SC #06. Common Challenging Problems in Bone and Soft Tissue Pathology. Andrew L. Folpe, MD Mayo Clinic Rochester, MN
|
|
|
- Hector Strickland
- 5 years ago
- Views:
Transcription

1 SC #06 Common Challenging Problems in Bone and Soft Tissue Pathology Andrew L. Folpe, MD Mayo Clinic Rochester, MN Andrew E. Horvai, MD, PhD University of California, San Francisco San Francisco, CA




2 Short Course #06 Common Challenging Problems in Bone and Soft Tissue Pathology USCAP 2015 Common problems in bone and soft tissue pathology: Introduction to bone pathology. Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Disease of bone Approach to bone diagnosis Pathology Clinical Relative incidence 8 million thousands Imaging 1



3 Approach to bone diagnosis Pathology Imaging Clinical Fracture Non-ossifying fibroma Osteoporosis Pathology Clinical Imaging Metastatic carcinoma Myeloma, lymphoma Pleomorphic undifferentiated sarcoma Approach to bone diagnosis: Necessary information Clinical : Age Location Pain Underlying disease: hyperparathyroidism, IVDU Radiology: Definitions Histology Clinical: Age Age Benign Malignant <10 Unicameral bone cyst, Langerhans Skeletal dysplasias Acute osteomyelitis Non-ossifying fibroma, ABC, osteochondroma, osteoblastoma, chondroblastoma Enchondroma, Giant cell tumor >40 Osteoma Osteonecrosis Renal osteodystrophy Paget disease Ewing, Leukemia/Lymphoma Osteosarcoma Ewing Adamantinoma Chondrosarcoma Myeloma, Chondrosarcoma, Chordoma Clinical: Pain Pain: Growing lesion Pathologic fracture Local tissue reaction Osteoid osteoma: Night pain, relieved by aspirin or NSAIDs Grade 1 chondrosarcoma: Usually painful vs. enchondroma (painless, unless fracture). 2



4 Clinical: Location epiphysis Chondroblastoma Giant cell tumor Clear cell chondrosarcoma Radiology: Modalities Plain radiographs*: 2 views metaphysis Osteosarcoma Osteochondroma Aneurysmal bone cyst Non-ossifying fibroma CT: Axial location, permeative lesions diaphysis Fibrous dysplasia Osteoid osteoma Ewing sarcoma Adamantinoma Lymphoma MRI: Soft tissue, neurovascular, surgical planning Radiology: Patterns of growth Radiology: Opacity Opacity Border Periosteum Lytic B Sclerotic 3













5 Radiology: Border Radiology: Periosteum Marginated Circumscribed Permeative Solid Codman s triangle Spiculated Histology: what is normal? Lamellar Always abnormal: woven bone Lamellar Woven Marrow: fat and hematopoetic cells only Lacunae contain osteocytes Evenly spaced cement lines Remodeling <20% of surface Neoplasms Osteoblastoma Osteosarcoma Inflammatory Osteomyelitis Metabolic/Developmental Osteogenesis Imperfecta Osteopetrosis 4


 Artifact")



6 Always abnormal: excess cement lines Paget disease Always* abnormal: Empty lacunae Empty lacunae Neoplasms Low grade osteosarcoma Inflammatory/Metabolic Paget disease Necrosis Inflammatory Bone infarct Radiation osteonecrosis Osteomyelitis (sequestrum) Artifact (overdecalcification) Interstitial lamellae Always abnormal: Marrow replaced Chondrosarcoma Always abnormal: Excess remodeling Hyperparathyroidism Neoplasms Chondrosarcoma Metastasis Hematolymphoid Inflammatory Osteomyelitis Metabolic/Developmental Fibrous dysplasia Xanthomatosis Inflammatory Paget disease Chronic osteomyelitis Metabolic/Developmental Hyperparathyroidism Renal osteodystrophy 5


 Chondrosarcoma variants Dedifferentiated chondrosarcoma")
 Andrew Horvai MD PhD Clinical")

7 Cartilage: what is normal Widely dispersed chondrocytes Small, dark chondrocyte nuclei Always abnormal: Cartilage High cellularity Large bizzare chondrocytes Myxoid matrix solid hyaline matrix USCAP 2015 Common problems in bone and soft tissue pathology: Cartilage tumors Outline Common intramedullary tumors Enchondroma Conventional chondrosarcoma ( atypical cartilage tumor ) Chondrosarcoma variants Dedifferentiated chondrosarcoma Mesenchymal chondrosarcoma Clear cell chondrosarcoma (Chondroblastoma to be discussed with giant cell rich lesions) Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Pitfalls and controversies Grading Malignant transformation from benign tumors Cartilage tumors of small bones of hands and feet 6


 Malignant transformation 15-20% 20-30%")
 Autosomal dominant 8q24, 11p11 EXT1, EXT2 Deformities of forearm, knee, short")
8 Principles: Definitions Unifying characteristics Collagen II Proteoglycan matrix 65% water Aggrecan most common Chondrotoin and Keratan sulfate side chains Principles: Radiology Ring-like calcifications Principles: Treatment Principles: Syndromes Enchondroma Observation Grade 1 chondrosarcoma, chondroblastoma Grade 2-3 chondrosarcoma Curettage and cement Wide local excision +/- chemo Dedifferentiated chondrosarcoma Wide local excision + chemotherapy Syndrome MOI* Locus Genes Associated conditions Ollier disease Sporadic 2q33, 15q26 IDH1, IDH2 Maffucci syndrome Sporadic Spindle cell hemangiomas (Glomangiomas Angiosarcomas Hepatobiliary) Malignant transformation 15-20% 20-30% Mesenchymal chondrosarcoma Wide local excision + chemotherapy Clear cell chondrosarcoma Wide local excision Multiple hereditary exostoses (osteochondromas) Autosomal dominant 8q24, 11p11 EXT1, EXT2 Deformities of forearm, knee, short stature 5-35% *MOI: Mode of inheritance 7



9 Ollier / Maffucci syndrome Malignant transformation of sporadic cartilage tumors Enchondroma: Case reports, <<1% Osteochondroma: 1 8% Synovial chondromatosis: <1% Ollier Case A 16 year old girl, incidentally discovered proximal tibia lesion No pain, no palpable mass. 8






10 Case A Case A Enchondroma Pitfalls: Enchondroma Necrosis Mucin in lacunae Clinical Radiology Histology Ddx Age: All Loc: Hands/feet, long tubular bones ~3% of adults Metaphysis Lytic, lobular Ring calcifications Intact cortex Lobular Peripheral ossification No permeation Low cellularity No atypia/mitoses Grade 1 Chondrosarcoma 9





11 Pitfalls: Enchondroma Binucleation Case B 57 year old man with painful hip for 2 months Needle biopsy performed of acetabular mass enchondroma chondrosarcoma 10


 Cortical")



12 Case B Case B Conventional chondrosarcoma Grade 1 chondrosarcoma or enchondroma? Clinical Radiology Histology Ddx Age: 50+ Loc: pelvis, metadiaphysis long bones Large (> 5 cm) Cortical disruption Endosteal scalloping Soft tissue extension Permeates viable, lamellar bone Myxoid change Hypercellular Atypia open chromatin Mitoses Enchondroma Clear cell chondrosarcoma Chondroblastic osteosarcoma Histology Radiology Molecular Pathology 11

 Pitfalls Small biopsy Curettage Endochondral ossification Mirra JM et al.")
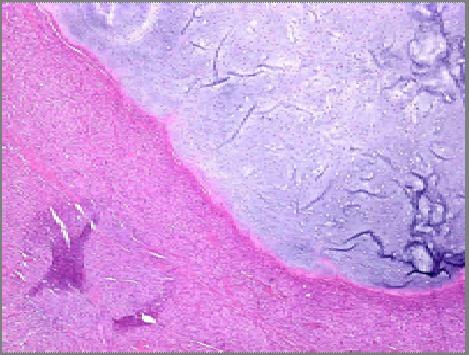
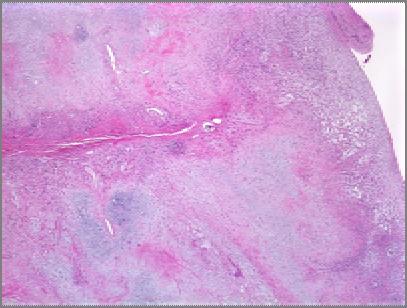
13 Enchondroma or Grade I chondrosarcoma: Histology Chondrosarcoma: Permeation Enchondroma: Multiple nodules of hyaline cartilage separated by normal marrow (and) plates of lamellar bone that conform to the irregular shapes of cartilage lobules. Kappa ~ 0.5 Two features >95% sensitivity and specificity Permeation = host bone entrapment > 20% myxoid matrix Eefting D et al. Am J Surg Pathol :50-57 Chondrosarcoma: Single confluent mass of cartilage trapping host lamellar bone or invasion into Haversian or Volkman systems. J. Mirra (1985) Pitfalls Small biopsy Curettage Endochondral ossification Mirra JM et al. Clin Ortho Rel Res : Permeation: host bone entrapment Permeation 12






14 Chondrosarcoma: permeation Permeation Permeation Enchondral ossification Chondrosarcoma: Myxoid change Enchondroma or Grade 1 chondrosarcoma: Radiology Most predictive Least predictive Pathologic fracture Axial skeleton Infiltrating margin Soft tissue mass Size > 5 cm Lobulated contour Periosteal reaction Cortical disruption or thickening Deep endosteal scalloping Murphey MD et al. Radiographics (5): Brien EW et al. Skeletal Rad 1997; 26(6) Giuffrida AY et al. J Bone Joint Surg Am :
 Enchondroma (n=14) and CHUMP (n=3): karyotypicallynormal Grade I chondrosarcoma: Numerical and structural aberrations (n=3).")

15 Enchondroma or Grade I chondrosarcoma: Molecular Genetic and molecular features: Karyotype: (C.H.A.M.P. study) Enchondroma (n=14) and CHUMP (n=3): karyotypicallynormal Grade I chondrosarcoma: Numerical and structural aberrations (n=3). Comparative genomic hybridization: Enchondroma: 13q21; 19, 22q Chondrosarcoma: 2 11, 14, 15, 18, 21 Similar numbers of aberrations Exome sequencing: COL2A1, IDH1, IDH2, TP53 Chondrosarcoma: Histologic Grading Grade 1 Grade 2 PROGNOSTIC FACTORS IN CHONDROSARCOMA OF BONE A Clinicopathologic Analysis with Emphasis on Histologic Grading Histology HARRY L. EVANS, M.D.* ALBERTO G. AYALA, MD AND MARVIN M. ROMSDAHL, MD, PHD Cancer 40: , Hypercellular, uniform but hyperchromatic nuclei, nuclear detail not visible Diffusely hypercellular, nuclei paler with visible intranuclear detail 5 year survival year survival Tallini G et al. J Pathol, 2002; 196(2):194 Ozaki T et al. Anticancer Res 2004; 1721 Amary MF et al. J Pathol. 2011; 334. Szuhai, et al. Cancer Genet 2012; 193. Tarpey PS et al. Nat Genet 2013; 923. Grade 3 Sheets of cells, larger nuclei, mitotic activity > 2mf/10 hpf Grade 1 Chondrosarcoma Grade 2 Chondrosarcoma 14

, painful, pathologic fracture")

16 Grade 2 Chondrosarcoma Grade 3 Chondrosarcoma Grade 3 Chondrosarcoma Pitfall: cartilage tumors of the hands and feet Enchondroma of hands and feet Clinical: Very common site (~30% of all enchondromas), painful, pathologic fracture common Radiographs: Cortical erosion common Histology: Hypercellular, myxoid change, nuclear hyperchromasia, permeation within medulla 15




:676 90. Bovee JV et al.")
17 Enchondroma of the phalanx Enchondroma of the phalanx Summary: chondrosarcoma of small bones of hands and feet Metacarpals, metatarsals, wrist and ankle: Soft tissue extension, Grade 3 cytology Behavior similar to chondrosarcoma grade 1 at other sites Phalanges: Soft tissue extension Metastatic rate is very low (<2%) Local resection is favored over amputation Dedifferentiated chondrosarcoma Ogose A et al. Cancer, (1):50 9 Ostrowski ML et al. Am J Surg Pathol, (6): Bovee JV et al.cancer, (9):

 Abrupt transition: 1. Chondrosarcoma grade 1 2.")

