Clinical Cases of Endocrine Hypertension
|
|
|
- Colleen Thompson
- 5 years ago
- Views:
Transcription
1 Clinical Cases of Endocrine Hypertension Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan
2 Disclosures Contracted Research Novartis Pharmaceuticals Strongbridge Biopharma Millendo Pharmaceuticals Neurocrine Biosciences Consultant Quest Diagnostics Corcept Therapeutics Janssen Pharmaceuticals Novartis Pharmaceuticals Strongbridge Biopharma Millendo Pharmaceuticals Diurnal LTD Spruce Biosciences
3 Endocrine HTN Case 1 52 YO WM Difficult-to-control HTN for 25 Years Amlodipine, Benazepril, Carvedilol, HCTZ, KCl Question: What is your Differential Diagnosis for Resistant Hypertension?
4 Resistant HTN Differential Dx Medication Nonadherence Ethanol Consumption Sleep Apnea Renal Insufficiency Mineralocorticoid Excess
5 Endocrine HTN Case 1 Preoperative Knee Surgery K = 1.9 meq/l Nephrology Evaluation Renal Artery Doppler Sono Normal High Urine K & Aldosterone, Normal PRA MRI Showed Possible 1 cm Nodule L Adrenal Spironolactone 100 mg QD Added BP & K Much Better Referred to Surgeon; Requested Endo Consult
6 Endocrine HTN Case 1 PRA 2.4 ng/ml/hr; Potassium 4.7 meq/l; Serum Aldosterone 74.5 ng/dl 24 h Urine: Epinephrine 40 mcg, Norepinephrine 286 mcg, Dopamine 697 mcg, Aldosterone 149 mcg, Potassium 80 meq, Creatinine 4.1 g Questions: What is the likelihood that this man has Primary Aldosteronism? Would you order any tests now?
7 Pearl #1: Screening is about whether renin is suppressed, not whether aldosterone is high
8 Primary Aldosteronism Whom To Screen? HTN + Hypokalemia Patients With Resistant HTN Or Controlled With 4 Drugs Patients With HTN At Age < 40 Or FH HTN or CVA Age <40 Considering Secondary Causes Sustained BP >150/100 HTN + Known Adrenal Mass or OSA HTN + First-Degree Relative With PA
9 ARR Sensitivity & Specificity Nishizaka 2005 Am J Hypertens 18:805
10 Who Has Primary Aldo? ARR Interpretation Serum Aldo PRA Potassium (ng/dl) (ng/ml/hr) ARR (meq/l) Interpretation Low ARR, not PA, stop Low aldo, not PA, stop Positive screen for PA, go to confirmatory testing Probably PA, supplement K, rescreen Probably PA, stop meds and rescreen
11 Funder et al 2016 JCEM 101:1889
12 Endocrine HTN Case 1 Labs Obtained: PRA 1.5 ng/ml/hr; Serum Aldosterone 55 ng/dl, Potassium 4.0 meq/l Spironolactone Discontinued, KCl Increased to 40 meq/d; 24 h Urine Collected 2 Weeks Later: 24 h urine: Aldosterone 41 mcg, Sodium 246 meq, Potassium 54 meq PRA <0.6 ng/ml/hr; Serum Aldosterone 29 ng/dl, Potassium 3.8 meq/l BUT--Unable to Do AVS For Several Weeks
13 Endocrine HTN Case 1 Potassium 3.2 meq/l; Amiloride 5 mg/d Added 3 Weeks Later/1 Week pre-avs: Potassium 3.9 meq/l, PRA 0.64 ng/ml/hr; Amiloride Stopped 3 Days Prior to AVS (Potassium 2.9 meq/l!)
14 Endocrine HTN Case 1 L ADX Remains on Amlodipine Monotherapy BP /80-85; Potassium 4.8 meq/l Everybody is Happy News: AVS With Spironolactone is OK!
15 Endocrine HTN Case 2 56 YO WM Referred for Evaluation of PA HTN, Low K, Elevated ARR PRA <0.15 ng/ml/hr; Potassium 3.1 meq/l; Serum Aldosterone 15.6 ng/dl CT: R Adrenal Mass of 1.2 cm AVS Outside: Localized to the Left Rx Spironolactone but Severe Gynecomastia Cannot Afford Eplerenone Chronically What Did the AVS Really Show?? What Would You Do Now??



