <1 <1 ndexed valve area (cm²/m² BSA) <0.6 <0.6 <0.6 Mean gradient (mmhg) >40 >50 >40 Maximum jet velocity (m/s) >4 >4 Velocity ratio <0.25 Severe AS is unlikely if CO is normal and there is a mean pressure gradient <50 mmhg (ESC 2007)


17 Correlation between AVA, mean gradient & Vmax 3483 exams, 2427 pts, good LV AVA of 1.0 cm 2 correlated to a ΔP m of 21 mmhg and a V max of 3.3 m/s. ΔP m of 40 mmhg corresponds to an AVA of 0.75 cm 2 V max of 4.0 m/s to an AVA of 0.82 cm 2. Minners et al, EHJ 2008; 29:
18 Same pattern in invasive hemodynamics Minners et al, Heart 2010; 96:

19 Paradoxical low-flow AS Pibarot & Dumesnil, JACC 2012; 60:

20 Paradoxical low-flow AS
21 Prognosis of severe AS (AVA<1 cm 2 ) with good LV (EF>55%) according to flow & gradient 1ry outcome - Time to occurrence of 1 st composite endpoint: CV death or need for AVR motivated by the development of symptoms or LV systolic dysfunction (LVEF <50%). Gradient cutoff: 40 mmhg Flow cutoff: 35 cc/m 2 Lancellotti et al, JACC 2012; 59:
22 Natural History of AS Premature AVR (?)


23 Severe asymptomatic AS: Short-lived event-free prognosis Otto et al. Rosenhek et al Pellika et al
24 Early surgery in very severe AS Kang et al, Circulation. 2010;121: Rosenhek et al, Circulation. 2010;121:
25 Severe* Vs. Very severe ** AS Actuarial survival * Severe V max - 4-5m/s, Mean Gr mmhg, AVA ** Very severe - V max>5m/s, Mean Gr >50 mmhg, AVA<0.6 Kitai T et al, Heart 2011
26 Additional predictors of adverse outcome Heavy calcification + MPG Rosenhek 2000 MPG at exercise Lancellotti 2005 Natriuretic peptides (Bergler-Klein 2004)
27 ndications for AVR in severe symptomatic AS AHA/ACC Vs ESC/EACTS AHA/ACC 2006/8 ESC 2007 ESC/EACTS 2012 Severe symptomatic AS Low-flow, lowgradient (<40 mmhg) Good LV LV dysf, myocardial reserve (+) LV dysf, myocardial reserve (-) * * * - a b a a b
28 ndications for AVR in severe asymptomatic AS AHA/ACC Vs ESC/EACTS AHA/ACC 2006/8 ESC 2007 ESC/EACTS 2012 LV dysfunction Planned CABG / other valvular / aorta Symptoms during ETT b Predicted rapid progression b a a Hypotension during ETT b a a Critical AS, predicted mortality <1% b - a High-grade arrhythmia during ETT - b - Severe LVH W/O HTN - b b High Natriuretic peptide - - b Mean gradient by >20 mmhg during ETT - - b

29 ndications for AVR in non-severe AS AHA/ACC Vs ESC/EACTS AHA/ACC 2006/8 ESC 2007 ESC/EACTS 2012 Moderate AS, Planned CABG / other valvular / aorta a a a Mild AS, planned CABG, rapid progression expected b - -

30 ESC/EACTS guidelines for AS ac: Vmax >5.5m/s; severe valve calcification + peak velocity progression 0.3 m/s/year. bc: markedly elevated natriuretic peptide levels; mean gradient increase with exercise >20 mmhg; excessive LVH
31 Avoiding patient-prosthesis mismatch (PPM) in AVR f the valve prosthesis patient ratio is expected to be,0.65 cm 2 /m 2 BSA, enlargement of the annulus to allow placement of a larger prosthesis may be considered