18 Dedifferentiated chondrosarcoma Dedifferentiated chondrosarcoma Dedifferentiated chondrosarcoma Dedifferentiated chondrosarcoma Clinical Radiology Histology Ddx Age: Adult >50 Loc: Pelvis>Femur> Humerus 5 year survival < 10% Metaphysis Bimorphic (especially on MRI) Abrupt transition: 1. Chondrosarcoma grade 1 2. osteosarcoma/ MFH / fibrosarcoma Chondroblastic osteosarcoma -Less abrupt transition -High grade cartilage component Mesenchymal chondrosarcoma -Young patients -Benign cartilage islands -Less abrupt transition 17


19 Dedifferentiated chondrosarcoma ~100% mortality Chondroblastic osteosarcoma ~30% mortality Mesenchymal chondrosarcoma Mesenchymal chondrosarcoma Mesenchymal chondrosarcoma 18



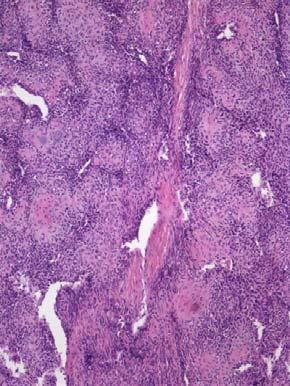
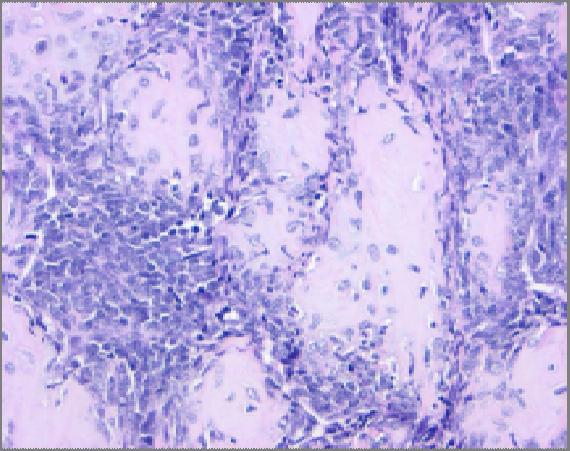
20 Mesenchymal chondrosarcoma Mesenchymal chondrosarcoma Clinical Radiology Histology Ddx Age: Loc: Jaw, rib, pelvis, soft tissue Multifocal 10yr survival 25% Variable course Lytic Ring calcifications Rarely circumscribed 1. Cartilage islands/perivascular 2. Small round blue cell tumor HPC-ish vessels common CD99, S100*, desmin Ewing sarcoma Dediff chondrosarc Small cell osteosarcoma Genetics: Inv(8q21.1;8q13.3) HEY1 NCOA2 Wang L, Genes Chromosomes Cancer 51:127. Clear cell chondrosarcoma Clear cell chondrosarcoma 19

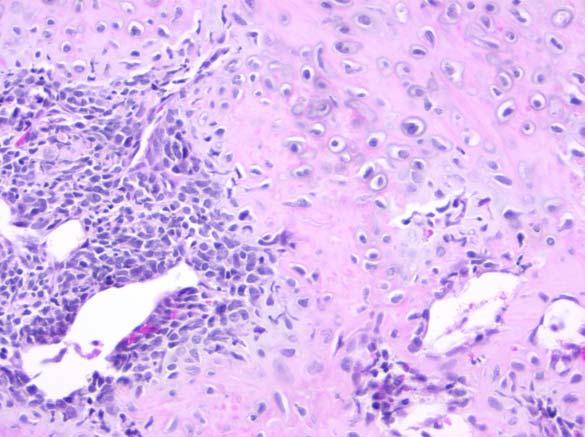
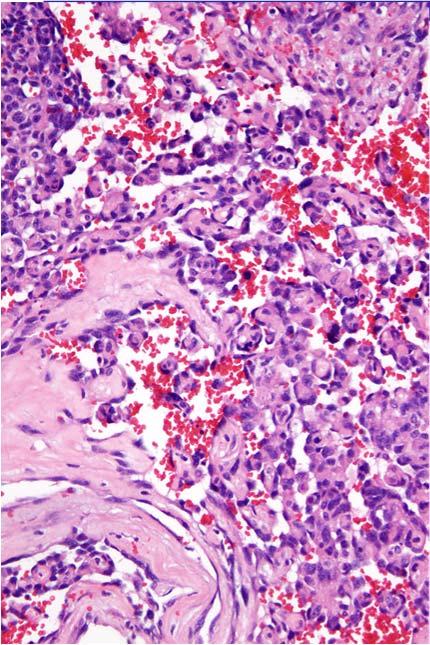
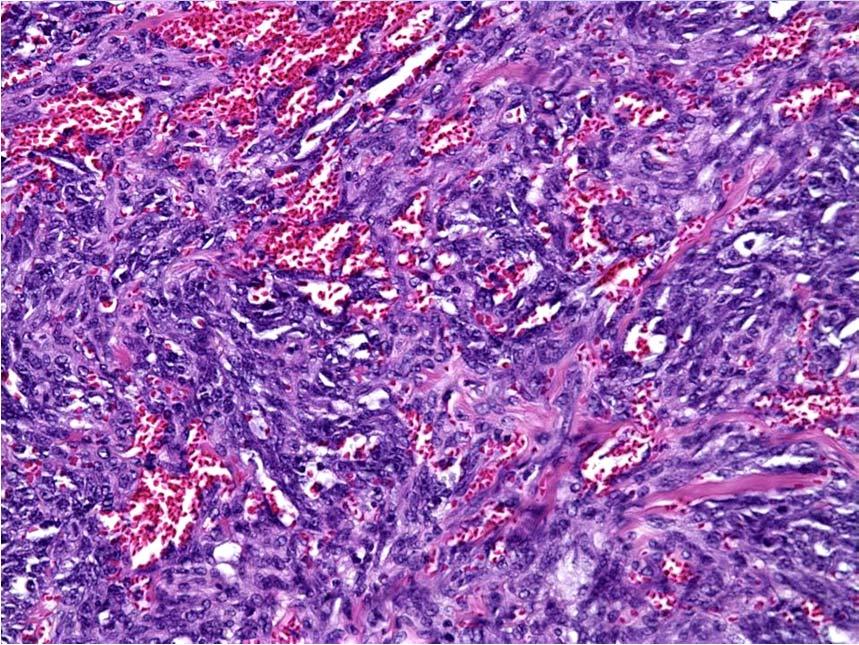
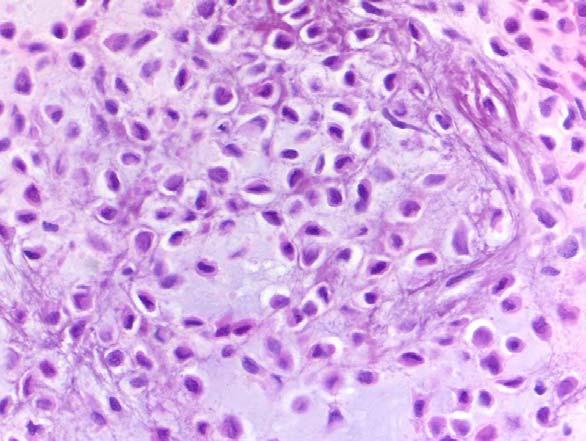
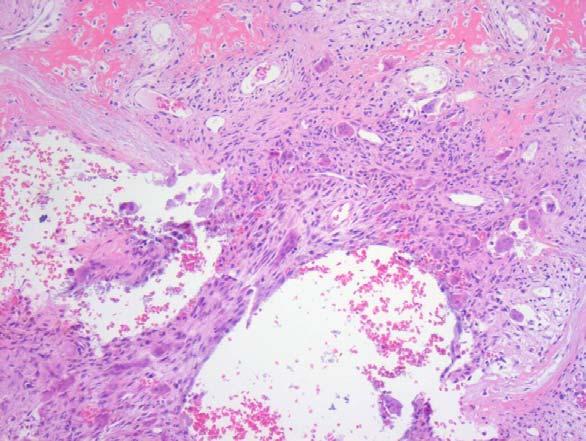
21 Clear cell chondrosarcoma Clear cell chondrosarcoma Clinical Radiology Histology Ddx Age: M>F Loc: Proximal femur Skull, rib, spine Slow growing ~25% Metastasize ~15% mortality Epiphysis Circumscribed Early: lytic, septae Late: sclerotic Permeates Osteogenic No hyaline cartilage Clear cells, well defined membrane, macronucleoli Chondroblastic osteosarcoma Osteoblastoma Chondroblastoma (radiology Ddx) Take home messages Correlation of radiologic, clinical and histologic features are critical, especially in low grade cartilage lesions. Permeation is the most sensitive histologic criterion separating enchondroma from chondrosarcoma. Chondrosarcoma of small bones of the hands and feet should be diagnosed with caution. Chondrosarcomas, especially grade 1, are predominantly locally aggressive, but local disease can be fatal even in the absence of metastases Dermatofibrosarcoma Protuberans and Cutaneous Fibrous Histiocytoma Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN 20


