Dr. Peter Hutten-Czapski HAILEYBURY ON 169
|
|
|
- Kerrie Bryant
- 5 years ago
- Views:
Transcription
1 Society of Rural Physicians of Canada 26TH ANNUAL RURAL AND REMOTE MEDICINE COURSE ST. JOHN'S NEWFOUNDLAND AND LABRADOR APRIL 12-14, 2018 Dr. Peter Hutten-Czapski HAILEYBURY ON RURAL CRITICAL CARE C-SPINE INJURY This session will review radiographic injury patterns of the cervical spine. 1. At the conclusion of this activity, participants will be able to appropriately order and interpret cervical spine X-rays. 2. Participants will learn to identify appropriate patients for imaging based on NEXUS and Canadian C-Spine rules. 3. Participants will be able to practice a systematic approach to interpret C-Spine films. Common pitfalls will be identified. 4. Participants will develop some comfort in identifying films with normal findings and some common injury patterns. 5. Participants will also identify films that they would not be comfortable with and might require further imaging and/or radiologist evaluation.



2 C-Spine X-ray Interpretation Karl Stobbe MD Beamsville, ON Peter Hutten-Czapski MD New Liskeard, ON Neil Leslie MD Revelstoke, BC Trina Larsen Soles MD Golden, BC C-spine x-ray interpretation When to x-ray Accuracy of x-ray What s normal Cases 1
3 Abnormal x-rays are uncommon 4% of patients have c-spine fracture without neurological deficit 1% have spinal cord injury How accurate are x-rays? Mower et al Ann Emerg Med 2001 n=34,069 3 views missed 0.1% of fractures Only missed 0.008% of unstable injuries 30% of missed injuries due to inadequate films 2
4 3
5 Patients excluded: Under 16 years old Unstable Acute paralysis Known vertebral disease: RA, spinal stenosis, etc. Injuries over 48 hrs old Minor injuries Pediatrics Epiphyses Fusion lines Pseudosubluxation Anterior wedging Predental space widening SCIWORA is more common Make interpretation difficult Canadian C-spine rules don t apply 4

6 What views to order Routine trauma series: Lat c-spine first proceed if normal A-P Odontoid view No data on obliques but some docs like them! Obliques can be helpful in seeing C7-T1 Flexion-extension views rarely or never show fracture when other views are normal In 30% of trauma cases, flex-ext is inadequate for diagnosis However, it is recommended ahead of MRI; can show ligamentous injury 5

 (1)")
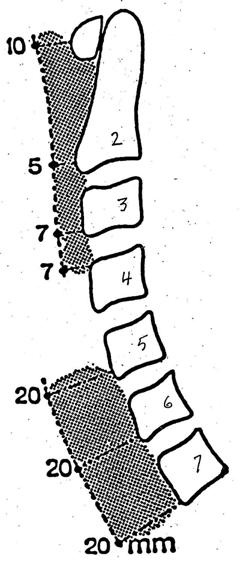
7 What Is Normal? A B C T1 (4) (1) (2) (3) 6

8 Atlantodens interval 7


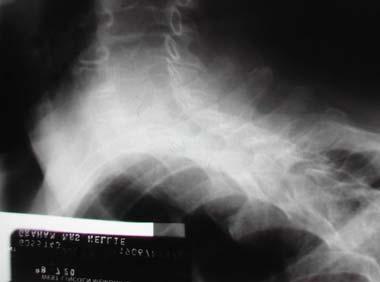
9 A-P view Unilateral facet dislocation 8



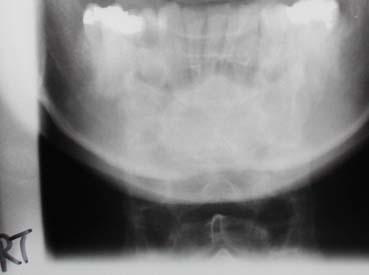
10 Open-mouth Odontoid view The standard C-spine trauma series 9
11 Patient 1 45 year old woman in a motor vehicle accident. She lost control of her car, slid into a ditch and rolled. Was brought to the hospital by ambulance with full c-spine immobilization. Vital signs stable, patient is alert but has no recall of the accident. She has facial lacerations, bruising on her shoulder and lower abdomen from the seat-belt, and abrasions on both her knees. She complains of neck pain. Chest exam shows good air entry bilaterally. Brief neurological exam is normal. 10




12 A-1-1 A1-2 11






13 A-1-3 A
14 After the x-ray No abnormality noted by ER physician. Facial lacerations were sutured, she was monitored overnight. X-ray reported as normal the next day by the radiologist. Patient sent home. Patient 2a 17 year old male, injured when a hay baler fell on his neck 13