32 Trans-catheter aortic valve implantation (TAV)
33

34 ndications for TAV ESC/EACTS 2012 * ** * PARTNER cohort B ** PARTNER cohort A
35 Risk assessment for savr Current scores: Good discrimination Poor calibration in high-risk pts. (overestimation) Logistic EuroSCORE >20% (overestimation) STS score >10% (more realistic) Factors not included in current scores: Frailty Porcelain aorta History of chest radiation Patent coronary bypass grafts ncorporate scores, but always use clinical judgment in addition
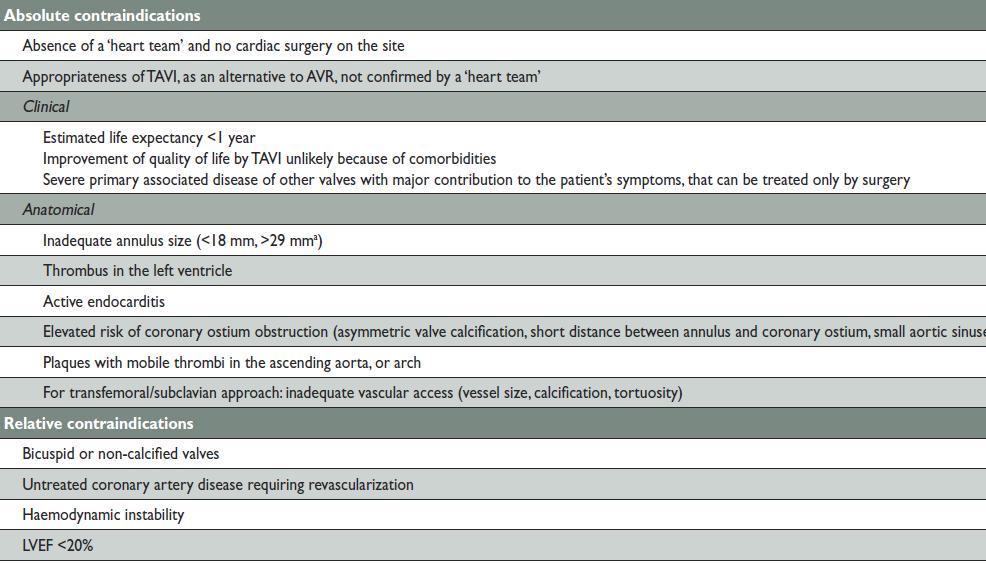
36 C to TAV

37 Leon M, TCT 2012
38 DAPT after TAV Low-dose aspirin + a thienopyridine (DAPT) is used early after TAV and MitraCLip Later - aspirin or a thienopyridine alone. Remarks: Lack of evidence Duration of DAPT -?? n patients in AF, a combination of VKA and aspirin or thienopyridine is generally used, but should be weighed against increased risk of bleeding.
39 Aortic regurgitation
40
41 ndications for surgery in chronic severe AR AHA/ACC Vs ESC/EACTS Symptomatic (NYHA 2-4) AHA/ACC ESC/EACTS 2007/12 LVEF <50% Planned operation - CABG / aorta / other valve Marked LV dilatation a LV > 75/55 a LV > 70/50 (ESD>25 mm/m 2 ) Moderate LV dilatation (70-75/50-55) b -
42 (mm/y) Marfan BAV Other Surgery for aortic dilatation Comparison of guidelines Aorta (American) 2010 > >40 (desired pregnancy) AHA/ACC VHD 2006/8 >5 >45 >40 (desired pregnancy) ESC 2007 > ESC/EACTS 2012 > (RF)* 55 ( 50+RF)** 55 * FH of aortic dissection and/or aortic size >2 mm/year, severe AR or MR, desire of pregnancy. ** FH of dissection aortic diameter >2 mm/year, coarctation, HTN Comparison of values: same technique, same level, side-by-side, confirmed by additional modality Lower threshold if AVR is undicated
43 Mitral stenosis (MS) Unchanged from 2007 ESC guidelines
44 Mitral regurgitation
45 LV dysfunction in 1 ry MR Normal Mild-moderate LV Dx Severe LV Dx LVEF >60% 30-60% <30% LVESD (mm) <40*/45** 40*/45**-55 >55 * AHA/ACC ** ESC/EACTS
46 Symptomatic 1 ry MR AHA/ACC ESC ESC/EACTS 2006/ Good LV Mild-moderate LV Dx Severe LV Dx, resistant to medical Tx, high likelihood of repair, W/O significant co-morbidity a a a Severe LV Dx, resistant to medical Tx, low likelihood of repair, W/O significant co-morbidity b b
47 Asymptomatic 1 ry MR AHA/ACC ESC ESC/EACTS 2006/ Mild-moderate LV Dx Good LV, AF* or PAP>50 a a a Good LV, high likelihood of repair, low operative risk Any LVESD LVESD>40 mm LA volume >60 cc/m 2 a - b - - a ** b PAP>60 mmhg at exercise a - b *new onset AF (AHA/ACC, ESC 2012) ** flail leaflet
48 Asymptomatic 1 ry MR LVEF>60%, high likelihood of repair, low predicted mortality < >45 AHA/ACC a ESC ESC/EACTS a