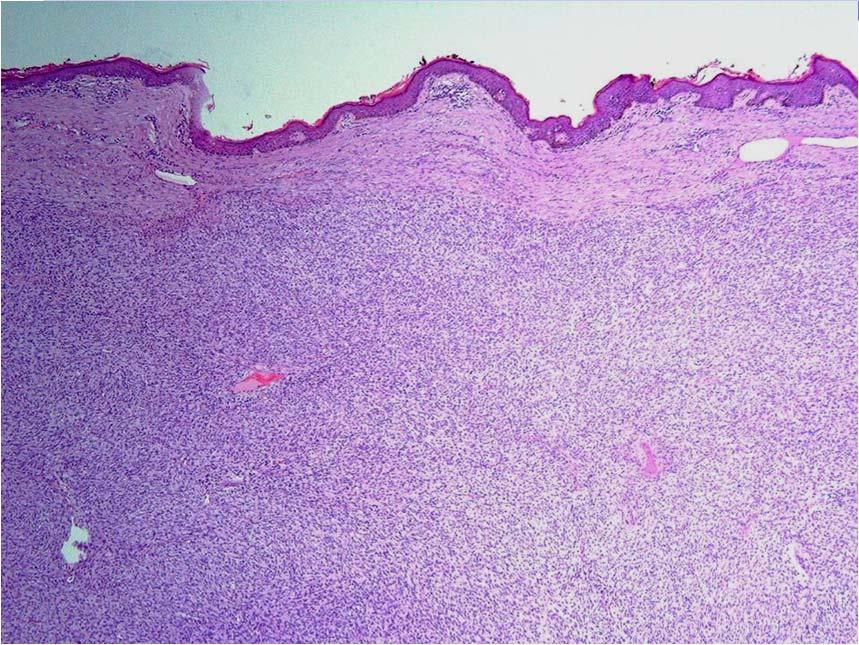
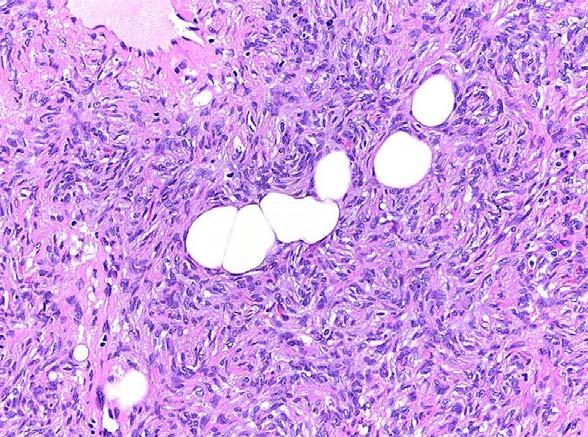
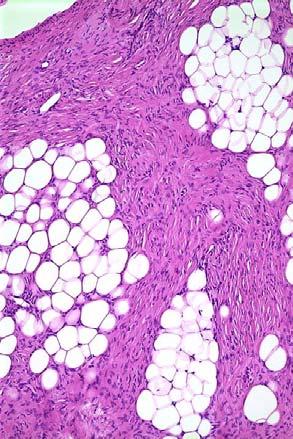
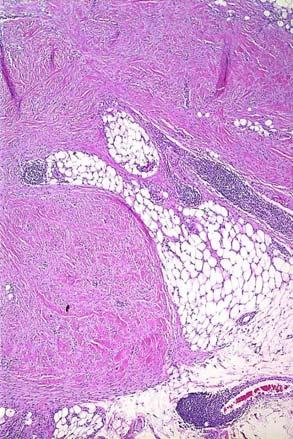
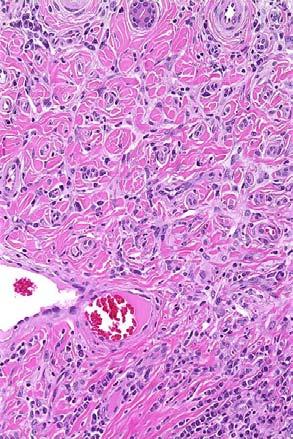
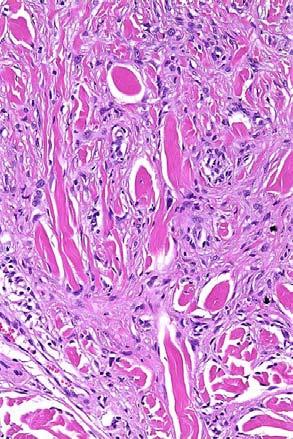
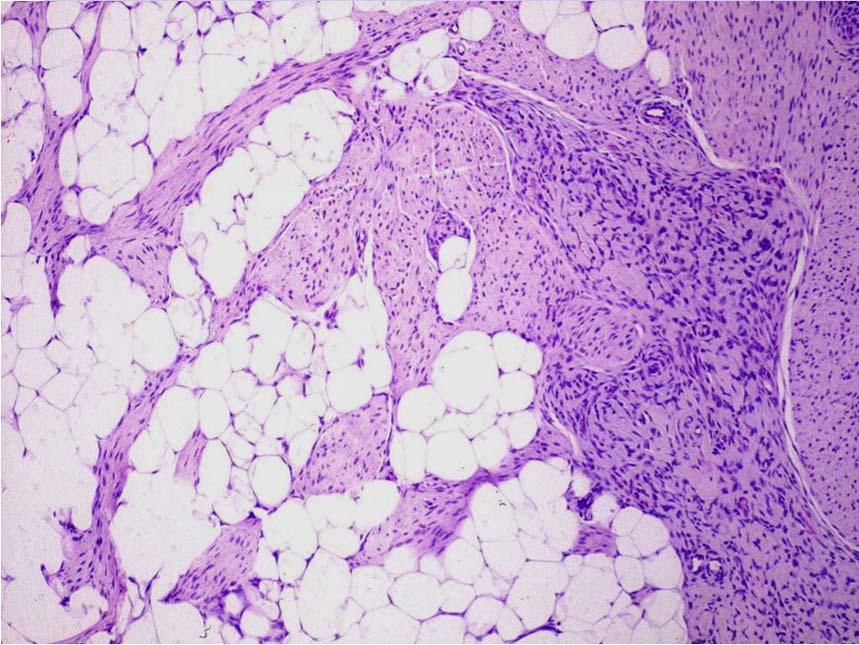
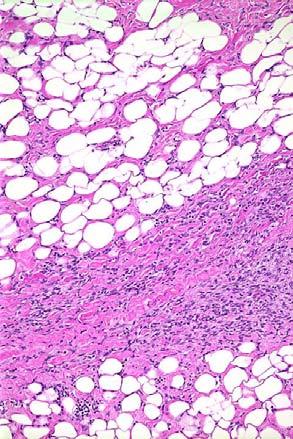
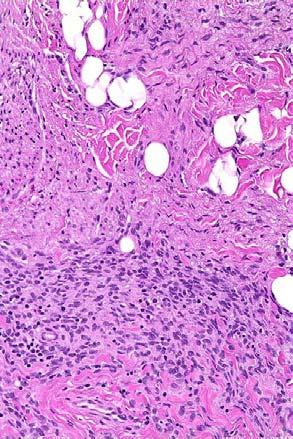
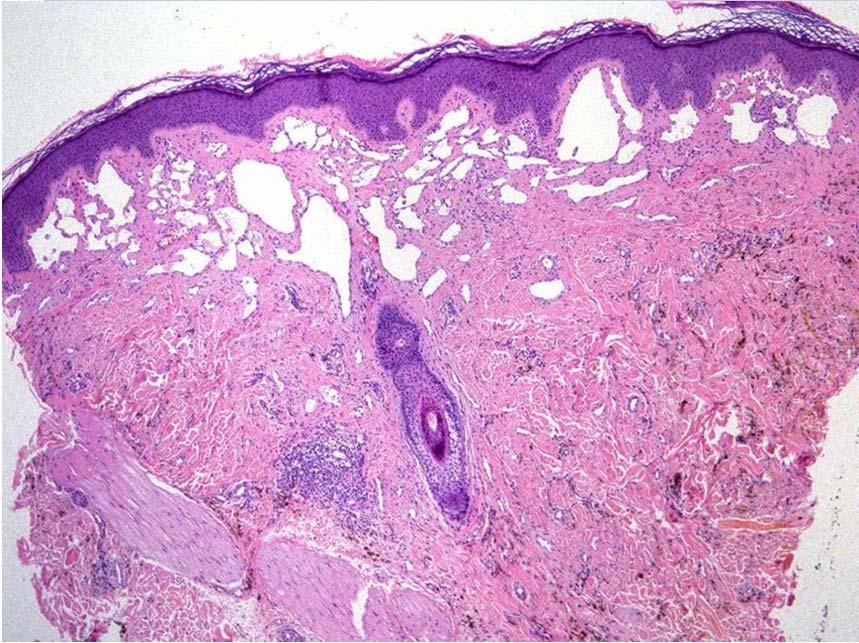
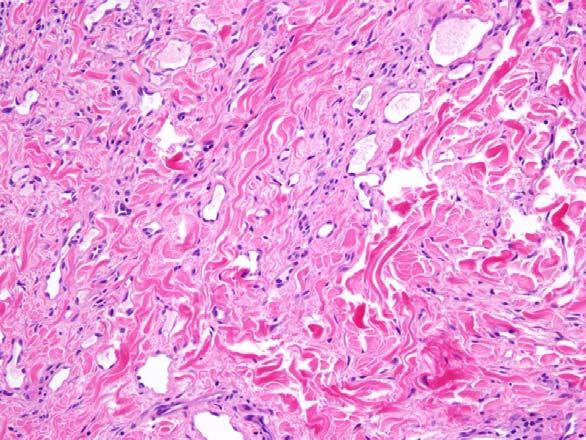
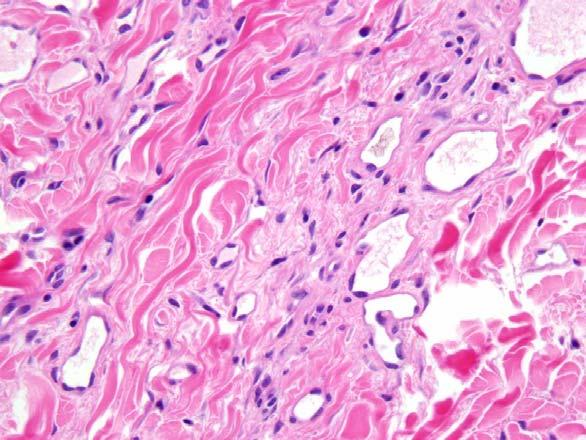
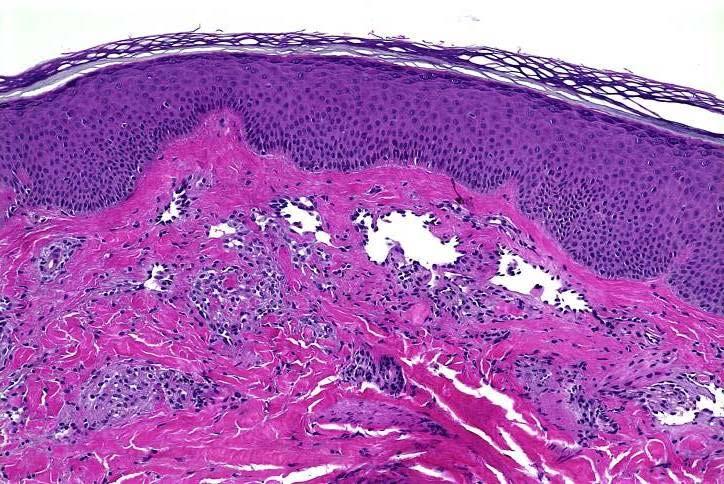
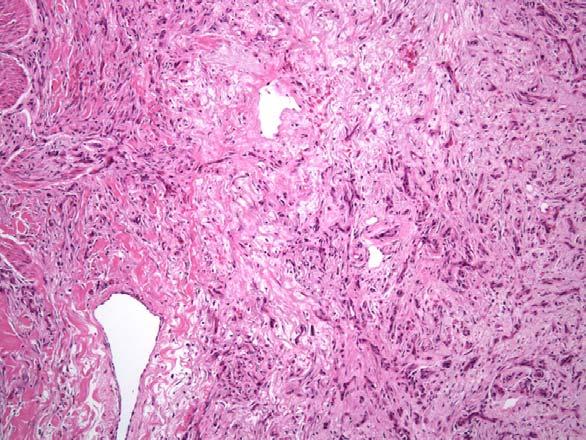
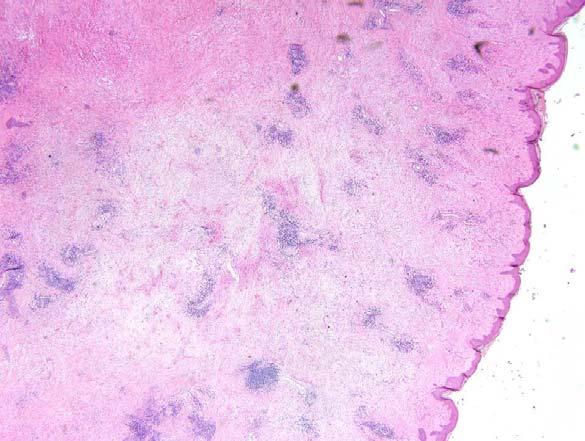
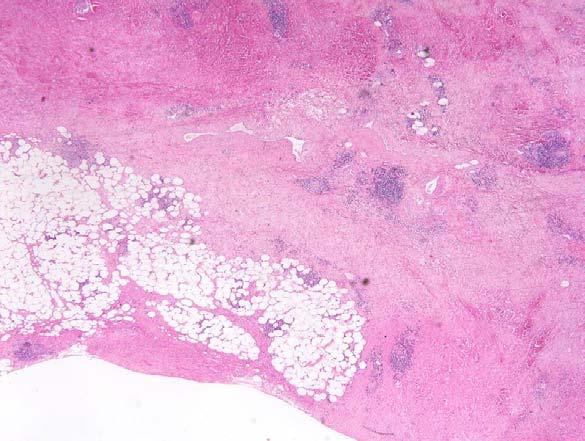
22 Most common in young to middle aged adults Usually occurs in trunk and proximal extremities Initially presents as plaque, with progression to uni/multinodular mass Plaque stage may mimic sclerosing dermatitis Nodular DFSP may have only clinically subtle dermal involvement and present as subcutaneous mass 2011 MFMER slide-82 Histopathology Uniform storiform growth, sometimes with short fascicles Monotonous, slender spindled cells with lightly eosinophilic cytoplasm and dark nuclei Honeycomb pattern of infiltration around individual adipocytes Low mitotic rate Lacks epidermal hyperplasia, siderophages, foamy macrophages, multinucleated giant cells Almost always intensely CD34-positive; usually negative for S100 protein, actins, desmin 21