15 A-2a-1 A-2a-2 14








16 A-2a-3 A-2a-4 15
17 The radiologist s report: C6 is subluxated anteriorly by 4mm with respect to C7. One small bone fragment measuring 1.2cm in length and 2mm in width is noted at the posterior aspect of the neural canal adjacent to the spinous process of C6 on the lateral view. This would suggest a fracture from a superior articular process of C7 but could also represent a fracture from an inferior articular facet of C6. On Oblique views there is asymmetry of the C6-7 intervertebral foramen on the right side and one small bone fragment is seen just above this which likely represents the previous described fragment. No other abnormality. Patient 3 24 year old female passenger on a motorcycle. Was wearing a helmet. Was thrown from the vehicle, landing on her head. 16



18 A-3-1 A


19 A-3-3 After the x-ray: Patient died in ER 18


20 Patient 4a 21 year old male, jumped from moving vehicle. Injured his head, briefly lost consciousness. Complaining of neck pain. A-4a 19
21 Radiologist s report: A complete study could not be done on this patient. Only A/P, odontoid view and a single crosstable projection showing the cervical spine to the level of C5 are available. There is seen to be a compression fracture of the body C4. This has resulted in anterior wedging of the body with loss of approximately 50 percent of its vertical body height. There appears to be at least one fracture line visible in the coronal plane. Other fracture sites cannot be excluded. There is a posterior extrusion of a portion of the body by approximately 3mm. The C3-4 interspace shows marked narrowing. The appearance of this suggests a hyperflexion injury. There does not appear to be any significant prevertebral edema. The cervical spine below C5 cannot be assessed on these films. Patient 5 17 year old male, was wrestling. Fell on the back of his head hyperflexion. Slept 4 hours woke with pain and stiffness in his neck. Was brought to hospital by his family. Examination was negative. 20



22 A-5-1 A




23 A-5-3 Radiologist s report: There is a flexion deformity of the cervical spine with loss of alignment at the C3 C4 level. The angulation at this point measures 15 degrees. This strongly suggests ligamentous injury, probably involving the posterior longitudinal ligament. 22


24 Patient 6 A 20 year-old female from a motorcycle accident. Complaining of neck pain. A




25 A-6-2 After the x-ray Transferred for surgery. Quadriplegic, but survived. 24


26 Patient 8 22 year-old male Hyperextension injury: stopped on highway, hit from behind by transport. Car demolished. A-8 25
27 Radiologist s report: There is a fracture-dislocation at the C2, C3 level with approximately 2 mm anterior displacement of C2 on C3. Patient 9 28 year old male complains of a sore neck the day after a fight in a bar. 26





28 A-9-1 A




29 A-9-3 Radiologist s report: There is a fracture through the spinous process of C7 with approximately 5mm posterior and caudad displacement of the fragment. Some mild degenerative arthritic changes can be seen at the intervertebral joints at C7-T1. The cervical spine appears otherwise unremarkable. Comment: Clay shovelers fracture spinous process C7. 28
30 C1-C2 anatomy Patient year old male. MVA hit another vehicle pulling onto the road. Multiple injuries. Required IV fluids, intubation. C-spine lateral was ordered along with chest and pelvic x-rays prior to detailed examination. 29


31 B-11 After the x-ray Odontoid fracture Type II with posterior displacement. Transferred for surgery which was successful. Long and stormy post-op course, eventual death from sepsis. 30


32 Odontoid fracture, type II Odontoid fracture, type II 31


33 Patient year old male; fall from a height. Bystanders thought his head bent forward. Patient has no recall of the fall. Complains of headache and neck pain. No neurological findings. Pain with neck movement. B




34 B-12-2 B
35 After the x-ray Patient complained of pain and tingling in his hands when flexion x-rays were done. Immobilized and transferred to referral centre. Surgical stabilization with good outcome. Rural MD was criticized for ordering too many x-rays when the abnormality was visible on the first 2 films. Patient year old woman injured in MVA at 50 kph. She was the front seat passenger, wearing seat belt. She has no recall of the accident, appears slightly confused but in no distress, though complains of neck pain. 34