49 2 ry MR (Functional MR FMR)
50 Surgery for FMR MR severity LVEF Need for revascularization Class Severe >30% (CABG) Moderate (CABG) a Severe <30% (+) a Severe >30% (-) b Repair whenever possible

51 Predictors of late failure of MV repair for FMR LVEDD >65 mm, PML angle >45º Distal AML angle >25º Systolic tenting area >2.5 cm 2, Coaptation distance >10 mm End-systolic interpapillary muscle distance >20 mm Systolic sphericity index >0.7
52 Surgery for FMR Unproved survival benefit No head-to-head comparison between repair & MVR Better results if CABG required (look for ischemia & viability)

53 MitraClip b indication, LOE C Less effective than surgical MV repair Candidates: Severe symptomatic 2 ry MR Failure of OMT (incl. CRT) Fulfillment of echo criteria noperable / high risk for surgery (Heart Team)
54 Tricuspid regurgitation
55 ndications for tricuspid surgery TR Type Severity AHA/ACC 2006/8 ESC 2007 ESC/EACTS ry/2ry Severe While undergoing left-sided valve surgery 1ry Moderate While undergoing left-sided valve surgery b ** a a 2ry Mild or moderate Dilated annulus ( 40 mm or >21 mm/m² *) in pts. undergoing left-sided valve surgery. b a a 1ry Severe Symptomatic, isolated TR without severe RV dysfunction a *** 1ry Severe Asymptomatic or mildly symptomatic patients with progressive RV dilatation or deterioration of RV function. - b a Any Severe After left-sided valve surgery, symptomatic patients / progressive RV dilatation/dysfunction, in the absence of left-sided valve dysfunction, severe right or left ventricular dysfunction, and severe pulmonary vascular disease. - a a * 21 mm/m 2 = 36 mm for BSA=1.7 ** f PHT or dilated annulus *** Despite medical Tx
56 Valve choice according to the desire of the informed patient (Class ) valve in valve not yet included in decision algorithms
57 Age limits for valve choice (a recommendation for all) AVR < >70 AHA/ACC Mech Mech Biol ESC 2007 Mech Mech Either Biol ESC/EACTS 2012 Mech Either Biol
58 Age limits for valve choice (a recommendation for all) MVR < >70 AHA/ACC Mech Biol ESC 2007 Mech Either Biol ESC/EACTS 2012 Mech Either Biol
59 Arguments in favor of a mechanical valve (beyond age) AHA/ACC 2006/8 ESC 2007 ESC 2012 Risk of accelerated SVD (age,40, PTH ) Already on OAC D/T an additional mechanical valve (AVR) When re-do is too risky a a * Already on OAC D/T high-risk of TE a ** a b * f life expectancy >10y ** MVR + AF
60 Arguments in favor of a biological valve (beyond age) AHA/ACC 2006/8 ESC 2007 ESC 2012 Cannot / will not take OAC Re-do for mechanical valve thrombosis despite therapeutic NR - - Re-do for mechanical valve thrombosis with proven subtherapeutic NR - - When re-do is at low risk - a a * Young women contemplating pregnancy. - b a * f life expectancy >10y
61 OAC / aspirin after valve replacement Low-dose aspirin (on top of OAC) selective in ESC guidelines (failure of therapeutic NR, atherosclerosis), mandatory in AHA/ACC guidelines. No need for life-long aspirin in low-risk patients with bioprosthetic valves in ESC guidelines (mandatory in AHA/ACC guidelines)
62 OAC / aspirin after valve replacement Lifelong OAC for all pts. with a mechanical prosthesis. Lifelong OAC for pts. with bioprostheses who have other indications for anticoagulation. Addition of aspirin* in all pts. with a mechanical biological prosthesis regardless of concomitant OAC, valve position and risk profile Addition of aspirin* in pts. with a mechanical prosthesis and concomitant atherosclerotic disease. Addition of aspirin* in pts. with a mechanical prosthesis after thromboembolism despite adequate NR. OAC for the first 3 months after implantation of a mitral- or tricuspid bioprosthesis. OAC for the first 3 months after mitral valve repair. Aspirin* for the first 3 months after implantation of an aortic bioprosthesis. OAC for the first 3 months after implantation of an aortic bioprosthesis. AHA/ACC a ESC/EACTS a a a a a b * low-dose