16 Endocrine HTN Case 2: CT Scan
17 Pearl #2: Imaging is not about whether an adenoma is present on one adrenal gland, it is about whether the other adrenal gland is unequivocally normal


18 Adrenal Vein Sampling Right Adrenal Venogram
19 AVS Interpretation Mixed Venous Cortisol & Aldosterone RAV, LAV Cortisol = Selectivity Index (SI) >2x IVC -Cosyntropin; >4x IVC +Cosyntropin A/C Gradients = Lateralization Index (LI) >2 -Cosyntropin; >4 +Cosyntropin Low Side < IVC = Contralateral Suppression Two Common Patterns (+Cosyntropin): High AV Low AV IVC Interpretation Lateralized Bilateral
20 Endocrine HTN Case 2 PRA <0.6 ng/ml/hr; Potassium 3.4 meq/l; Serum Aldosterone 42 ng/dl Switched to Amiloride 5 mg/d AVS Lateralized to R R ADX K Normal, BP Much Better
21 Primary Aldosteronism Teaching Points Cases 1 & 2 Interpreting ARR on Medications Confirmatory Testing Managing Hypokalemia During Workup Healthy Skepticism for Reports of CT, MRI, and AVS In God We Trust, All Others Show Us the Data
22 Primary Aldosteronism AVS Example 42 yo HM, HTN x 5 yr BP 155/95; 3 Drugs; Many Side Effects 24 h Urine K 106, Na 385, Aldo 217 PRA 1, PAC 47, K 4.7, 18OHB 45 CT: L 1.5 cm; 5 mm R

23 AVS Example A 26,160 C 922 A/C 28.4 IVC: A 39 C 19.3 A/C 2.02 A 2,131 C 1,264 A/C 1.79
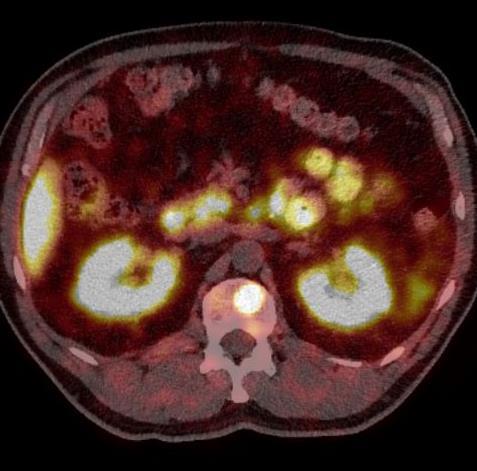
24 Endocrine HTN Case 3 36 YO Vietnamese F Recurrent Pregnancy Losses Resistant HTN, Hypokalemia Labetolol, Amlodipine, KCl PRA 1 ng/ml/h; Aldo 21 ng/dl, K h U Aldo 17 mg Na 155 meq, K 197 meq CT: 3 cm R Adrenal Mass, L Poorly Seen

25 Endocrine HTN Case 3: CT Scan
26 Endocrine HTN Case 3: AVS Site Aldo Cortisol Ratio RAV LAV IVC PV What s Going On???
27 Endocrine HTN Case 3 Endo Referral ROS: Bruising, 10 lb Wt Gain, Depression Exam: Wt 103 lbs, BMI 24 kg/m 2, +Bruises, SC Fat Pads 24h UFC 260 mg ACTH <5 pg/ml DHEA-S 18 mg/dl AM Cortisol After 1 mg Dex 22.5 mg/dl

28 Endocrine HTN Case 4 42 YO WF Sudden Onset HTN, Hirsutism PRA <0.4 ng/ml/h; Aldosterone 5 ng/dl, DST Cortsol 1 μg/dl, K 2.8 meq/l, T 125 ng/dl Spironolactone 300 mg/d Normalized BP & K
29 Mineralocorticoid HTN Differential Diagnosis Primary Hyperaldosteronism APA, IHA, FHAs Secondary Aldosteronism Cortisol Cushing Syndrome AME: 11bHSD2, Licorice 11-DOC Tumor, Drugs, 17OHD, 11OHD Liddle Syndrome
30 What the...??? 3-yo girl: Growth retardation, hypertension (180/140 mmhg), Hypokalemia (2.7 mmol/l), hyporeninemic hypoaldosteronism Dexamethasone ACTH Spironolactone BD 160/100 Serum K 2.8 Urin Na 150 PRA <0.3 Urin Aldo < / <0.3 < / < / <0.3 < / Dx: AME Ulick et al 1979 JCEM 49:757
31 Protecting MR from Glucocorticoids HO CH 2 OH O HC C=O MR O CH 2 OH CH 2 OH O HO C=O OH 11ßHSD2 X O O C=O OH Licorice DHF 5aDHF DHE THF 5aTHF THE THF+5aTHF = THE Ferrari 2000 Kidney Int 57:1374
32 Endocrine HTN Case 5 35 YO WF, Ovaries/Uterus Did Not Develop I think I have Androgen Insensitivity PMH: HTN, Inguinal Hernia Repair Meds: Metoprolol, Irbesartan, Amlodipine Hydralazine, KCl + Premarin BP 130/86 HR 73, Not Obese, 2/6 SEM No Cushingoid Stigmata Breasts Tanner V, Sparse Body Hair K 3.0, MR-Angio: Nl Renal Arteries, But.