36 Patient 12 X-ray tech: very difficult patient to do. Did my best. B




37 B-13-2 B




38 B-13-4 B




39 B-13-6 B
40 After the x-rays Frustrated with the poor quality films, the rural ER doc has a last look. On one lateral film, he wonders about the odontoid. Decides to immobilize the patient s c-spine and talk to the nearest surgical centre. With much reluctance the patient is accepted in transfer. Radiologist s report: The cervical spine is very difficult to image in this patient due to her inability to co-operate and fairly marked cervical kyphosis. There is seen to be a moderately severe degree of osteoporosis throughout the cervical spine. Moderately advanced degenerative arthritic change is present with interspaces at C5-6 and C6-7 slightly narrowed suggesting degenerative disc disease. On one lateral projection there is seen to be a deformity of the odontoid process of C2. This appears to be angulated ventrally by approximately 15 degrees and a step deformity can be seen in both its anterior and posterior margins measuring approximately 3mm. The overall appearance is strongly suggestive of a fracture of the odontoid process (type III). 39


41 Patient 13 A young man was involved in a MVA. He arrives by ambulance in full spinal immobilization to Revelstoke hospital. He has neck pain spasm and tenderness. Neurological examination is normal. A cross table Xray was taken at 62 80KV and 3 msec IX-1 40
42 Radiology Report Fracture Odontoid with posterior displacement. Also note incidental fracture C7- T1. Clayshoveler s Fracture. Atlantodens interval 41

43 Atlantodens interval Patient 14 A 7-year-old male was diving off a ledge when he landed head first in shallow water. He was pulled semiconscious from the water by lifeguards. While maintaining his airway, the lifeguards placed the patient in full C-spine immobilization. When the patient became more alert, he complained of pain to his upper neck region. Paramedics transported the patient to the ED. Upon arrival, the patient is awake, alert, cooperative, and in C-spine immobilization. His vital signs are normal, and the neurologic exam is nonfocal. He continues to complain of upper neck pain. A cross table lateral neck radiograph is obtained. 42

44 II-1 Not so unusual Quality II-2 43


45 But it is enough II-3 Repeat View II-4 44

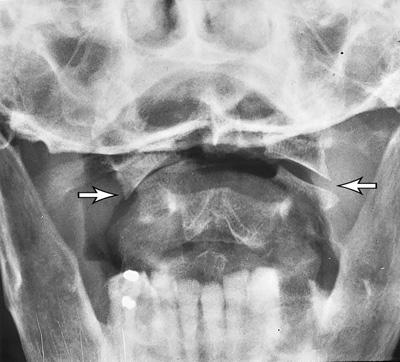
46 CT of our patient II-5 X-ray Report The lateral neck radiograph is suggestive of mild prevertebral soft tissue widening. Jefferson fracture (C1 ring) is demonstrated 45

47 Jefferson fracture Jefferson fracture 46


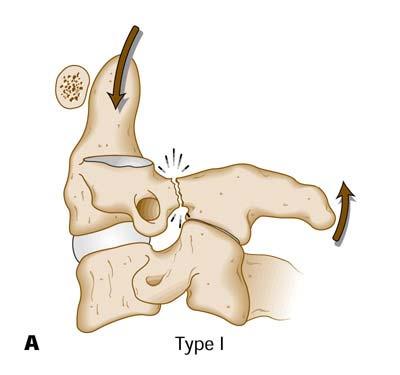
48 Jefferson fracture C-17 Atlantoaxial spondylolisthesis, type I 47
49 Atlantoaxial spondylolisthesis, type II Patient 15 A young male was involved in a MVA. He was dragged semi conscious up an embankment by his friend. A cross table Xray was done on arrival at the Revelstoke hospital. He has a lot of neck pain spasm and tenderness. Neurological examination is normal. 48



50 VII-1 After the X-ray Radiologist s first comment is Why are you taking post mortem Films? C2 Fracture/dislocation. Hangman type Neurosurgeon unable to reduce the dislocation so fused as is. 49

51 Hangman's fracture Atlantoaxial spondylolisthesis, type II 50


52 Patient year old male. C


53 C-18-2 Radiologist s comments Hyper Extension injury Hangman s fracture Seen best with slight flexion Posterior laminar line C2-C3 Step deformity 52