63 NR target ESC 2007, ESC/EACTS 2012 Vale position AVR MVR Low-risk AHA/ACC 2006/8 High-risk

64 Novel oral anticagulants (NOAC) (a or Xa inhibitors) The substitution of vitamin K antagonists by direct oral inhibitors of factor a or Xa is not recommended in patients with a mechanical prosthesis, because specific clinical trials in such patients are not available at this time.
65 Bridging therapy AHA/ACC Esc 2007 ESC/EACTS 2012 V UFH a LMWH b b a
66 Questionable issues Prophylactic re-replacement of xenograft >10 Y/O without SVD during open-heart surgery (b) MSCT may be useful in excluding CAD in patients who are at low risk of atherosclerosis (no classification)
67 Gaps and challenges Elaboration and validation of improved risk scoring systems for predicting outcomes after valve surgery and interventional procedures. The prognostic impact and diagnostic value of stress echocardiography should be further evaluated. Long term results of aortic valve repair. The potential role of TAV in intermediate risk patients with AS and that of MitraClip in high risk patients with secondary MR.
68 Gaps and challenges (cont d) The indications for intervention in asymptomatic patients with AS or MR should be further evaluated. Controlled clinical trials to better define the modalities of early anticoagulant therapy after valve replacement using a mechanical prosthesis, a bioprosthesis in aortic position or after TAV. The usefulness of direct oral inhibitors of factor a or Xa in patients with a mechanical prosthesis. Valve-in-valve
69 Key notes Collaboration with surgeons (Heart Team). Risk stratification. TAV (PARTNER-like pts). Paradoxical low-flow AS. Asymptomatic critical AS. Higher thresholds for replacement of aorta. Lower LVESD for MV repair in low-risk 1 ry MR MitraClip for FMR Reduced age limits for biological AVR ASA instead of OAC early after biological AVR