33 CT Adrenals
34 Case 5: ACTH Stimulation Test Hormone (ng/dl) Baseline Post-ACTH Normal ACTH (pg/ml) 31 <25 Direct Renin (mu/ml) < DHEA-sulfate (mg/dl) < Cortisol (mg/dl) >20 Aldosterone 4 6 doubles Corticosterone 14,544 21,981 <1, Deoxycorticosterone Dx: 17-Hydroxylase Deficiency
35 ACTH 17OHD: Pathophysiology Cholesterol Aldosterone Renin StAR CYP11A1 3bHSD Pregnenolone Progesterone CYP11B2 Blood Pressure Blood Volume CYP21A2 CYP17A1 CYP17A1 DOC CYP11B1 B CYP17A1 17OH-Preg 3bHSD CYP17A1 17OH-Prog CYP21A2 CYP11B1 Cortisol DHEA Androgens & Estrogens
36 Pituitary 11OHD Cholesterol ACTH CYP11A1 Salt & Water Retention Kidney Renin/ATII CYP17A1 Pregnenolone 3bHSD CYP17A1 Progesterone CYP21A2 DOC CYP11B2 CYP11B1 Aldosterone Corticosterone 3bHSD 17OH-Pregnenolone CYP11B1 17OH-Progesterone 11-Deoxycortisol Cortisol CYP21A2 CYP17A1 (b 5 ) DHEA 3bHSD CYP17A1 (b 5 ) Androstenedione CYP19A1 Estrone 17bHSD1 17bHSD2 17bHSD3 17bHSD2 17bHSD1 17bHSD2 Androstenediol CYP19A1 3bHSD Testosterone Estradiol 5a-Reductases Dihydrotestosterone
37 DOC Excess & AME in 2018 Abiraterone Acetate CYP17A1 Inhibitor for CRPC Co-Administer Prednis(ol)one 5 mg BID Osilodrostat (LCI-699) CYP11B1/11B2 Inhibitor ( New Metyrapone ) In Phase III Trials For Cushing Disease Licorice Good & Plenty Contains Some Real Licorice Chewing Tobacco + Licorice Nutritional Supplements
38 Management ACTH-Dependent MC HTN MR Antagonists Titrate to Normal Renin Glucocorticoids Sparingly Cushingoid Side Effects Dex > Pred > HC Amiloride, Triamterine for K; CCB for BP AME: MRA + Hydrocortisone 17OHD: Spironolactone + Estrogen + HC 11OHD: HC + Eplerenone (M) or Spiro (F)
39 Endocrine HTN Summary: Mineralocorticoids Know Who to Screen and When to Stop Must Confirm Non-suppressible Aldo Do Not Be Duped by CT Scans AVS for Most PA Cases Prior to Surgery Genetics of Mineralocorticoid Excess Do Not Forget Other Mineralocorticoids Spironolactone, Eplerenone Medical Rx
40 Endocrine HTN Case 6 53 YO WM, Uncontrolled HTN Morbidly Obese, IGT, +Cigs +EtOH Fatigue, Snoring, Medication AE s Amlodipine, Losartan-HCT, Clonidine BP 148/96 HR 88, Spikes to 190/110 K 4.0 meq/l, Cr 1.8 mg/dl, malb 110 mg/g PRA <0.4 ng/ml/h; Aldosterone 6 ng/dl Plasma NMN 1.3, MN <0.2 nmol/l
41 Pearl #3: Pheo Symptoms Correlate With Catecholamine Elevations
42 Endocrine HTN Case 7 40 YO LAM With Abd Pain, Dyspnea ECG: HR 156, ST-Depression Echo: LVEF 20%, Normal Filling & Valves Cath: Global Hypokinesis, Normal Cors, BP <70 TFTs Normal, LFTs Slight High, BNP 488 pg/ml CXR: Cardiomegaly, Bibasilar Infiltrates

43 Endocrine HTN Case 7
44 Pearl #4: Pheos Do Not Hide on CT Scans
45 Pheochromocytoma Differential Diagnosis Of Spells + HTN &/Or Tachycardia Flushing, No HTN Labile Essential HTN Sleep Apnea Clonidine Withdrawal Neuroblastoma Arrhythmia Thyrotoxicosis Panic Attacks Hypoglycemia Drugs Menopause Mastocytosis Carcinoid Medullary Thy CA Diencephalic Sz Diabetes/Autonomic Drugs (Panic Attacks)
46 Pheochromocytoma Clinical Features Pressure: Sustained HTN + Spikes Pain: Throbbing HA, Chest Pain Perspiration: Heavy, Generalized Palpitations Pallor Other: Hyperglycemia, Weight Loss, Tremor, Orthostasis, Hypercalcemia, Fatty Liver, Cardiomyopathy 5-10% Asymptomatic(!!)
47 Pheochromocytoma The Pheo Paroxysm ( Spell ) Throbbing HA & Chest Pain Drenching Sweat Pounding Tachycardia Extreme BP Elevation Pallor, All Lasting Min NO Flush, Wheezing, Itching, Diarrhea, Syncope, Dermatographia DDx: Menopause & Clonidine Withdrawal
48 Catecholamine Biosyntheis HO CO 2 H TOH HO CO 2 H Tyrosine NH 2 HO NH 2 L-DOPA OH DDC HO NH 2 DBH HO NH 2 HO Dopamine HO Norepinephrine PMNT HO OH NHCH 3 HO Epinephrine