54 Patient 17 Elderly female brought to ER from MVA. Found at the scene. Car badly damaged. She was the driver. Car flipped. Was wearing seat belt. C-19 53
55 Radiologist s report: There is a slight step deformity with approximately 3mm anterior displacement of the body of C2 on C3. Films are not of good quality, however, there appears to be a defect through the pedicles of C2 with slight displacement of the anterior and posterior fragments. There is a marked degree of swelling of the prevertebral soft tissues at this level. Comment: These findings are suggestive of hyperextension or Hangman s fracture. Crosstable lateral view only is available which demonstrates the cervical spine only to be to the level of C4. The cervical spine appears, otherwise, unremarkable. Patient 18 A 7-year-old female is brought in by paramedics in full C-spine immobilization after being involved in a motor vehicle accident. According to her parents, the unrestrained child was sitting in her restrained mother's lap on the passenger side when the passenger side of the car was broadsided by another vehicle. The child's head was thrown into the dashboard, and she sustained severe injuries to the face and scalp. Upon arrival at the hospital, the patient is crying and responsive to all stimuli. There are multiple facial lacerations, a large scalp laceration, and facial edema/ecchymosis. 54
56 V-1 The hangman's fracture is an unstable fracture of the C2 pedicles, with forward displacement of C1 and the body of C2 on C3. V-2 55
57 Hangman's fracture Patient year old male, front-seat passenger. High-speed collision with parked vehicle in a residential neighbourhood. Driver has been airlifted to trauma centre. Patient is a happy drunk. Smiling, wandering around ER, uncooperative. Extremity bruises are his only obvious injuries. He has no complaints. Exam: midline tenderness over c-spine. 56




58 C-21-1 C




59 C-21-3 Patient 19 When told he has an unstable c-spine injury, the patient goes out for a smoke, refuses to believe diagnosis. Eventually he agrees to be immobilized and transferred. 58
60 Radiologist s comments: Unilateral Facet Dislocation C4-C5 Flexion rotation injury Patient year old tourist from Calgary on snow machine tour. Hits a bump, thrown off snow machine into the air and hits a tree about 15 feet off the ground. Slides down, c/o neck pain. Brought to ER on spine board with full spinal precautions. Some tingling in R hand. 59




61 60



62 61

63 Patient year old woman. Known history of osteoporosis. Fell in the bathroom and hit face on the sink. C/O neck pain. Drove self to hospital. Arrived in ER with a towel wrapped around her neck 62