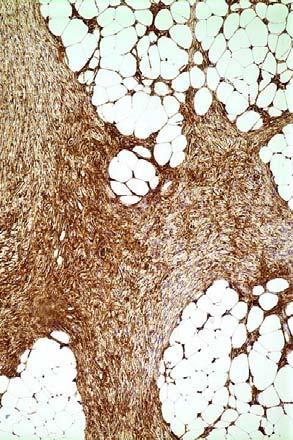
23 CD34 22




24 Important Variants Atrophic Presenting as a subcutaneous mass Myxoid With myoid nodules Pigmented (Bednar tumor) 23
 Often presents as new,")


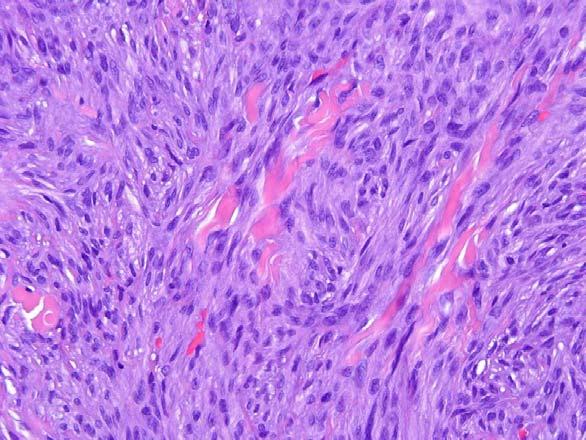
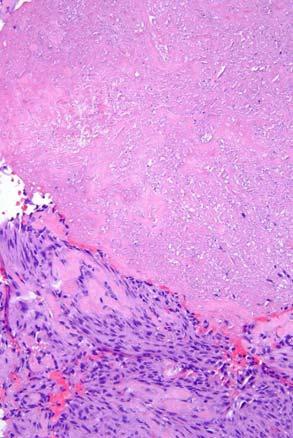
25 Fibrosarcomatous Change Exact incidence difficult to determine (<5-16%) Often presents as new, rapidly growing nodule Should account for 5-10% of tumor, usually with abrupt transition from typical DFSP Fascicular growth pattern Increased mitotic activity Greater cytologic atypia Often diminished CD34 expression 2011 MFMER slide-96 24
 Conventional wide (2-3cm) excision")
 in DFSP,")
 Unclear whether wide excision")



26 CD34 Outcome Local recurrence Identical for DFSP and FS-DFSP (20-50%) Conventional wide (2-3cm) excision lowers recurrence rate to <20% Moh s surgery reduces LR rate to 2-7% Metastasis Very rare (<2%) in DFSP, almost always in recurrent tumors Higher metastatic risk in FS-DFSP (~15%) Unclear whether wide excision has any impact on metastatic risk 2011 MFMER slide-100 Excision Pathology Uniform fibrohistiocytic cells in a whorled pattern with collagen and fat entrapment Deep to the above proliferation Proliferation of atypical spindled cells with hyperchromasia Numerous mitoses Occasional herringbone pattern Deep margin involved 25

 COL1A1/PDGF-β fusion gene, resulting in autocrine growth")




27 Genetics Liver Met Supernumerary ring chromosomes by conventional cytogenetics Subsequently found to contain occult t(17;22) (q22;q13.1) COL1A1/PDGF-β fusion gene, resulting in autocrine growth stimulation Identical fusion found in giant cell fibroblastoma PDGF-β Primary CD34 Targeted Therapy Giant Cell Fibroblastoma Now known to be juvenile variant of DFSP Histologic overlap with hybrids GCFB recurrent as DFSP and vice versa Almost always occurs in 1 st decade; very rare in adults Usually located in trunk and proximal extremities Myxoid to hyalinized stroma Monomorphic, spindled cells infiltrating fat Pseudovascular spaces lined by large, hyperchromatic multinucleated cells Frequent local recurrences; metastases and fibrosarcomatous change extremely rare 26


28 Differential Diagnosis Fibrous histiocytoma variants Diffuse neurofibroma Lipofibromatosis Fibrous hamartoma of infancy Cellular Fibrous Histiocytoma Proximal extremities, head and neck Lightly eosinophilic spindled cells, fascicular to storiform pattern Lacks siderophages, giant cells and foam cells Necrosis in 10%; mitotic figures frequent Limited involvement of subcutaneous fat Key is recognition of ordinary BFH 20-30% local recurrence rate Complete excision recommended 27

29 28






30 Aneurysmal Fibrous Histiocytoma Darkly pigmented, often thought to be vascular or melanocytic tumor May be large at time of diagnosis Plump spindled cells in a fascicular to tight storiform pattern Hemorrhage with siderophages Key is identifying features of ordinary BFH Behavior similar to C-BFH Factor XIIIa CD34 29


 Behavior")
31 Atypical Fibrous Histiocytoma Clinically similar to conventional BFH/ dermatofibroma Low power resemblance to ordinary BFH High power examination shows foci of markedly atypical, sometimes multinucleated cells, with mitotic figures (including atypical forms) Behavior similar to cellular BFH 30



32 Differential Diagnosis: AFX Usually much older patients Sun damaged skin Absence of areas of BFH IHC in the Diagnosis of BFH Multiple cell populations Factor XIIIA-positive dendrocytes CD34-positive interstitial cells S100 protein-positive Langerhans cells CD68-positive macrophages Actin-positive myofibroblasts May show a peripheral rim of reactive CD34-positive cells 31







33 Factor XIIIA CD34 CD68 S100 CD34 Metastasizing BFH Approximately 20 reported cases Most often associated with cellular FH, but reported with all subtypes May be related to repeated local recurrences No histologic features of primary tumors predictive of metastasis Cases reported as cystic fibrohistiocytic tumor of the lung represent metastatic BFH Prognosis generally favorable if metastases can be completely resected; rare deaths from disease 32



34 Lipofibromatosis Formerly known as infantile or juvenile fibromatosis Usually occurs in infants and young children Most common in distal extremities Poorly circumscribed, partially fatty-appearing, infiltrative Histopathology Admixture of adipose tissue and short fascicles of immature-appearing, bland, fibroblastic cells CD34-negative or very weakly positive Frequent local recurrences, no metastases 33



35 Diffuse Neurofibroma Children and young adults Usually occurs in head and neck Associated with NF1 in 10% Histopathology Bland, round cells, diffusely infiltrating dermal structures and fat Myxoid, finely fibrillary matrix Wagner-Meissner bodies S100 protein-positive, usually CD34-negative May recur locally, extremely low risk of malignant transformation Fibrous Hamartoma of Infancy Infants and very young children Much more common in males Axillary region, proximal extremities Triphasic, organoid appearance Mature fat Variably hyalinized, fibroblastic zones Nodules of primitive-appearing mesenchymal cells Often CD34-positive Benign with potential for local recurrence S100 34

36 35

 Arteriovenous fistula-related Prosthetic")
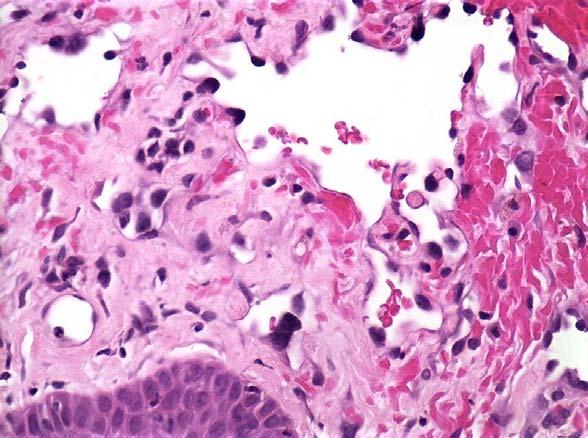
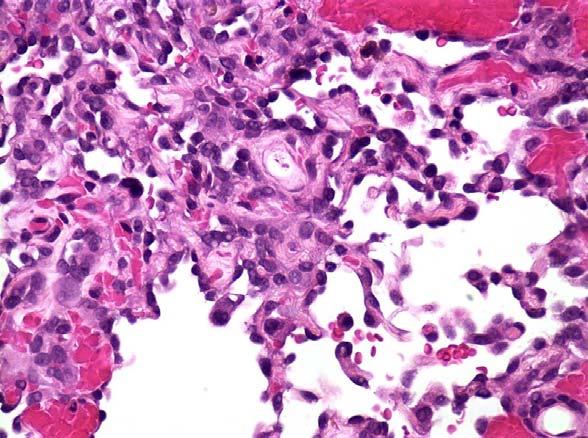
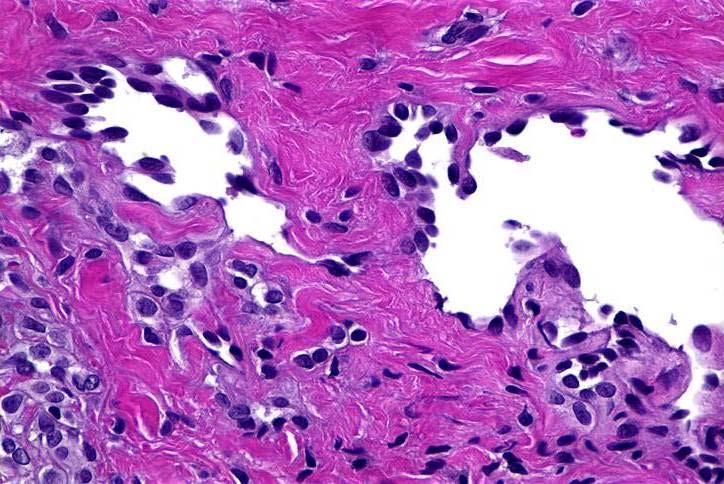
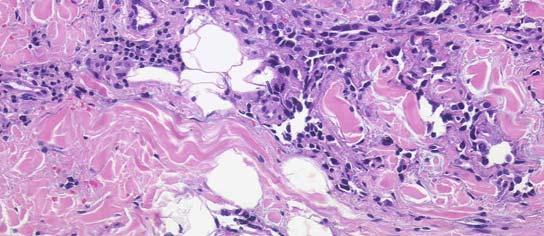
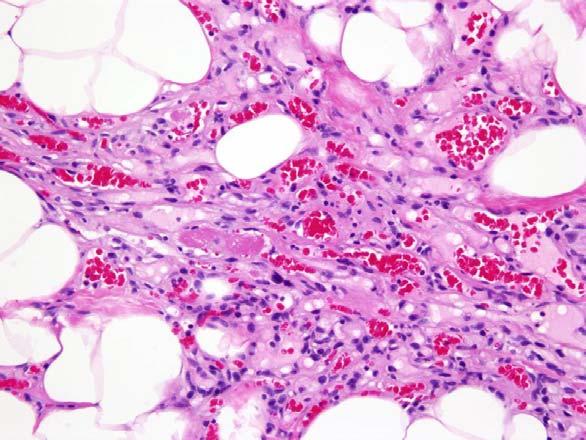
37 Overview Post-Irradiation Vascular Proliferations Radiation-associated vascular proliferations Selected benign mimics of angiosarcoma Andrew L. Folpe, MD Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN Iatrogenic Angiosarcomas Secondary to chronic lymphedema (Stewart-Treves) Arteriovenous fistula-related Prosthetic material-associated Thorotrast-related Following breast-conserving surgery and irradiation AS arising in chronic lymphedema 36
38 Cahan Criteria For Radiation- Induced Sarcoma History of radiation to the tissue in which the sarcoma arises The latency period between radiation therapy and diagnosis is relatively long (usually >10 years) The second malignancy arises within the area of radiation treatment The new disease is pathologically distinct from the primary malignancy Post-irradiation Cutaneous Angiosarcomas of the Breast Prior to 1970 s: Radical and modified radical mastectomy Lymphedema-associated AS Late 1970 s- present time: Breastconserving surgery plus axillary LN dissection plus adjuvant breast irradiation 1981: Maddox and Evans (MDACC) reported first cutaneous post-irradiation breast angiosarcoma Incidence and Prevalence Approximately 300 reported cases Overall incidence estimated at % of patients receiving WLE+RT Approximately 10-fold RR Incidence appears to be increasing Report of 0.03% incidence in a single institution (Orange, CA) Clinical Features Almost always women Wide age range (median 60 years) Skin of breast or chest wall, much less commonly breast parenchyma Post-radiation interval may be very short (< 3 years) but typically > 5 years Violaceous or erythematous plaques, nodules, or areas of eccymoses Variable in size Frequently multicentric 37