49 HO Catecholamine Catabolism OH OH NH HO 2 NHCH 3 HO HO Norepinephrine OH NH 2 COMT HO HO Epinephrine OH NHCH 3 CH 3 O Normetanephrine Dopamine COMT HO Methoxytyramine MAO CH 3 O Homovanillic Acid (HVA) MAO CH Metanephrine 3 O OH CO 2 H Vanillylmandelic Acid (VMA)
50 --500 pg/ml Plasma Catecholamines & Metanephrines After 0.3 mg Clonidine --1 nmol/l Eisenhofer et al 2003 JCEM 88:2656
51 Pheochromocytoma Associated Diseases & Genes Most Autosomal Dominant MEN2A: MTC, Pheo, HPTH, RET MEN2B: MTC, Pheo, Neuromas, RET VHL: Angiomas, Renal Cell CA, VHL Isolated Familial Pheo Is VHL Type 2C NF-1: Café au Lait, Neurofibromas, NF1 Paragangliomas: SDHx = A, B, C, D, AF2 Phakomatoses: Tuberous Sclerosis, Ataxia- Telangectasia, Sturge-Weber Other Genes: TMEM127, MAX, HRAS, HIF2A, PHD1, PHD2, FH, ATRX, MDH2
52 Endocrine HTN Case 8 58 YO WM, Single Episode Hematuria No Paroxysms, Nl BP US: R Adrenal Mass 24 h Urine MN 233 mcg, NMN 2504 mcg MRI: 3.4 cm R adrenal mass High, Heterogeneous Signal T2-weighted No Signal Drop-out on Out-of-phase T1 Plasma MN 0.45, NMN 7.65

53 Endocrine HTN Case 7

54 Pheochromocytoma MIBG

55 Metastatic PGL [ 68 Ga]DOTATATE
56 Summary: Pheo/PGL Plasma & Urine Metanephrines Both OK Most Slightly Positive Screens Not Pheo Sleep Apnea, Clonidine Withdrawal Reversible a-blockers If Mild Disease Blockade Prior to CT Scans Not Needed Think Familial If Young, Weird Tumor(s) Think VHL In Isolated Familial Pheo Think SDHx for Paragangliomas
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Primary Aldosteronism & Implications for Primary Hypertension
 & Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
& Implications for Primary Hypertension Richard J. Auchus, MD, PhD, FACE Professor and Fellowship Program Director Depts of Internal Medicine/MEND & Pharmacology University of Michigan Disclosures Contracted
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Transitions For the CAH Patient
 Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Adrenal Disorders. Disclosure: I do not have any conflicts of interest
 Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
Adrenal Disorders Robert G. Dluhy, M.D. Disclosure: I do not have any conflicts of interest Robert G. Dluhy, MD Case 1 28 y.o. male with no significant past medical history presents with 6-8 months of
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Differential Diagnosis of Cushing s Syndrome
 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University
The most current assessment of this problem can be found in the Apex note dated
 Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
Him andpcos Smartphrase:.REFENDOPCOS NOTE: patients with suspected PCOS are welcomed to endocrine clinic. There is also a PCOS clinic is available in the Ob/Gyn Department. I am referring @name@, a @age@
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Adrenal disease Real and Unreal. Objectives. Real
 Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
Adrenal disease Real and Unreal J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine UCSF Objectives Participants will: 1) understand the signs, symptoms, diagnosis and
ENDOCRINE FORMS OF HYPERTENSION. Michael Stowasser
 ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
ENDOCRINE FORMS OF HYPERTENSION Michael Stowasser Hypertension Unit, University Department of Medicine, Princess Alexandra Hospital, Brisbane 4102, Australia. ENDOCRINE FORMS OF HYPERTENSION Mineralocorticoid
4/23/2015. Objectives DISCLOSURES
 2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
2015 PENS Conference Savannah, GA Novel Cases of Congenital Hyperreninemic Hypaldosteronism Jan M. Foote DISCLOSURES I have no actual or potential conflicts of interest in relation to this presentation.
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