64 63





65 64
")
66 A final word of caution SCIWORA Spinal Cord Injury WithOut Radiographic Abnormality (Treat the patient not the x-ray) 65
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Selective Spine Assessment & Spinal Motion Restriction
 Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
Selective Spine Assessment & Spinal Motion Restriction Supersedes: 02-09-15 Effective: 10-20-15 Spinal cord injury may be the result of direct blunt and/or penetrating trauma, compression forces (axial
1/15/2012. Cervical Spine Trauma. Who to Image. Who to Image. Who to Image. Who to Image. Trauma Cx Spine Protocols NEXUS. CCR and Nexus CCR CCR
 Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Selective Spinal Immobilization
 Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Selective Spinal Immobilization Objectives Understand the background of spinal immobilization. Understand the rationale for developing a current selective spinal immobilization protocol. Review the data
Overview. Overview. Chapter 30. Injuries to the Head and Spine 9/11/2012. Review of the Nervous and Skeletal Systems. Devices for Immobilization
 Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Chapter 30 Injuries to the Head and Spine Slide 1 Overview Review of the Nervous and Skeletal Systems The Nervous System The Skeletal System Devices for Immobilization Cervical Spine Short Backboards Long
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Radiology of Cervical Spine Trauma. Cervical Spine Trauma. Imaging Standards. Canadian C. Spine Rule 11/28/2016
 Radiology of Cervical Spine Trauma Dr. Steven J. Gould, D.C. Board Certified Chiropractic Radiologist Cleveland Chiropractic College, KC. MO. Radiology Residency at CCC, KC Cervical Spine Trauma Vertebral
Radiology of Cervical Spine Trauma Dr. Steven J. Gould, D.C. Board Certified Chiropractic Radiologist Cleveland Chiropractic College, KC. MO. Radiology Residency at CCC, KC Cervical Spine Trauma Vertebral
Chapter 32. Objectives. Objectives 01/09/2013. Spinal Column and Spinal Cord Trauma
 Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Chapter 32 Spinal Column and Spinal Cord Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1.
Spine and Spinal Cord Injury in Children
 Spine and Spinal Cord Injury in Children S. Danielle Brown, MS, RN, CNRN, SCRN Director, Research Coordination and Education Barrow Neurological Institute at Phoenix Children s Hospital Introduction Trauma
Spine and Spinal Cord Injury in Children S. Danielle Brown, MS, RN, CNRN, SCRN Director, Research Coordination and Education Barrow Neurological Institute at Phoenix Children s Hospital Introduction Trauma
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
Focused History and Physical Examination of the
 Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Henry: EMT Prehospital Care, Revised 3 rd Edition Lecture Notes Chapter 10: Focused History and Physical Examination of Trauma Patients Chapter 10 Focused History and Physical Examination of the Trauma
Indications for cervical spine immobilisation: -
 Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Paediatric Trauma Cervical Spine Guidelines UHW Traumatic injuries of the cervical spine (C-spine) are uncommon in children. However, it is safer assume there is a cervical spine injury until examination
Patient Assessment. Chapter 8
 Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
Patient Assessment Chapter 8 Patient Assessment Scene size-up Initial assessment Focused history and physical exam Vital signs History Detailed physical exam Ongoing assessment Patient Assessment Process
MDCT and MRI evaluation of cervical spine trauma
 Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Spinal Trauma. Dr T G Kruger
 Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Introduction. Objectives C-Spine: Where Are We Now? NAEMSP Medical Director Course 1/9/2013
 NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
NAEMSP Medical Director Course 1/9/2013 Objectives C-Spine: Where Are We Now? Robert M. Domeier, MD EMS Medical Director Washtenaw/Livingston Medical Control Authority Department of Emergency Medicine
Spine Trauma- Part B
 Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
Spine Trauma- Part B Cervical Spine Injuries Atlanto- Occipital Dislocation Hyperextension and distraction mechanism Down s syndrome, RA more susceptible Asymmetric lateral masses on odontoid view Widened
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES
 REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
Spinal injury. Structure of the spine
 Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
Spinal injury Structure of the spine Some understanding of the structure of the spine (spinal column) and the spinal cord is important as it helps your Neurosurgeon explain about the part of the spine
PREPARED FOR. Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016. REFERRING DOCTOR : Dr.
 Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing
 1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
1 2 3 4 5 6 Chapter 8 Trauma Patient Assessment The Patient Assessment Process The Primary Assessment ABCDE s Airway, Breathing, Circulation while securing D-Disability Chief complaint and/or Mechanism
The Dynamics of Trauma. Jamie Syrett, MD Director of Prehospital Care Rochester General Health System
 The Dynamics of Trauma Jamie Syrett, MD Director of Prehospital Care Rochester General Health System Me Boarded EM physician Fellowship trained in EMS Volunteer EMT-B,D,P,L5...etc etc etc Today - Commitment
The Dynamics of Trauma Jamie Syrett, MD Director of Prehospital Care Rochester General Health System Me Boarded EM physician Fellowship trained in EMS Volunteer EMT-B,D,P,L5...etc etc etc Today - Commitment
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Shenandoah Co. Fire & Rescue. Injuries to. and Spine. December EMS Training Bill Streett Training Section Chief
 Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Shenandoah Co. Fire & Rescue Injuries to the Head and Spine December EMS Training Bill Streett Training Section Chief C.E. Card Information BLS Providers 2 Cards / Provider Category 1 Course # Blank Topic#
Pediatric Trauma Cases
 Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
Pediatric Trauma Cases QPEM 2018 Barbara Blackie, MD, MEd, FRCPC DISCLOSURE I do not have any relevant financial relationship with commercial interest to disclose. Learning Objectives -Manage interactive
LESSON ASSIGNMENT. Positioning for Exams of the Spine. After completing this lesson, you should be able to identify:
 LESSON ASSIGNMENT LESSON 4 Positioning for Exams of the Spine. LESSON ASSIGNMENT Paragraphs 4-1 through 4-15. LESSON OBJECTIVES After completing this lesson, you should be able to identify: 4-1. Identify
LESSON ASSIGNMENT LESSON 4 Positioning for Exams of the Spine. LESSON ASSIGNMENT Paragraphs 4-1 through 4-15. LESSON OBJECTIVES After completing this lesson, you should be able to identify: 4-1. Identify
of Trauma Assembly 27 th Page 1
 Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
Eastern Association for the Surgery of Trauma 27 th Annual Scientific Assembly Sunrise Session 08 To Scan or Not To Scan Thatt is the Question January 16, 2014 Waldorf Astoria Naples Naples, Floridaa Page
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW
 INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
Evaluation and Stabilization of the Athlete with Possible Spine Injury
 Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Evaluation and Stabilization of the Athlete with Possible Spine Injury Jeffrey H. Bohmer, MD, FACEP Emergency Physician Northwestern Medicine Central DuPage Hospital June 12, 2015 Introduction Goals: 1.
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
The vault bones Frontal Parietals Occiput Temporals Sphenoid Ethmoid
 The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
Anterior Cervical Subluxation: An Unstable Position
 275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
XXX Spinal Motion Restriction
 Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
Nor-Cal EMS Policy & Procedure Manual NAME OF MODULE XXX Purpose: The purpose of this protocol is to protect patients with signs and symptoms of spinal injuries and those who have the potential for spinal
SpineFAQs. Neck Pain Diagnosis and Treatment
 SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
SpineFAQs Neck Pain Diagnosis and Treatment Neck pain is a common reason people visit their doctor. Neck pain typically doesn't start from a single injury. Instead, the problem usually develops over time
3/14/2014 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION THE PROBLEM OLD THINKING
 USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
USED TO BE SIMPLE.. TO IMMOBILIZE OR NOT TO IMMOBILIZE.THAT IS THE QUESTION Immobilization following injury used to be a simple decision--but no one was thinking. Up to 5 million people per year receive
Trauma Overview. Chapter 22
 Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
Trauma Overview Chapter 22 Kinematics of Trauma Injuries are the leading cause of death among children and young adults. Kinematics introduces the basic physical concepts that dictate how injuries occur
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Injuries to the Head and Spine
 Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
Injuries to the Head and Spine Anatomy Review Skull Protects the brain Made up of several bones with seam like sutures Regions of the scalp-frontal, occipital, parietal, temporal Bones of face Orbits Mandible
2. The vertebral arch is composed of pedicles (projecting from the body) and laminae (uniting arch posteriorly).
 and laminae (uniting arch posteriorly).") VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
SPINAL IMMOBILIZATION
 Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
Spinal Immobilization Decision Assessment Recent studies have shown an increase in mortality for patients with isolated penetrating trauma who are spinally immobilized. Therefore spinal immobilization
SpineFAQs. Lumbar Spondylolisthesis
 SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
SpineFAQs Lumbar Spondylolisthesis Normally, the bones of the spine (the vertebrae) stand neatly stacked on top of one another. The ligaments and joints support the spine. Spondylolisthesis alters the
Traumatic Spinal Cord Injury. 39 th CANP Annual Educational Conference March 18 th, :00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc
 Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Traumatic Spinal Cord Injury 39 th CANP Annual Educational Conference March 18 th, 2016 5:00pm-6:15pm Carl Wherry, ACNP-bc Amanda Severson, ACNP-bc Disclosures No conflicts of interest to disclose. Introduction
Chance Fracture Joseph Junewick, MD FACR
 Chance Fracture Joseph Junewick, MD FACR 08/02/2010 History Restrained teenager involved in motor vehicle accident. Diagnosis Chance Fracture (Hyperflexion-Distraction Injury) Discussion Chance-type spinal
Chance Fracture Joseph Junewick, MD FACR 08/02/2010 History Restrained teenager involved in motor vehicle accident. Diagnosis Chance Fracture (Hyperflexion-Distraction Injury) Discussion Chance-type spinal
The Spine.
 The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
The Spine www.fisiokinesiterapia.biz Characteristics of Vertebrae Cervical Spine 1 and 2 Sacrum and Coccyx Curves Lordotic in the Spine Kyphotic Lordotic Ligamentous Support Muscles of the Spine Spinal
The Positive Findings In Neck Injuries. American Journal of Orthopedics. August-September, 1964, pp
 The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
The Positive Findings In Neck Injuries 1 American Journal of Orthopedics August-September, 1964, pp. 178-187 Ruth Jackson, MD This author analyzed 5,000 patients with disorders and found the following:
VERTEBRAL COLUMN VERTEBRAL COLUMN
 VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
TALK TRAUMA Clearing the C-Spine. David Ouellette
 TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