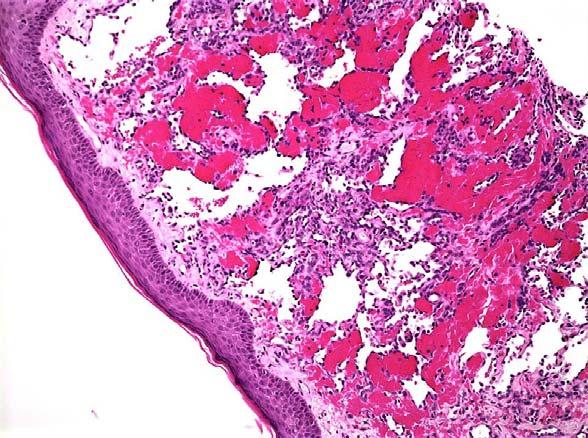
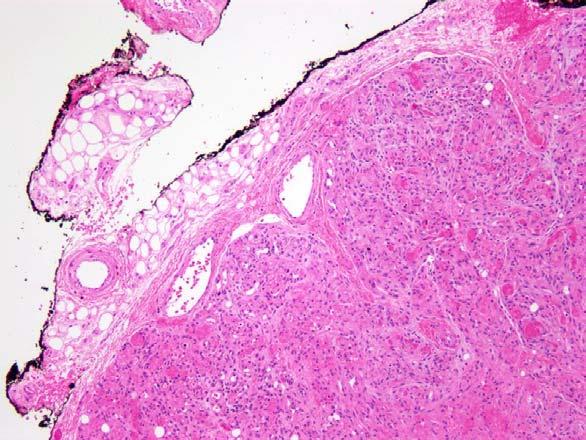
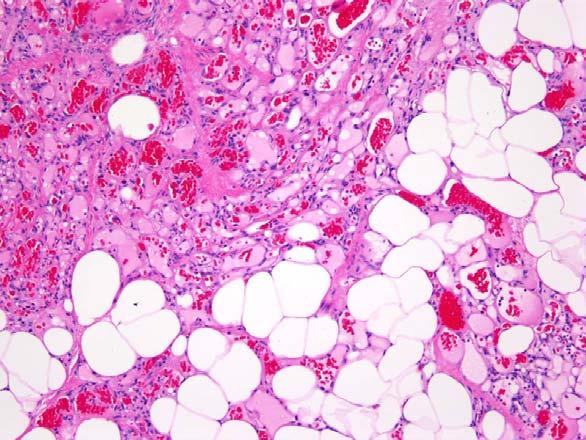
39 Angiosarcoma Most are histologically high-grade Highly malignant-appearing cells Diffuse dermal infiltration by poorly formed vascular channels Endothelial mitotic activity and multilayering Occasional cases appear low-grade Vessels are relatively well-formed but infiltrative Subtle nuclear atypia and rare mitoses No study to date has convincingly shown histopathological grading to accurately stratify patients with angiosarcoma All should be regarded as clinically high-grade 38
40 39


41 40
; usually occur after multiple LR Nearly 50% ultimately metastasize to lungs, contralateral breast, skeleton Approximately 35% of patients dead of disease in less than 3")
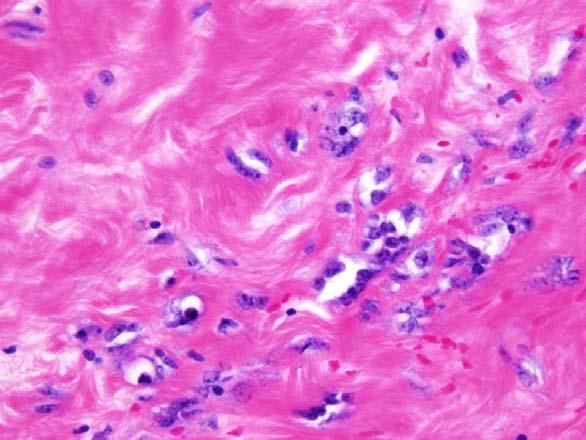
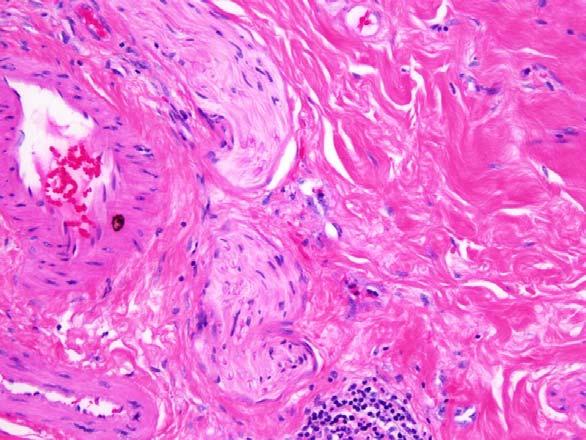
42 Outcome May be impossible to completely excise Over 70% will recur with surgery alone 84% of LR are < 1yr LR occur in >40% of patients treated with radical salvage surgery Metastases extremely uncommon at presentation (<1%); usually occur after multiple LR Nearly 50% ultimately metastasize to lungs, contralateral breast, skeleton Approximately 35% of patients dead of disease in less than 3 years MSKCC series: Median survival of post-rt breast AS (2.6 yrs) worse than for de novo AS (5.1 yrs) Radiation-Associated Cutaneous Vascular Proliferations Fibrosis with increased vascularity Benign lymphangiomatous papules Atypical vascular lesions Angiosarcoma Benign Lymphangiomatous Papules Also known as lymphatic-type atypical vascular lesions Solitary, well-circumscribed, superficial Dilated lymphangioma-like spaces lined by slightly enlarged, uniform endothelial cells Absent nuclear atypia, mitotic activity or endothelial multilayering BLAP 41


43 BLAP 42
; originally regarded as benign Solitary or")


44 Atypical Vascular Lesions Described by Fineberg and Rosen (1994); originally regarded as benign Solitary or multicentric Relatively circumscribed proliferation of small, irregular vascular spaces Endothelial cells may be hyperchromatic but lack significant nuclear atypia No endothelial stratification or mitotic activity Confined to dermis AVL AVL- Suspicious for AS 43
45 44



46 AVL Clinical Behavior Multiple synchronous or metachronous lesions in 10-20% Local recurrences in 7-20% Progression to angiosarcoma in 0-6% Unclear significance True precursor lesions? Markers of patients at risk for angiosarcoma? Unrelated radiation-related vascular proliferations? Early angiosarcomas? Significant interobserver variability Must be completely excised to exclude AS; long-term follow-up with rebiopsy of new or recurrent lesions within radiation field 45
 Oncogene located on 8q24 Stimulates")


47 MYC in Post-Radiation Vascular Lesions of the Breast (Mentzel et al, Mod Pathol 2012; 25: 75-85) Oncogene located on 8q24 Stimulates angiogenesis, may promote invasion and metastasis High level MYC amplification, detectable by IHC and FISH, seen in all postradiation cutaneous AS Amplification absent in BLAP, AVL, and primary AS Suggests either that AVL are not AS precursors, or require secondary MYC amplification to progress to AS 46



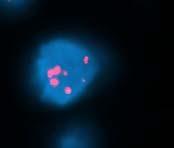
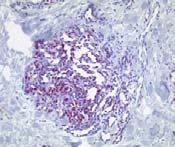

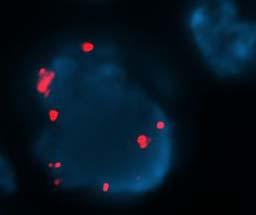
48 BLAP: MYC negative AVL: MYC negative AS: MYC positive AS: MYC positive 47


49 Angiolipoma Benign Mimics of AS Diffuse dermal angioendotheliomatosis Angiolipoma Common in superficial soft tissues of extremities and in breast May be multiple and painful Well-circumscribed with variable amount of fat; little if any fat in cellular angiolipoma Fibrin microthrombi Absent endothelial atypia 48
50 49



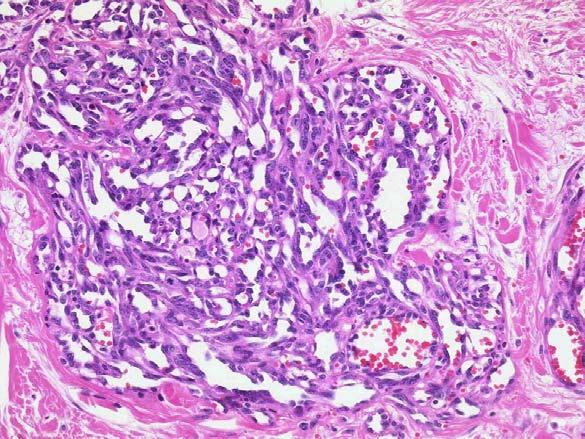
51 Diffuse Dermal Angioendotheliomatosis Typically limited to skin Reactive, secondary to underlying peripheral vascular disease, calciphylaxis, croglobulinemeia, others Exuberant dermal/subcutaneous capillary proliferation, often with infiltrative pattern Absent endothelial atypia Retained pericyte layer around vessels 50



52 CD31 51
 Differential diagnosis of ALN Dedifferentiated liposarcoma ALN/WDL Nomenclature")
 malignancy")
53 Well-differentiated Adipocytic Neoplasms Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN Overview Approach to the diagnosis of atypical lipomatous neoplasms/ well differentiated liposarcomas (ALN/WDL) Differential diagnosis of ALN Dedifferentiated liposarcoma ALN/WDL Nomenclature Pre-1979: All cases diagnosed as WDL (any depth/location) Evans and Kempson: suggested term atypical lipoma for superficial or intramuscular tumors; WDL reserved for retroperitoneal tumors Weiss: proposed retention of WDL for intramuscular tumors Current WHO classification: considers atypical lipomatous neoplasms in any location to be mesenchymal tumors of intermediate (borderline) malignancy Personal recommendation: 1) Use ALN for superficial and intramuscular tumors in extremities; 2) Use WDL for inguinal, paratesticular and retroperitoneal tumors 52




54 ALN/WDL Large, fatty-appearing masses Irregular fibrous septae and mature fat containing enlarged hyperchromatic cells Lipoblasts usually rare or absent Hypercellular blood vessels containing intramural hyperchromatic cells 53



55 Low-grade Variants of ALN/WDL Spindle cell Myxoid Inflammatory Lipoleiomyosarcoma WDL with rhabdomyoblasts Spindle cell WDL Inflammatory WDL Lipoleiomyosarcoma 54


 MDM2")
56 Genetics WDL with rhabdomyoblasts Giant ring and marker chromosomes Amplified sequences from 12q14-15, other parts of 12q, 1q Amplification of MDM2, CDK4, SAS and HMGIC Overexpression of MDM2 and CDK4 may be detected by IHC or FISH/CISH in ALN/WDL and in DL Clinical Behavior Tumor of intermediate malignancy (no metastatic capability) incomplete excision Local recurrence complete excision Cure Tumor progression (dedifferentiation) MDM2 CISH Metastasis 55