Tests that have had changes to the method/ CPT code, units of measurement, scope of analysis, reference comments, or specimen requirements.
 Updates In our continuing effort to provide you with the highest quality toxicology laboratory services available, we have compiled important changes regarding a number of tests we perform. Listed below
Updates In our continuing effort to provide you with the highest quality toxicology laboratory services available, we have compiled important changes regarding a number of tests we perform. Listed below
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas. Dilemmas in Management of Pheochromocytoma and Paraganglioma
 Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
Conferencia III: Dilemas en el tratamiento de Feocromocitomas y Paragangliomas Dilemmas in Management of Pheochromocytoma and Paraganglioma William F. Young, Jr., MD, MSc Mayo Clinic Rochester, MN, USA
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Spectrum of Hypertension & Hypokalemia
 Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
Spectrum of Hypertension & Hypokalemia Farheen K. Dojki, PGY-6 Hypertension Fellow, ASH Hypertension Center Dr. Dojki does not have any relevant financial relationships with any commercial interests. OBJECTIVES:
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
MedKorat Endocrine Day 2018 Approach to common adrenal disorder
 MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
MedKorat Endocrine Day 2018 Approach to common adrenal disorder Rungnapa Laortanakul, MD Nov.2018 Outline Adrenal insufficiency Cushing s syndrome Pheochromocytoma Primary Aldosteronism Adrenal incidentaloma
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Adrenal Update. Mohamed Ahmed MRCP(UK),MRCP-Endo(London),Diabetes Dip. Consultant Physician HEFT
,MRCP-Endo(London),Diabetes Dip. Consultant Physician HEFT") Adrenal Update Mohamed Ahmed MRCP(UK),MRCP-Endo(London),Diabetes Dip. Consultant Physician HEFT The adrenal steroidogenesis pathway 73 yrs. Female. The incidental adrenal mass Case 1 Incidental extremely
Adrenal Update Mohamed Ahmed MRCP(UK),MRCP-Endo(London),Diabetes Dip. Consultant Physician HEFT The adrenal steroidogenesis pathway 73 yrs. Female. The incidental adrenal mass Case 1 Incidental extremely
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
MANAGEMENT OF CAH IN ADULT PATIENTS. Mizuho Mimoto, MD, PhD Endorama June 22, 2017
 MANAGEMENT OF CAH IN ADULT PATIENTS Mizuho Mimoto, MD, PhD Endorama June 22, 2017 22 yo M with CAH presents with pruritis HPI: Several month history of progressive pruritis, worse in extremities (antecubital
MANAGEMENT OF CAH IN ADULT PATIENTS Mizuho Mimoto, MD, PhD Endorama June 22, 2017 22 yo M with CAH presents with pruritis HPI: Several month history of progressive pruritis, worse in extremities (antecubital
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
ComprehensivePLUS Hormone Profile with hgh
 OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
OLEBound400: 801 SW 16th St Suite 126 Renton WA 98057 425.271.8689 425.271.8674 (Fax) ComprehensivePLUS Hormone Profile with hgh Doctor ID Patient Name 6206 Doe, Jane Age Sex Date of Birth 44 F Date Collected
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment. Jamie Johnston, MD University of Pittsburgh School of Medicine
 Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Potassium, Aldosterone, and Hypertension: How Physiology Determines Treatment Jamie Johnston, MD University of Pittsburgh School of Medicine No Disclosures Acknowledgements: Evan Ray, MD, PhD Objectives
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
ADRENAL DISORDERS Anand Vaidya, MD MMSc
 ADRENAL DISORDERS Anand Vaidya, MD MMSc Director, Center for Adrenal Disorders Division of Endocrinology, Diabetes, & Hypertension Brigham and Women s Hospital Assistant Professor of Medicine, Harvard