TALK TRAUMA 2011 Clearing the C-Spine David Ouellette Case #1 - Mother / Daughter MVC 34 y/o female Dangerous mechanism CHI Mumbling incoherently Femur # - distracting injury ETOH - 22 9 y/o female Dangerous
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries
 A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
A Pictorial Review of the Biomechanics and Imaging Findings in Cervical Spine Injuries Award: Certificate of Merit Poster No.: C-1741 Congress: ECR 2011 Type: Educational Exhibit Authors: A. Adams, A.
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
Cervical Spine Precautions A quick review. By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine
 Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
Cervical Spine Precautions A quick review By Joseph Lewis, M.D. Medical Director, Honolulu EMS Board Certified in Emergency Medicine 1 Goals of this Cervical Spine Immobilization In-service Learn Objectives:
MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question.
 EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
EPC Ch 24 Quiz w-key Name MULTIPLE CHOICE. Choose the one alternative that best completes the statement or answers the question. 1) Which of the following best explains the presentation and prognosis of
The craniocervical junction
 Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS AND PAIN
 Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury?
 Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury? 1 Patient Safety in Surgery March 8, 2009 Martin Elbel, Michael Kramer,
Deceleration during 'real life' motor vehicle collisions: A sensitive predictor for the risk of sustaining a cervical spine injury? 1 Patient Safety in Surgery March 8, 2009 Martin Elbel, Michael Kramer,
Thoracolumbar Spine Fractures
 Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
10O SPLINTING OF INJURIES ADULT & PEDIATRIC. 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric:
 10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
10O SPLINTING OF INJURIES ADULT & PEDIATRIC EMERGENCY MEDICAL RESPONDER EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC 10Oa: Axial/Spine with Selective Spinal Motion Restriction Adult & Pediatric: Many
Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE
 READ ONLINE") Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE If you are searching for a ebook Management of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) in pdf
Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE If you are searching for a ebook Management of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) in pdf
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Physical and Radiographic Examination of the Spine
 Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
Physical and Radiographic Examination of the Spine Christopher M. Bono, MD Assistant Professor, Department of Orthopaedic Surgery Boston University School of Medicine, Boston Medical Center, Boston, MA
CERVICAL STRAIN AND SPRAIN
 CERVICAL STRAIN AND SPRAIN Description Cervical strain/sprain is an injury to the neck caused when it is forcefully whipped or forced backward or forward. The structures involved are the muscles, ligaments,
CERVICAL STRAIN AND SPRAIN Description Cervical strain/sprain is an injury to the neck caused when it is forcefully whipped or forced backward or forward. The structures involved are the muscles, ligaments,
CERVICAL STRAIN AND SPRAIN (Whiplash)
") CERVICAL STRAIN AND SPRAIN (Whiplash) Description time and using proper technique decrease the frequency of Whiplash is an injury to the neck caused when it is forcefully whipped or forced backward or
CERVICAL STRAIN AND SPRAIN (Whiplash) Description time and using proper technique decrease the frequency of Whiplash is an injury to the neck caused when it is forcefully whipped or forced backward or
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #2 Blunt Trauma Blunt trauma is the most common cause of traumatic death and disability. The definition
Patient Information MIS LLIF. Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine...2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine...2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Date of Admission: [DATE]. Date of Discharge:
![Date of Admission: [DATE]. Date of Discharge:](/thumbs/74/71277118.jpg "Date of Admission: [DATE]. Date of Discharge:") Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Date of Admission: [DATE]. Date of Discharge: History of Present Illness: Mr. [NAME] AKA [NAME] is a 31-year-old male who presents to the [PLACE] Trauma Surgery Service as a moderate trauma on [DATE] following
Assessment of the Trauma Patient
 CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
CHAPTER 10 Assessment of the Trauma Patient Overall Assessment Scheme Scene Size-Up Initial Assessment Trauma Physical Exam Vital Signs & SAMPLE History Medical SAMPLE History Physical Exam & Vital Signs
Bottom of stairway. Respond to a fall victim at. Books and papers scattered on the ground Initial Assessment: Scene Survey
 Trauma Objective/Teaching Points: MOI: Twisted Ankle Very first scenario Establish the need to use common sense Establishing rapport with patient (Communication) Bottom of stairway Respond to a fall victim
Trauma Objective/Teaching Points: MOI: Twisted Ankle Very first scenario Establish the need to use common sense Establishing rapport with patient (Communication) Bottom of stairway Respond to a fall victim
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition
 Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
Injuries to the Head and Spine From Bradys Emergency Care 10 th Edition 1. When performing the four-rescuer log roll, which responder pulls the board into position? A.) Head B.) Waist C.) Knee D.) Shoulder
3/3/2017. Acute spine disorder (< 4weeks duration) Subacute spine disorder (4-12 weeks duration) Chronic spine disorder (>12 weeks duration)
 Subacute spine disorder (4-12 weeks duration) Chronic spine disorder (>12 weeks duration)") William Hsu BSc DC DACBR March 4, 2017 Acute spine disorder (< 4weeks duration) Subacute spine disorder (4-12 weeks duration) Chronic spine disorder (>12 weeks duration) Neurologic symptoms and signs pain