57 Differential Diagnosis Fat necrosis/ Lochkern cells Intramuscular lipoma Spindle cell and pleomorphic lipoma Exogenous lipid reaction Hibernoma Angiomyolipoma Massive localized lymphedema Myxoid liposarcoma Mixed-type liposarcoma Fat necrosis and Lochkern cells Fat necrosis May show irregular fibrous septae Adipocyte variability Histiocyte nuclei may be enlarged Lipid-laden histiocytes mimic lipoblasts Lochkern cells Enlarged adipocyte nucleus with intranuclear pseudovacuole, mimicking lipoblasts Usually in thick sections 56



58 Intramuscular Lipoma May be large and infiltrative Atrophic skeletal muscle cells mimic enlarged hyperchromatic cells of ALN Spindle Cell/ Pleomorphic Lipoma Now regarded as ends along the spectrum of a single entity Shoulder/neck region of older men Generally superficial to fascia Admixture of mature fat, myxoid stroma, bland spindled cells, wiry collagen Hyperchromatic, multinucleated cells, floret-like giant cells in PL 57




59 Exogenous Lipid Reaction Silicone and other exogenous materials Numerous pseudolipoblast-like vacuolated histiocytes Foreign body-type giant cells 58





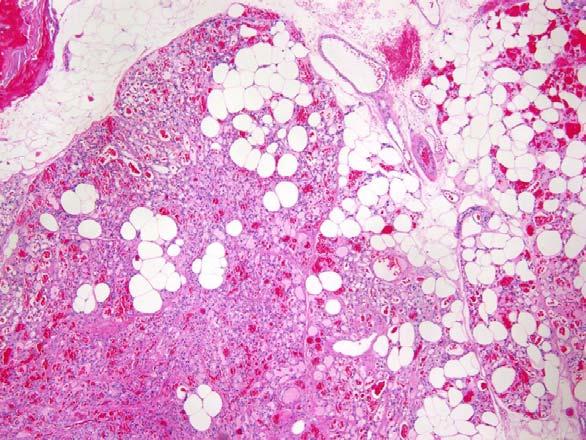
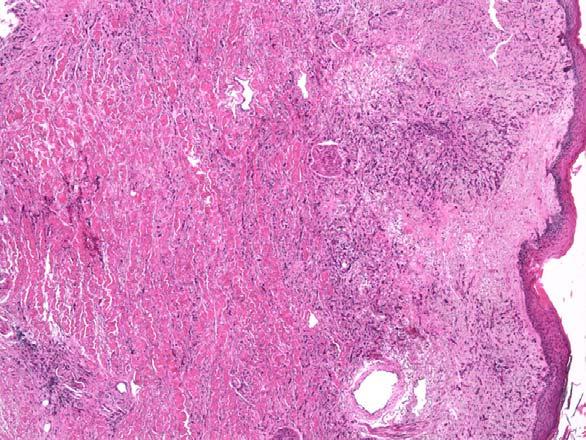
60 Hibernoma Multivacuolated brown fat cells mimic lipoblasts Centrally placed, normochromatic nuclei Important to remember that hibernomatous differentiation may be seen in essentially any fatty tumor, in particular liposarcomas Angiomyolipoma Expansile, non-infiltrative, hemorrhagic masses Triphasic histology Abnormal thick walled vessels Spindled to epithelioid PEC Lipid distended PEC ( adipocytes ) Myomelanocytic immunophenotype Adipocyte -rich variant may mimic WDL Hyperchromatic cells Pseudolipoblasts WDL with brown fat 59




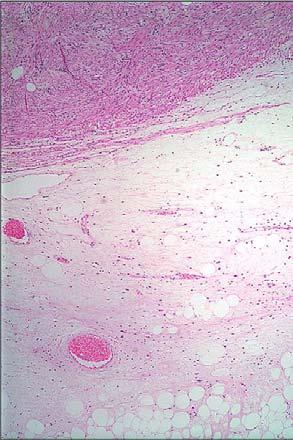
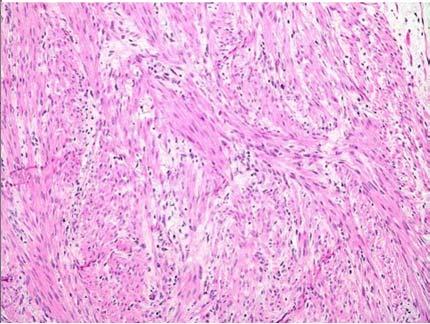
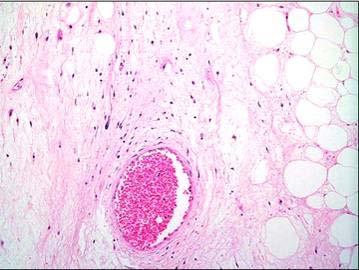
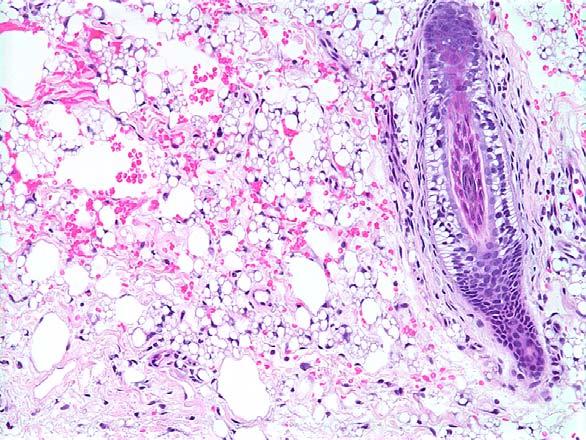
61 Massive localized lymphedema Massively obese patients, usually in the medial thigh Huge, edematous masses Epidermal thickening Expansion of fibrous septae and fibroblastic proliferation Lymphatic proliferation HMB45 60



62 From: Bae, D. K. et al. Arch Dermatol 2008;144:



 (FUS-DDIT3): 95% t (12;22) (q13;q12)")
63 Myxoid and Round Cell LPS Middle aged patients; most common pediatric LPS Most often occur in proximal extremities RCL is now considered a high-grade form of myxoid LPS Pure MLPS are relatively low-grade sarcomas; ~20% risk of distant metastasis even for lesions without round cell component >5% RCL component: high-grade sarcoma with >40% metastases Importance of careful sampling and strict criteria t(12;16) (q13; p11) (FUS-DDIT3): 95% t (12;22) (q13;q12) (EWS-DDIT3): 5% 62


 highgrade, non-lipogenic")



64 Mixed WDL-MLPS Most often reported in the retroperitoneum Shows genetic features of ALN/WDL, but not MLPS MLPS does not occur in the retroperitoneum Represents myxoid ALN/WDL, not MT-LPS Dedifferentiated Liposarcoma Definition: The development of a (usually) highgrade, non-lipogenic sarcoma in the setting of a pre-existing ALN/WDL May be present at initial presentation or following multiple recurrences over many years Most common in retroperitoneal WDL > inguinal/paratesticular WDL >> deep soft tissue of extremities >>> superficial ALN Regarded as time-dependent, rather than sitedependent, phenomenon WDL with myxoid change 63





65 Pathologic Features Grossly visible, solid, non-lipogenic area +/necrosis, within larger fatty mass Usually consist of pleomorphic, undifferentiated sarcoma (MFH-like) Heterologous differentiation may be present May rarely appear histologically low-grade, resembling low-grade fibrosarcoma or fibromatosis Rare variant with meningothelial-like whorls and metaplastic bone High-grade DL Low-grade DL 64






66 Differential Diagnosis Cellular ALN/WDL Some ALN/WDL show increased cellularity and atypia, falling short of clear-cut DL DL should contain at least a 1cm focus of non-lipogenic sarcoma The significance of smaller areas of non-lipogenic sarcoma is uncertain Such cases should be very carefully sampled Non-lipogenic sarcoma infiltrating fat Clear-cut ALN/WDL must be present at least 1 cm away from areas of non-lipogenic sarcoma Pleomorphic liposarcoma Admixture of non-lipogenic sarcoma with pleomorphic lipoblasts DL with perineurial-like whorls 65




67 Sarcoma infiltrating fat Pleomorphic LPS Clinical Behavior DL should be considered high-grade sarcomas Local recurrences in 50%, metastases in 15-20%, 5-year disease-specific mortality of 30% Data suggesting that DL have a better prognosis than other pleomorphic sarcomas are preliminary, and use principally metastases as a clinical endpoint 66

68 That s a lot of giant cells USCAP 2014 Common problems in bone and soft tissue pathology: Giant cell rich lesions Giant cell tumor of bone (GCT) Aneurysmal bone cyst (ABC) Solid aneurysmal bone cyst / giant cell reparative granuloma / brown tumor Chondroblastoma Giant cell rich osteosarcoma Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA A trimodal approach Clinical Radiology Pathology Age Location Clinical Number of lesions Co morbidities Fracture Hyperparathyroidism / renal failure 67



69 Clinical: Age at presentation Clinical: Treatment and prognosis GCT Chondroblastoma ABC GC rich osteosarcoma Recurrence 25% 6-20% <5% N/A Metastasis 2-4% Case reports None* >80% Malignancy <<1% primary Case reports None* 100% Treatment Curettage Denosumab (?) Curettage Curettage Neo-adjuvant chemo, resection Is it intraosseous? Location Compartment Opacity Border Periosteum Radiology Giant cell tumor Chondroblastoma ABC GC rich Osteosarcoma 68





70 Radiology Summary Pathology GCT Chondroblastoma ABC GC rich osteosarcoma Compartment Epiphysis Epiphysis Metaphysis Metaphysis Opacity Purely lytic Lytic + calcifications Purely lytic Lytic + sclerotic Border configuration Circumscribed Marginated, sclerotic rim Marginated, expansile Permeative Denosumab What does this have to do with pathology? Giant cells are not the neoplastic population Pay attention to other components Mononuclear cells Matrix Atypia, pleomorphism Squamous cell carcinoma Roux et al. Am J Clin Pathol 2002;117:




71 Case C: 43 year old woman, proximal fibula mass, undergoes curettage Case C: Giant cell tumor Giant cell tumor Giant cell tumor 70



72 Chondroblastoma Chondroblastoma: GC rich area Chondroblastoma: fibrochondroid matrix Chondroblastoma: chickenwire calcifications 71



73 Chondroblastoma: nuclear grooves Aneurysmal bone cyst Aneurysmal bone cyst: fibrous septae Aneurysmal bone cyst: cells, matrix 72
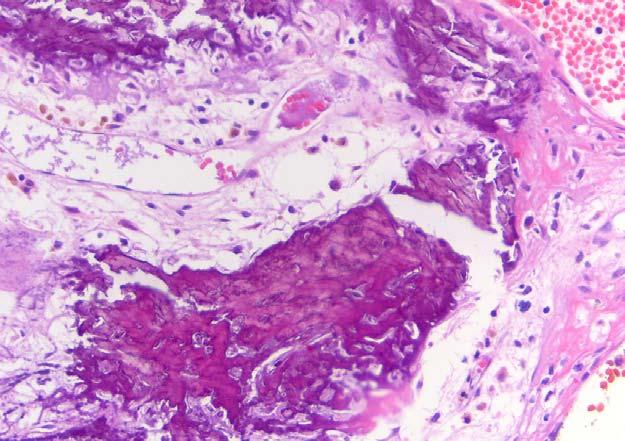
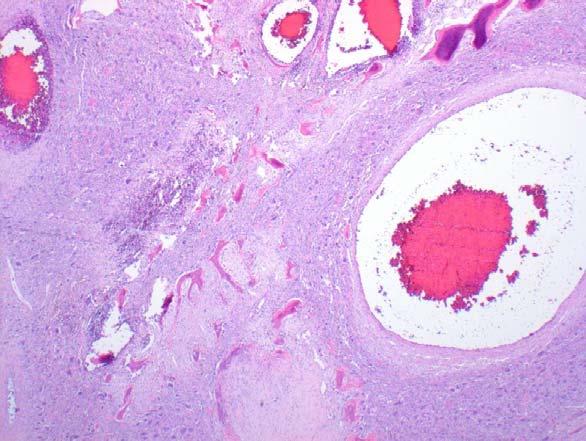