70
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
2017 ESC/EACTS Guidelines for the management of valvular heart disease
 2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
2017 ESC/EACTS Guidelines for the management of valvular heart disease Prof. Fausto J. Pinto, FESC, FACC Immediate ESC Past President Head, Cardiology Dpt/ University Hospital Sta Maria-HPV University
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Valvular Guidelines: The Past, the Present, the Future
 Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Guidelines: The Past, the Present, the Future Robert O. Bonow, MD, MS Northwestern University Feinberg School of Medicine Bluhm Cardiovascular Institute Northwestern Memorial Hospital Editor-in-Chief,
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Spotlight on Valvular Heart Disease Guidelines
 Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Spotlight on Valvular Heart Disease Guidelines Aortic Valve Disease Raphael Rosenhek Department of Cardiology Medical University of Vienna Palermo, April 26 th 2018 1998 2002 2006 2007 2008 2012 2014 2017
Low Gradient Severe? AS
 Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Low Gradient Severe? AS Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de Québec / Québec Heart
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Potential conflicts of interest
 Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Potential conflicts of interest Speaker's name: Petros Dardas MEDTRONIC proctor for TAVI Intermediate risk 83 FEMALE COAD SEVERE AS NYHA III Mean gradient 35 mmhg, AVA 0.45cm2, SVI 21ml/m2 Paradoxical
Severe aortic stenosis should be operated before symptom onset CONTRA. Helmut Baumgartner
 Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Severe aortic stenosis should be operated before symptom onset CONTRA Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center Dept. of Cardiology
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France
 Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Management of significant asymptomatic aortic stenosis. Alec Vahanian Bichat Hospital University Paris VII Paris, France Background Aortic stenosis (AS) is the most frequent valve disease among referred
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives. Bernard Iung Bichat Hospital, Paris
 Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Percutaneous Treatment of Valvular Heart Diseases: Lessons and Perspectives Bernard Iung Bichat Hospital, Paris Euro Heart Survey on Valvular Diseases 3547 Patients with Native Valve Disease n= 1250 1000
Sténose aortique à Bas Débit et Bas Gradient
 3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
3.6 m/s Sténose aortique à Bas Débit et Bas Gradient Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Doctorate Honoris Causa, Université de Liège Institut
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Outcome of elderly patients with severe but asymptomatic aortic stenosis
 Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Outcome of elderly patients with severe but asymptomatic aortic stenosis Robert Zilberszac, Harald Gabriel, Gerald Maurer, Raphael Rosenhek Department of Cardiology Medical University of Vienna ESC Congress
Assessment and Preparation of Patients with TAVI. Rob Tanzola Associate Professor, Queen s University
 Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Assessment and Preparation of Patients with TAVI Rob Tanzola Associate Professor, Queen s University My patient has aortic stenosis and needs non-cardiac surgery Should (s)he get a TAVI? Rob Tanzola Associate
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid
 Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Reshape/Coapt: do we need more? Prof. J Zamorano Head of Cardiology University Hospital Ramon y Cajal, Madrid Patient records 76 y.o. male Hypertension. Dyslipidemia. OPLD. Smoked in the past. Diabetes
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Late secondary TR after left sided heart disease correction: is it predictibale and preventable
 Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Late secondary TR after left sided heart disease correction: is it predictibale and preventable Gilles D. Dreyfus Professor of Cardiothoracic surgery Nath J, et al. JACC 2004 PREDICT Incidence of secondary
Aortic Valvular Stenosis
 Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
Aortic Valvular Stenosis How to Assess the Four Variables for Management Low Flow / Low Gradient / Normal EF / Low EF Patrick T. O Gara, MD, MACC Brigham and Women s Hospital Harvard Medical School No
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Understanding the guidelines for Interventions in MR. Ali AlMasood
 Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Understanding the guidelines for Interventions in MR Ali AlMasood Mitral regurgitation The most diverse from all acquired valve diseases About 50% of patients with an LVEF 35 percent had moderate to severe
Low Gradient AS: Multi-Imaging Modalities
 Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Low Gradient AS: Multi-Imaging Modalities Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Institut Universitaire de Cardiologie et de Pneumologie de
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular heart disease (VHD) is present in 2.5% of the
 is present in 2.5% of the") 2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
ESSENTIAL MESSAGES FROM
 ESSENTIAL MESSAGES FROM ESC GUIDELINES Committee for Practice Guidelines To improve the quality of clinical practice and patient care in Europe VHD ESC/EACTS Guidelines ON the Management OF VALVULAR HEART
ESSENTIAL MESSAGES FROM ESC GUIDELINES Committee for Practice Guidelines To improve the quality of clinical practice and patient care in Europe VHD ESC/EACTS Guidelines ON the Management OF VALVULAR HEART
Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO!
 ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
ESC 2011, Paris Controversies in Low-Flow, Low-Gradient Aortic Stenosis Aortic Valve Replacement Improves Outcome in Patients with Preserved Ejection Fraction: PRO! Philippe Pibarot, DVM, PhD, FACC, FAHA,
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Transcatheter aortic valve implantation and pre-procedural risk assesment
 Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Transcatheter aortic valve implantation and pre-procedural risk assesment Alec Vahanian,FESC, FRCP(Edin.) Bichat Hospital University Paris VII, Paris, France Disclosures Relationship with companies who
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines. Christophe Tribouilloy Amiens, France
 Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Mitral Valve prolapse: What s new? Which indications of early surgery? Input of new 2017 ESC/EACTS guidelines Christophe Tribouilloy Amiens, France I have no financial relationships to disclose related
Load and Function - Valvular Heart Disease. Tom Marwick, Cardiovascular Imaging Cleveland Clinic
 Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
Load and Function - Valvular Heart Disease Tom Marwick, Cardiovascular Imaging Cleveland Clinic Indications for surgery in common valve lesions Risks Operative mortality Failed repair - to MVR Operative
TAVI Versus Suturless Valve In Intermediate Risk Patients
 TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI Versus Suturless Valve In Intermediate Risk Patients Walid Abukhudair FRCSc President of Saudi Society for Cardiac Surgeons Head of Cardiac Surgery in KFAFH Background AS is the most frequent cardiac
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal
 Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Valve Disease in Patients With Heart Failure TAVI or Surgery? Miguel Sousa Uva Hospital Cruz Vermelha Lisbon, Portugal I have nothing to disclose. Wide Spectrum Stable vs Decompensated NYHA II IV? Ejection
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
 Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat Innovative Procedures, Devices & State of the Art Care for Arrhythmias, Heart Failure & Structural Heart Disease October 8-10,
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Severe left ventricular dysfunction and valvular heart disease: should we operate?
 Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Severe left ventricular dysfunction and valvular heart disease: should we operate? Laurie SOULAT DUFOUR Hôpital Saint Antoine Service de cardiologie Pr A. COHEN JESFC 16 janvier 2016 Disclosure : No conflict
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor
 Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Low Gradient Severe AS: Who Qualifies for TAVR? Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University
Aortic stenosis with concomitant mitral regurgitation
 Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Challenges in the evaluation and management of aortic stenosis Aortic stenosis with concomitant mitral regurgitation S1 Philippe Unger, M.D., FESC Erasme Hospital - Université Libre de Bruxelles Brussels,
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain
 Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
Eulogio Garcia MD Hospital Clínico San Carlos Madrid - Spain Device Landscape 2010 PERCUTANEOUS TECHNIQUES Percutaneous indirect annuloplasty Percutaneous direct annuloplasty Edge to Edge ( E-Valve ) Non
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Organic mitral regurgitation
 The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
The best in heart valve disease Organic mitral regurgitation Ewa Szymczyk Department of Cardiology Medical University of Lodz, Poland I have nothing to declare Organic mitral regurgitation leaflet abnormality
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Management of Valvular Heart Disease. Management of Valvular Heart Disease
 Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017
 Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Disclosures: GE stock, Primary Mitral Valve Disease: Natural History & Triggers for Intervention ACC Latin American Conference 2017 Athena Poppas, MD FACC Past ACC Scientific Sessions Chair, ACC Board
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute
 Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Indicator Mild Moderate Severe
 Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Indicator Mild Moderate Severe Jet velocity (m/s) 2.0-2.9 3.0-3.9 4.0 Mean gradient (mmhg) < 20 20-39 40 Valve area (cm 2 ) 1.0 Valve area index (cm 2 /m 2 ) 0.6 1 Abnormal AV with Reduced Systolic Opening
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France
 Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
Measuring the risk in valve patients Lessons learnt from the TAVI story? Bernard Iung Bichat Hospital, Paris, France Faculty disclosure Bernard Iung I disclose the following financial relationships: Consultant
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives. Martin B. Leon, MD
 The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
The Changing Epidemiology of Valvular Heart Disease: Implications for Interventional Treatment Alternatives Martin B. Leon, MD Columbia University Medical Center Cardiovascular Research Foundation New
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease
 2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
2017 Update to the AHA/ACC Guideline for Management of Mitral Valve Disease Patrick T. O Gara, MD BWH Heart and Vascular Center Professor of Medicine, Harvard Medical School Disclosures NHLBI CTSN Co-chair
Interventional Updates 2016
 nterventional Updates 2016 Matthew Johnson, MD Dual Antiplatelet Therapy (DAPT ) What is the newest. Can they ever make up there minds???? What is new in the world of TAVR 1 New risk MitraClip getting
nterventional Updates 2016 Matthew Johnson, MD Dual Antiplatelet Therapy (DAPT ) What is the newest. Can they ever make up there minds???? What is new in the world of TAVR 1 New risk MitraClip getting
Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère asymptomatique de type dégénérative?
 Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Réunion d automne de la SSC à Lucerne le 24.11.2011 Incertitudes dans le travail cardiologique quotidien Les valvulopathies en sourdine: la valve mitrale Quoi faire devant une régurgitation mitrale sévère
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Aortic Regurgitation & Aorta Evaluation
 VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
VALVULAR HEART DISEASE Regurgitation Valvular Lessions 2017 Aortic Regurgitation & Aorta Evaluation Jorge Eduardo Cossío-Aranda MD, FACC Chairman of Outpatient Care Department Instituto Nacional de Cardiología
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV?
 Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Aortic Stenosis: Interventional Choice for a 70-year old- SAVR, TAVR or BAV? Interventional Choice for a 90-year old- SAVR, TAVR or BAV? Samin K Sharma, MD, FACC, FSCAI Director Clinical & Interventional
Low Gradient AS Normal LVEF
 Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Low Gradient AS Normal LVEF Shahbudin H. Rahimtoola MB, FRCP, MACP, MACC, FESC, D.Sc.(Hon) Distinguished Professor University of Southern California Griffith Professor of Cardiology Professor of Medicine
Worldwide rheumatic fever is the most common cause of valve disease. In industrialized areas, valvular disease of old age predominates
 Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
Michael Sumners DO Epidemiology Worldwide rheumatic fever is the most common cause of valve disease In industrialized areas, valvular disease of old age predominates Calcific aortic stenosis Functional
VALVULAR HEART DISEASE AND PULMONARY CIRCULATION
 ESC CONGRESS HIGHLIGHTS VALVULAR HEART DISEASE AND PULMONARY CIRCULATION N. Ajmone Marsan (Leiden, NL) MD, PhD, FESC Conflicts of Interest None CONTENTS Pulmonary arterial hypertension Rheumatic heart
ESC CONGRESS HIGHLIGHTS VALVULAR HEART DISEASE AND PULMONARY CIRCULATION N. Ajmone Marsan (Leiden, NL) MD, PhD, FESC Conflicts of Interest None CONTENTS Pulmonary arterial hypertension Rheumatic heart
The best in heart valve disease Aortic valve stenosis
 The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
The best in heart valve disease Aortic valve stenosis Marie Moonen, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM My declaration of interest : I have nothing to declare Prevalence
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Β. Κόλλιας, Σ. Ματιάτου, Δ. Αγγουράς.
 Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Rapid deployment aortic valve replacement for the treatment of severe aortic stenosis in high risk patients. Οι βιοπροσθετικές αορτικές βαλβίδες ταχείας έκπτυξης στην αντιµετώπιση της σοβαρής αορτικής
Valvular Intervention
 Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
Valvular Intervention Outline Introduction Aortic Stenosis Mitral Regurgitation Conclusion Calcific Aortic Stenosis Deformed Eccentric Calcified Nodular Rigid HOSTILE TARGET difficult to displace prone