William Hsu BSc DC DACBR March 4, 2017 Acute spine disorder (< 4weeks duration) Subacute spine disorder (4-12 weeks duration) Chronic spine disorder (>12 weeks duration) Neurologic symptoms and signs pain
OMT for the ACOFP Boards: A Review of Clinical and Basic Information
 OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
OMT for the ACOFP Boards: A Review of Clinical and Basic Information Kevin D. Treffer, D.O., FACOFP Associate Professor, Department of OMM and Primary Care Interim Chair, Department of OMM Kansas City
Cervical Spine Trauma 2016 Nordic Trauma Society
 Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
Cervical Spine Trauma 2016 Nordic Trauma Society Stuart E. Mirvis. M.D., FACR Department of Radiology and Maryland Shock-Trauma Center University of Maryland School of Medicine Topics to Review Definition
Cervical Spine Injuries in the Athlete: The pain in the neck. BrianBraaksma, MD Orthopedic Spine Surgeon
 Cervical Spine Injuries in the Athlete: The pain in the neck BrianBraaksma, MD Orthop Surgeon Outline Incidence Pathophysiology Diving injuries Football Sprain Stingers and burners Transient Quad Fractures
Cervical Spine Injuries in the Athlete: The pain in the neck BrianBraaksma, MD Orthop Surgeon Outline Incidence Pathophysiology Diving injuries Football Sprain Stingers and burners Transient Quad Fractures
Purely Ligamentous Flexion-Distraction Injury in a Five-Year-Old Child Treated with Surgical Management
 Open Access Case Report DOI: 10.7759/cureus.1130 Purely Ligamentous Flexion-Distraction Injury in a Five-Year-Old Child Treated with Surgical Management Ryan M. Schiedo 1, William Lavelle 2, Nathaniel
Open Access Case Report DOI: 10.7759/cureus.1130 Purely Ligamentous Flexion-Distraction Injury in a Five-Year-Old Child Treated with Surgical Management Ryan M. Schiedo 1, William Lavelle 2, Nathaniel
Chapter 20: The Spine The McGraw-Hill Companies, Inc. All rights reserved.
 Chapter 20: The Spine Anatomy of the Spine Prevention of Injuries to the Spine Cervical Spine Muscle Strengthening Muscles of the neck resist hyperflexion, hyperextension and rotational forces Prior
Chapter 20: The Spine Anatomy of the Spine Prevention of Injuries to the Spine Cervical Spine Muscle Strengthening Muscles of the neck resist hyperflexion, hyperextension and rotational forces Prior
EMS Spinal Assessment and Precautions
 EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
EMS Spinal Assessment and Precautions Adapted from a presentation prepared by Chelsea C. White IV, MD, NREMT-P Medical Director, Bernalillo County Fire Department Robert M. Domeier, MD, EMS Medical Director,
Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men years old
 Annually 15,000 permanent spinal cord injuries Commonly men years old") 1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
1 2 3 4 5 6 7 Chapter 24 Spinal Trauma Introduction to Spinal Injuries (1 of 2) Annually 15,000 permanent spinal cord injuries Commonly men 16-30 years old Mechanism of Injury: Vehicle crashes: 48% : 21%
8/4/2012. Causes and Cures. Nucleus pulposus. Annulus fibrosis. Vertebral end plate % water. Deforms under pressure
 Causes and Cures Intervertebral discs Facet (zygopophyseal) joints Inter body joints Spinal nerve roots Nerve compression Pathological conditions Video Causes of back pain Nucleus pulposus Annulus fibrosis
Causes and Cures Intervertebral discs Facet (zygopophyseal) joints Inter body joints Spinal nerve roots Nerve compression Pathological conditions Video Causes of back pain Nucleus pulposus Annulus fibrosis
Digital Motion X-ray Cervical Spine
 NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the
NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES
 AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
AO CLASSIFICATIONS THORACO-LUMBAR SPINAL INJURIES T H E A O / A S I F ( A R B E I T S G E M E I N S C H A F T F Ü R O S T E O S Y N T H E S E F R A G E N / A S S O C I A T I O N F O R T H E S T U D Y O
DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT
 P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
Kinetic Energy Energy in Motion KE = Mass (weight) X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT
 X Velocity (speed)² 2 Double Weight = Energy Double Speed = Energy IS THE GREATEST DETERMINANT") 1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
1 Chapter 17 Blunt Trauma 2 Introduction to Blunt Trauma Most common cause of trauma death and disability exchange between an object and the human body, without intrusion through the skin 3 Blunt trauma
Patient Information MIS LLIF. Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques
 Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine....2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Patient Information MIS LLIF Lateral Lumbar Interbody Fusion Using Minimally Invasive Surgical Techniques Table of Contents Anatomy of Spine....2 General Conditions of the Spine....4 What is Spondylolisthesis....5
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018
 Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Gillian Wooldridge, DO Houston Methodist Willowbrook Hospital Primary Care Sports Medicine Fellowship May 3, 2018 Disclosures Neither I nor any family members have financial disclosures Special thanks
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Cervical and Thoracic Spinal Conditions Chapter 11
 Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Cervical and Thoracic Spinal Conditions Chapter 11 Anatomy Spinal column Vertebrae Cervical (7) convex anteriorly Thoracic (12) concave anteriorly Lumbar (5) convex anteriorly Sacral (5 fused) concave
Spinal Trauma at the Pediatric Age
 Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns
Spinal Trauma at the Pediatric Age Burçak B LG NER Nejat AKALAN ABSTRACT Spinal trauma is relatively rare in pediatric patients. The anatomy and biomechanics of the growing spine produce failure patterns