74 Aneurysmal bone cyst: blue bone Solid ABC Brown tumor = solid ABC Giant cell rich osteosarcoma 73




75 Giant cell rich osteosarcoma Giant cell rich osteosarcoma Giant cell rich osteosarcoma Pathology summary GCT Chondroblastoma Matrix Absent Fibrochondroid plaques + calcification Mononuclear cells Ovoid, uniform, nuclei similar to GC Ovoid, eccentric nuclei, grooves ABC Osteoid, Collagen Blue bone Hemosiderin Spindled, fibroblastic/ fibrohistiocytic GC rich osteosarcoma Osteoid Polygonal to spindled, hyperchromatic Mitosis Abundant Rare Variable Abundant, atypical Atypia Absent Absent Absent Marked Distribution of giant cells Uniform Heterogeneous Heterogeneous Heterogeneous 74
 rearrangement Present in conventional and solid ABC Absent in giant cell reparative granuloma of jaw and brown tumor GCT: Histone H3F3A mutations at")



76 Ancillary tests Immunohistochemistry p63: sensitive for giant cell tumor, not specific RunX2, Sox9, Twist: New markers, may become useful Molecular/Genetic ABC: 17p13 (USP6) rearrangement Present in conventional and solid ABC Absent in giant cell reparative granuloma of jaw and brown tumor GCT: Histone H3F3A mutations at Gly34 Chondroblastoma: Histone H3F3B at Lys36 Pitfalls Frozen section, scant material Trimodal approach still applies Exclude osteosarcoma or other malignancy Giant cell rich lesion, no malignancy is acceptable if distinction cannot be made between GCT, ABC and chondroblastoma Treatment will be curettage with follow up Lee et al. Mod Pathol : Dickson et al. Mod Pathol : De la Roza. Archives Path Lab Med :776-9 Horvai et al. Mod Pathol : Panoutsakopoulos G et al. Genes Chrom Ca : Oliveira A et al. Oncogene : Behjati S et al. Nat Genet : Agaram NP et al. Hum pathol : Pitfalls: Giant cell tumor Exceptions to no matrix Cartilage: healing pathological fracture Bone: Capsule, residual cortex, secondary ABC change Malignancy in GCT Benign GCT Necrosis Abundant mitotic activity (>20 mf / 10 hpf) Intravascular invasion Lung metastases in 2 4% Metastases can spontaneously regress 75