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων. Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος
 Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
Επιδιόπθωζη μιηποειδικήρ ζςζκεςήρ ζε ππόπηωζη ή πήξη γλωσίνων Βαζίλειορ Σασπεκίδηρ Επιμεληηήρ Β Καπδιολογίαρ Γ.Ν. Παπαγεωπγίος MV anatomy Otto C. NEJM 2001 Leaflets anatomy 2% of population Etiology Terminology
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH
 TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
TRANSCATHETER AORTIC VALVE IMPLANTATION: PSCC EXPERIENCE DR HUSSEIN ALAMRI PSCC RIYADH Available systems: Edwards (TA and TF) and Core valve. INTRODUCTION 3 4% 0f > 65 y. 30 40% of elderly denied surgery,.
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.
, FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia.") Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC President of Saudi Heart Association King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia. Decision process for Management of any valve Timing Feasibility
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
Pregnancy, Heart Disease and Imaging. Hemodynamics. Decreased systemic vascular resistance. Physiology anemia
 Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Pregnancy, Heart Disease and Imaging Sangeeta Shah, MD, FASE, FACC Associate Professor, Ochsner Clinical School of Medicine Advanced CV Imaging and Adult Congenital Heart Disease New Orleans, LA Hemodynamics
Corrective Surgery in Severe Heart Failure. Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio
 Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
Corrective Surgery in Severe Heart Failure Jon Enlow, D.O., FACS Cardiothoracic Surgeon Riverside Methodist Hospital, Ohiohealth Columbus, Ohio Session Objectives 1.) Identify which patients with severe
TAVR SPRING 2017 The evolution of TAVR
 TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
TAVR SPRING 2017 The evolution of TAVR Matthew Johnson, MD Disclosers None Evolution of the Balloon- Expandable Transcatheter Valves Cribier 2002 SAPIEN 2006 SAPIEN XT 2009 SAPIEN 3 2013 * Sheath compatibility
Introducing the COAPT Trial
 physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
physician INFORMATION Eligible patients Symptomatic functional mitral regurgitation 3+ Not suitable candidates for open mitral valve surgery NYHA functional class II, III, or ambulatory IV Introducing
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management
 Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Who will Benefit from Percutaneous Management of Mitral Regurgitation? An Imaging Guide to Management James D. Thomas, M.D., F.A.C.C. Department of Cardiovascular Medicine Heart and Vascular Institute
Index. B B-type natriuretic peptide (BNP), 76
, 76") Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Index A ACCESS-EU registry, 158 159 Acute kidney injury (AKI), 76, 88 Annular enlargement, RV, 177 178 Annuloplasty chordal cutting, 113 complete ring, 99 etiology-specific ring, 100 evolution, 98 flexible
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine
 Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Chapter 24: Diagnostic workup and evaluation: eligibility, risk assessment, FDA guidelines Ashwin Nathan, MD, Saif Anwaruddin, MD, FACC Penn Medicine Mitral regurgitation, regurgitant flow between the
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee
 - 5 important lessons learnt from HK experiences Michael KY Lee") Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Transcatheter Aortic Valve Implantation (TAVI) - 5 important lessons learnt from HK experiences Michael KY Lee Queen Elizabeth Hospital, Hong Kong President, HKSTENT APCASH 2013 SJ Park TAVI Summit 2013
Learn and LiveSM. ACC/AHA Pocket Guideline. Based on the ACC/AHA 2006 Guideline Revision. Management of Patients With. Valvular Heart Disease
 Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
2/15/2018 DISCLOSURES OBJECTIVES. Consultant for BioSense Webster, a J&J Co. Aortic stenosis background. Short history of TAVR
 TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
TRANSCATHETER AORTIC VALVE REPLACEMENT IN 2018: IS IT NOW THE STANDARD OF CARE? 22 ND ANNUAL COASTAL CARDIAC & VASCULAR CONFERENCE FEBRUARY 17, 2018 R. David Anderson, MD, MS, FACC, FSCAI Professor of
Reverse left atrium and left ventricle remodeling after aortic valve interventions
 Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
Reverse left atrium and left ventricle remodeling after aortic valve interventions Alexandra Gonçalves, Cristina Gavina, Carlos Almeria, Pedro Marcos-Alberca, Gisela Feltes, Rosanna Hernández-Antolín,
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream
 Going Mainstream") The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org
The Mitral Revolution: Transcatheter Repair (and Replacement?) Going Mainstream Matthew J. Price MD Director, Cardiac Catheterization Laboratory Scripps Clinic La Jolla, CA, USA price.matthew@scrippshealth.org