ADRENAL DISORDERS Anand Vaidya, MD MMSc Director, Center for Adrenal Disorders Division of Endocrinology, Diabetes, & Hypertension Brigham and Women s Hospital Assistant Professor of Medicine, Harvard
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON
 When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON Conflict of interest None related to the topic When to look
Endocrine hypertension
 Endocrine hypertension Justyna Kuliczkowska-Płaksej Department of Endocrinology, Diabetes and Isotope Therapy Wroclaw Medical University Idiopathic hypertension (primary or essential) - 85% Secondary hypertension
Endocrine hypertension Justyna Kuliczkowska-Płaksej Department of Endocrinology, Diabetes and Isotope Therapy Wroclaw Medical University Idiopathic hypertension (primary or essential) - 85% Secondary hypertension
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
My favorite hypertensive patients. Entertaining you is Friedrich C. Luft
 My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Supplemental Data. Supplement to: Abiraterone Acetate to Lower Androgens in Classic 21-Hydroxylase Deficiency
 Supplemental Data Supplement to: Abiraterone Acetate to Lower Androgens in Classic 21-Hydroxylase Deficiency Richard J. Auchus, Elizabeth O. Buschur, Alice Y. Chang, Gary D. Hammer, Carole Ramm, David
Supplemental Data Supplement to: Abiraterone Acetate to Lower Androgens in Classic 21-Hydroxylase Deficiency Richard J. Auchus, Elizabeth O. Buschur, Alice Y. Chang, Gary D. Hammer, Carole Ramm, David
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013
 3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
3- & 12-Year-Old Sisters with Li-Fraumeni Syndrome KRISTEN DILLARD, M.D. ENDORAMA FEBRUARY 28, 2013 Presentation Sisters referred by Peds Oncology to Endo clinic for adrenocortical carcinoma screening
A 64 year old man referred for evaluation of suspected hyperaldosteronism
 A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
A 64 year old man referred for evaluation of suspected hyperaldosteronism Dr. Dickens does not have any relevant financial relationships with any commercial interests. ENDORAMA: 64 year old man referred
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management
 Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Adrenal Insufficiency During Pregnancy
 Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Disclosures Adrenal Insufficiency During Pregnancy Research funding from Diurnal Limited via NIH CRADA mechanism Deborah P. Merke, M.D., M.S. Bethesda, MD Outline Primary Adrenal Insufficiency Physiological
Il Carcinoma Surrenalico
 Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
Il Carcinoma Surrenalico Massimo Terzolo Medicina Interna I AOU San Luigi Orbassano (TO) Italy AGENDA DIAGNOSIS CLINICAL PRESENTATION IMPACT ON PROGNOSIS TREATMENT DIAGNOSIS 23-yr-old lady October 2010,
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Pediatric Hypertension. Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019
 Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Pediatric Hypertension Alisa A. Acosta, MD, MPH Asst. Professor, Renal Section April 5, 2019 Objectives Recognize the importance of accurate blood pressure measurement in pediatric patients Define pediatric
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the bod
 The Players Part II The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the body Can affect all hormone systems
The Players Part II The Adrenals Are a key factor in all hormonal issues Because the adrenals can convert one hormone to another they play a role like no other in the body Can affect all hormone systems
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the