77 Case D: 53 year old woman, distal radius bone mass Case D: Malignant giant cell tumor Malignant giant cell tumor Primary malignant GCT Typical GCT mixed with or adjacent to high grade sarcoma Transition gradual, or entire tumor malignant Atypical mitotic figures and atypia in mononuclear cells diagnostic Secondary 10+ year interval after initial diagnosis Radiotherapy Histological types: osteosarcoma, fibrosarcoma Pitfalls: Chondroblastoma Only ~30% of cases demonstrate all characteristic features Fibrochondroid matrix, chicken wire calcifications, nuclear grooves 76
78 Pitfalls: Chondroblastoma unusual sites Temporal bone Talus T2 fat sat Take home messages Pathologic diagnosis of giant cell rich lesions requires careful correlation with radiographic and clinical findings The benign lesions in this category (GCT, ABC, chondroblastoma) are treated similarly, so the most important consideration is to exclude malignancy, especially giant cell rich osteosarcoma RANK RANK L interaction likely mediate the accumulation of giant cells in these lesions, explain their morphologic similarity, and may be a therapeutic target 77
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors
 USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
USCAP 2014 Common problems in bone and soft tissue pathology: Cartilage tumors Andrew Horvai MD PhD Clinical Professor, Pathology UCSF, San Francisco, CA Outline Common intramedullary tumors Enchondroma
Disclosures. Giant Cell Rich Tumors of Bone. Outline. The osteoclast. Giant cell rich tumors 5/21/11
 Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Disclosures Giant Cell Rich Tumors of Bone Andrew Horvai, MD, PhD Associate Clinical Professor, Pathology This lecture discusses "off label" uses of a number of pharmaceutical agents. The speaker is describing
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Grading of Bone Tumors
 Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Grading of Bone Tumors Joon Hyuk Choi, M.D. Department of Pathology College of Medicine, Yeungnam University Introduction to grading system of bone tumor used at Mayo Clinic WHO Histologic Classification
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell
 Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Primary bone tumors > metastases from other sites Primary bone tumors widely range -from benign to malignant. Classified according to the normal cell counterpart and line of differentiation. Among the
Fun with Fat. General Rules. Case
 Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Fun with Fat General Rules Imaging: location (deep vs. superficial) Superficial lesions are seldom liposarcomas Deep lesions may be benign or malignant Myxoid stroma is common in benign and malignant lesions
Update On Lipomatous Tumors: Old Standbys and New Concepts
 Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
The Radiology Assistant : Bone tumor - well-defined osteolytic tumors and tumor-like lesions
 Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - well-defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Introduction to Musculoskeletal Tumors. James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon
 Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
Introduction to Musculoskeletal Tumors James C. Wittig, MD Orthopedic Oncologist Sarcoma Surgeon www.tumorsurgery.org Definitions Primary Bone / Soft tissue tumors Mesenchymally derived tumors (Mesodermal)
MARK D. MURPHEY MD, FACR. Physician-in-Chief, AIRP. Chief, Musculoskeletal Imaging
 ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE MARK D. MURPHEY MD, FACR Physician-in-Chief, AIRP Chief, Musculoskeletal Imaging ALPHABET SOUP AND CYSTIC LESIONS OF THE BONE Giant cell tumor (GCT) Unicameral
Essential Dermatopathology. Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center
 Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Essential Dermatopathology Jinah Kim, MD, PhD Department of Pathology and Dermatology Stanford University Medical Center OBJECTIVES Review clinical, pathologic and molecular aspects of bone and fat tumors
Bone Tumors Clues and Cues
 William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
William Herring, M.D. 2002 Bone Tumors Clues and Cues In Slide Show mode, advance the slides by pressing the spacebar All Photos Retain the Copyright of their Authors Clues by Appearance of Lesion Patterns
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
Bone and Joint Part 2. Leslie G Dodd, MD
 Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Bone and Joint Part 2 Leslie G Dodd, MD Relative rates of cancer Sarcomas are relatively uncommon tumors New cancer cases 2007 All sites 1.4 million prostate 218,890 lung 213,380 breast 180,510 Soft tissue
Bone Tumours - a synopsis. Dr Zena Slim SpR in Histopathology QAH 2009
 Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Bone Tumours - a synopsis Dr Zena Slim SpR in Histopathology QAH 2009 Aims General approach to diagnosis Common entities.and not so common ones. Mini quiz Challenge of bone tumour diagnosis Bone tumours
Mayo Medical Laboratories
 Mayo Medical Laboratories Virtual Lectures 2014 MFMER 2016 MFMER slide-1 Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
Mayo Medical Laboratories Virtual Lectures 2014 MFMER 2016 MFMER slide-1 Virtual Lectures Planning Committee Disclosure Summary As a provider accredited by ACCME, College of Medicine, Mayo Clinic (Mayo
Update on Cutaneous Mesenchymal Tumors. Thomas Brenn
 Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
5/10. Pathology Soft tissue tumors. Farah Bhani. Mohammed Alorjani
 5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
5/10 Pathology Soft tissue tumors Mohammed Alorjani Farah Bhani Slides are included in this sheet. Objectives: Soft tissue tumors 1. Describe soft tissue tumors. 2. Understand the classification of soft
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
The Radiology Assistant : Bone tumor - ill defined osteolytic tumors and tumor-like lesions
 Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
Bone tumor - ill defined osteolytic tumors and tumor-like lesions Henk Jan van der Woude and Robin Smithuis Radiology department of the Onze Lieve Vrouwe Gasthuis, Amsterdam and the Rijnland hospital,
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Musculoskeletal Sarcomas
 Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
Musculoskeletal Sarcomas Robert C. Orth, M.D., Ph.D. Edward B. Singleton Department of Pediatric Radiology Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 9:01:18 AM No disclosures Page 1 xxx00.#####.ppt
APMA 2018 Radiology Track Bone Tumors When to say Gulp!
 APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
APMA 2018 Radiology Track Bone Tumors When to say Gulp! DANIEL P. EVANS, DPM, FACFAOM Professor, Department of Podiatric Medicine and Radiology Dr. Wm. Scholl College of Podiatric Medicine Conflict of
* I have no disclosures or any
 Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
Howard Rosenthal, M.D. Associate Professor of Orthopedic Surgery University of Kansas Sarcoma Center I have no disclosures or any conflicts related to the content of this presentation. Objectives 1. Describe
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Newer soft tissue entities
 Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Tumors of Adipose Tissue Tumors Epidemiology Clinical Features. Morphology. Mature Adipocytes Separated by delicate fibrous septa
 Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
Tumors of Adipose Tissue Lipoma Liposarcoma Most commonly happens in female The most common soft tissue tumor o Originates from matured Adipocytes Most commonly happes at the 4 th and 5 th decade of life
GIANT CELL TUMOR OF BONE
 GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
GIANT CELL TUMOR OF BONE Definition. First described by Jaffe et al. 1, giant cell tumor of bone is a locally aggressive primary neoplasm of bone that is composed of proliferation of bland looking oval
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Adipocytic Tumours in children
 Università degli Studi di Padova Dipartimento di Medicina Sezione di Anatomia Patologica Generale e Citopatologia Adipocytic Tumours in children Rita Alaggio Basel Seminars in Pathology Paediatric Pathology
Università degli Studi di Padova Dipartimento di Medicina Sezione di Anatomia Patologica Generale e Citopatologia Adipocytic Tumours in children Rita Alaggio Basel Seminars in Pathology Paediatric Pathology
Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do?
 Andrew L. Folpe, MD Mayo Clinic, Rochester, MN ISBSTP Handout 2010 Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do? Introduction Over the past several decades
Andrew L. Folpe, MD Mayo Clinic, Rochester, MN ISBSTP Handout 2010 Morphologically Benign Lesions of Soft Tissue and Bone Which Metastasize - What Can We Do? Introduction Over the past several decades
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE
 SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
SOFT TISSUE TUMOR PATHOLOGY: AN UPDATE Jason L. Hornick, MD, PhD July 18, 2013 Department of Pathology Brigham and Women s Hospital Harvard Medical School Boston, MA, USA I have no disclosures. New Soft
Malignant bone tumors. Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7%
 Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
Malignant bone tumors Incidence Myeloma 45% Osteosarcoma 24% Chondrosarcoma 12% Lyphoma 8% Ewing s Sarcoma 7% Commonest primary bone sarcoma is osteosarcoma X ray Questions to ask 1. Solitary or Multiple
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington
 What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
What Do You Need to Know About Bone Pathology? Benjamin L. Hoch M.D. Associate Professor Department of Pathology University of Washington What s Do You Need To Know About Bone Pathology? Reactive/pseudosarcomatous
An Overview of Cutaneous Vascular Neoplasms
 An Overview of Cutaneous Vascular Neoplasms By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School
An Overview of Cutaneous Vascular Neoplasms By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology
 IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
IN THE NAME OF GOD Dr. Kheirandish Oral and maxillofacial pathology ORAL FOCAL MUCINOSIS Uncommon Tumorlike Cutaneous myxoid cyst Overproduction of hyaluronic acid by firoblasts Young adults Female Gingiva
CASE REPORT PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE.
 PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE. M. Madan 1, K. Nischal 2, Sharan Basavaraj. C. J 3. HOW TO CITE THIS ARTICLE: M. Madan, K. Nischal,
PLEOMORPHIC LIPOSARCOMA OF PECTORALIS MAJOR MUSCLE IN ELDERLY MAN- CASE REPORT & REVIEW OF LITERATURE. M. Madan 1, K. Nischal 2, Sharan Basavaraj. C. J 3. HOW TO CITE THIS ARTICLE: M. Madan, K. Nischal,
WHAT IS MDM2? (MDMTWOMICS) MDM2 IN SARCOMAS? (MDMTWOMAS) MDM2MICS? NO CONFLICT OF INTERESTS 5/07/2018 MDM2 IN SOFT TISSUE AND BONE SARCOMAS
 MDM2 IN SARCOMAS? (MDMTWOMAS) MDM2MICS? NO CONFLICT OF INTERESTS 5/07/2018 MDM2 IN SOFT TISSUE AND BONE SARCOMAS") IN SOFT TISSUE AND BONE SARCOMAS WHAT IS? (MDMTWOMICS) Raf Sciot, M.D., PhD. Department of Pathology, University Hospitals Katholieke Universiteit Leuven, LEUVEN, Belgium IN SARCOMAS? (MDMTWOMAS) MICS?
IN SOFT TISSUE AND BONE SARCOMAS WHAT IS? (MDMTWOMICS) Raf Sciot, M.D., PhD. Department of Pathology, University Hospitals Katholieke Universiteit Leuven, LEUVEN, Belgium IN SARCOMAS? (MDMTWOMAS) MICS?
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Typical skeletal location and differential diagnosis of bone tumors.
 Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Typical skeletal location and differential diagnosis of bone tumors. Poster No.: C-2418 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Barros, L. A. Ferreira, Y. Costa, P. J. V. Coelho, F. Caseiro
Bread and Butter Bone Pathology
 Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Bread and Butter Bone Pathology NICOLE D. RIDDLE, MD RUFFOLO, HOOPER, AND ASSOC. / UNIVERSITY OF SOUTH FLORIDA Goals: Fundamentals of neoplastic bone pathology Bone Producing Cartilage Producing Miscellaneous
Klinisch belang van chromosomale translocatie detectie in sarcomen
 Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
LAC + USC.
 Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Jeff McDavit,, M.D. LAC + USC mcdavit@usc.edu Clinical History 55 year old male with large, deep, non- tender left thigh mass. Seen at LAC+USC Med Ctr FNA clinic No h/o trauma or radiation Vimentin
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Abid Irshad, MD Director Breast Imaging. Medical University of South Carolina Charleston
 Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Abid Irshad, MD Director Breast Imaging Medical University of South Carolina Charleston Cases Financial disclosure: I or my family have no financial interest related to the material discussed in this presentation
Case Presentations 17-20
 Case Presentations 17-20 Case Presentations 17 Case 17 2 year old boy with history of urinary retention and prostate biopsy. After biopsy and chemotherapy, child regains urine flow but the mass does not
Case Presentations 17-20 Case Presentations 17 Case 17 2 year old boy with history of urinary retention and prostate biopsy. After biopsy and chemotherapy, child regains urine flow but the mass does not
Bone/Osteoid Producing Lesions
 Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
Chapter 2 Bone/Osteoid Producing Lesions Introduction There are many lesions that are associated with reactive new bone formation; this chapter predominantly covers those in which deposition of osteoid/bone
Molecular pathology in soft tissue tumors. Sylvia Höller Pathologie
 Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Malignant Bone Tumours. PathoBasic, Daniel Baumhoer
 Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
Malignant Bone Tumours PathoBasic, 20.03.18 Daniel Baumhoer FNCLCC Grading The differentiation score is defined as the extent to which a tumor resembles adult mesenchymal tissue (score 1), the extent to
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
COPYRIGHT 2004 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
 84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
84 COPYRIGHT 2004 BY THE JOURNAL BONE AND JOINT SURGERY, INCORPORATED Radiographic Evaluation of Pathological Bone Lesions: Current Spectrum of Disease and Approach to Diagnosis BY BENJAMIN G. DOMB, MD,
Part 1. Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013
 Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Part 1 Slides 1-38, Rita Alaggio Soft tissue tumors Trondheim 14. mars 2013 Pediatric Pathology Soft Tissue Tumors AN UPDATE Rita Alaggio Azienda Ospedaliera Università di Padova Soft Tissue Tumors More
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology
 David M. Parham, MD Chief of Anatomic Pathology") Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Rhabdomyomas and Rhabdomyosarcomas (RMS) David M. Parham, MD Chief of Anatomic Pathology Tumors of skeletal muscle: Rhabdomyomas and rhabdomyosarcomas Embryonal muscle 2 3 4 5 6 7 8 Rhabdomyoma Benign
Contents Part I Introduction 1 General Description 2 Natural History: Importance of Size, Site, Histopathology
 Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
Fluid-fluid levels in bone tumors: A pictorial review
 Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
Fluid-fluid levels in bone tumors: A pictorial review Poster No.: C-578 Congress: ECR 2009 Type: Educational Exhibit Topic: Musculoskeletal Authors: L. Figueroa Nasra, C. Martín Hervás, M. Tapia-Viñé,
INDEX. in this web service Cambridge University Press
 actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
actin 14 adamantinoma 202, 290 292, 297 adenocarcinoma 136 adipocytes in hibernoma 149, 150 in lipoblastoma 148 in lipoma 141, 142, 145 in liposarcoma 152 in myelolipoma 151 adrenal gland tumors see myelolipoma
Normal endometrium: A, proliferative. B, secretory.
 Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Normal endometrium: A, proliferative. B, secretory. Nội mạc tử cung Nội mạc tử cung Cyclic changes in endometrium.. Approximate relationship of useful microscopic changes. Arias-Stella reaction in endometrial
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
The Impact of Advances in Molecular Genetic Pathology on the. Classification, Diagnosis and Treatment of Selected Soft Tissue
 The Impact of Advances in Molecular Genetic Pathology on the Classification, Diagnosis and Treatment of Selected Soft Tissue Tumors of the Head and Neck Joaquín J. García MD and Andrew L. Folpe MD Department
The Impact of Advances in Molecular Genetic Pathology on the Classification, Diagnosis and Treatment of Selected Soft Tissue Tumors of the Head and Neck Joaquín J. García MD and Andrew L. Folpe MD Department
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE
 ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
ORTHOPAEDIC ONCOLOGY OITE REVIEW COURSE Richard D. Lackman, MD FACS Director, Orthopaedic Oncology Center Cancer Institute Introduction In the evaluation of a patient with a bone tumor, there are several
Bone tumors. RMG: jan
 Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
Bone tumors RMG: jan 217. @Kijohs KIZZA JOHN KIJOHS Diseases arising in bone Lipoma Fibrous cortical defects Non-ossifying fibroma Bone island Benign simple cysts Enchondroma Osteochondroma Osteoid osteoma
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
An Overview of Genital Stromal Tumors
 An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
An Overview of Genital Stromal Tumors By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel School of Medicine
CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. CYSTIC NEPHROMA
 Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
Page 1 CYSTIC TUMORS OF THE KIDNEY JOHN N. EBLE, M.D. Department of Pathology & Laboratory Medicine Phone (317) 274-4806 Medical Science A-128 FAX: (317) 278-2018 635 Barnhill Drive jeble @iupui.edu Indianapolis,
University Journal of Surgery and Surgical Specialities
 University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 EXTRA SKELETAL MESENCHYMAL CHONDROSARCOMA :A CASE REPORT Rajaraman R Subbiah S Navin Naushad Kilpaulk Medical College Abstract:
University Journal of Surgery and Surgical Specialities Volume 1 Issue 1 2015 EXTRA SKELETAL MESENCHYMAL CHONDROSARCOMA :A CASE REPORT Rajaraman R Subbiah S Navin Naushad Kilpaulk Medical College Abstract:
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples
 Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Primary bone tumors according to the WHO classification: a review of 13 years with illustrative examples Poster No.: C-1741 Congress: ECR 2015 Type: Educational Exhibit Authors: J. Silva, M. A. Ramírez
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
ISSN: DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY
 : 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
: 289-295 ISSN: 2277 4998 DISTRIBUTION OF BONE AND CARTILAGINOUS TUMORS IN PEDIATRIC AGE GROUP IN WESTERN UTTAR-PRADESH: AN EVALUATIVE STUDY QADRI S, HASAN M, AKHTAR K * AND SHERWANI RK The Departments
Case 1 10/2/17. Myxoid Soft Tissue Tumors & Tumor-like Lesions. Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About
 Myxoid Soft Tissue Tumors & Tumor-like Lesions Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (4:15-5:00pm, Saturday, 23-09-17) Heterogenous
Myxoid Soft Tissue Tumors & Tumor-like Lesions Myxofibro- or Fibromyxo-?: Myxoid Soft Tissue Tumours We Are All Mixed Up About Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (4:15-5:00pm, Saturday, 23-09-17) Heterogenous
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY
 PATHOLOGY CONCEPTS Thursday, October 16, :30am - 11:30am FACULTY COPY") SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
SESSION 1: GENERAL (BASIC) PATHOLOGY CONCEPTS Thursday, October 16, 2008 9:30am - 11:30am FACULTY COPY GOAL: Describe the basic morphologic (structural) changes which occur in various pathologic conditions.
Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is:
 Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is: A. Angiosarcoma B. Haemangiopericytoma C.Myopericytoma D.Myofibroma E. Angioleiomyoma
Case 27 Male 42. Painless, static, well-circumscribed, subcutaneous nodule right lower leg,?lipoma. The best diagnosis is: A. Angiosarcoma B. Haemangiopericytoma C.Myopericytoma D.Myofibroma E. Angioleiomyoma
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Giant cell tumour of the sternum-two cases
 Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
Giant cell tumour of the sternum-two cases Nishaa.P 1, Raghuram.P 2, Navin patil 3, Jaipal B.R 4 Akkamahadevi patel 5 Assistant Professor ESIC medical college and PGIMSR 1 Professor and HOD, 2 Professor
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Primary Breast Liposarcoma
 Primary Breast Liposarcoma Bhagyam Nagarajan 1*, GayatriAutkar 1, Keyuri Patel 1, Meghal Sanghvi 1 1. Department of Radiology, Wockhardt Hospital, Mumbai, India * Correspondence: Dr Bhagyam Nagarajan,
Primary Breast Liposarcoma Bhagyam Nagarajan 1*, GayatriAutkar 1, Keyuri Patel 1, Meghal Sanghvi 1 1. Department of Radiology, Wockhardt Hospital, Mumbai, India * Correspondence: Dr Bhagyam Nagarajan,
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Bone, soft tissue and skin tumors. By: Shefaa qa qa
 Bone, soft tissue and skin tumors By: Shefaa qa qa Bone tumors Most bone neoplasms develop during the first several decades of life and have a propensity for the long bones of the extremities. The occurrence
Bone, soft tissue and skin tumors By: Shefaa qa qa Bone tumors Most bone neoplasms develop during the first several decades of life and have a propensity for the long bones of the extremities. The occurrence
The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone
 The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone Cristina Antonescu, MD Memorial Sloan-Kettering Cancer Center, New York Nothing to declare Disclosure Spectrum of Myoepithelial
The Genetics of Myoepithelial Tumors: salivary glands, soft tissue and bone Cristina Antonescu, MD Memorial Sloan-Kettering Cancer Center, New York Nothing to declare Disclosure Spectrum of Myoepithelial
Acta Medica Okayama. Malignant fibrous histiocytoma with skeletal involvement. Hideo Takechi Kohji Taguchi OCTOBER 1978
 Acta Medica Okayama Volume 32, Issue 5 1978 Article 4 OCTOBER 1978 Malignant fibrous histiocytoma with skeletal involvement Hideo Takechi Kohji Taguchi Okayama University, Okayama University, Copyright
Acta Medica Okayama Volume 32, Issue 5 1978 Article 4 OCTOBER 1978 Malignant fibrous histiocytoma with skeletal involvement Hideo Takechi Kohji Taguchi Okayama University, Okayama University, Copyright
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features