Perioperative use of high oxygen concentration
|
|
|
- Emery Watson
- 5 years ago
- Views:
Transcription



1 Perioperative use of high oxygen concentration F. Javier Belda MD, PhD, Professor of Anesthesiology Head of Department of Anesthesia and Critical Care Hospital Clinico Universitario, University of Valencia, Valencia (Spain)
")

2 Conflicts of interest: Valencia (Spain May 2007) February 2015 Anesthesiology 2014;120: JAMA. 2005;294:
3 Hyperoxia induced lung injury (HILI) Impairment of innate inmune response - Reduced phagocytosys AM - Decreased production of inflammatory mediators - Impaired bacterial killing. Edema, proliferation of type II and destruction of type I alveolar epithelial cells, hyaline membrane formation, interstitial fibrosis... Altemeier WA. Hyperoxia in the intensive care unit: why more is not always better. Curr Opin Crit Care 2007;13:73 78.
4 Hyperoxia induced lung injury (HILI) Impairment of innate inmune response - Reduced phagocytosys AM - Decreased production of inflammatory mediators - Impaired bacterial killing. Edema, proliferation of type II and destruction of type I alveolar epithelial cells, hyaline membrane formation, interstitial fibrosis... Rats and rabits Altemeier Spontaneous WA. Hyperoxia breathing, the intensive injurious care unit: ventilation why more is not always better. Curr Opin Lethal Crit Care experiences 2007;13: Exposure to 100%O2 for several days Subletal injury: 4 days O2 + 4 days Room Air
5 Hiperoxia in healthy humans Clinical hyperoxia in normal lungs FiO2: % Exposure: hours Studies: clinical cases, volonteers, divers... Clark, J. M. and Lambertsen, C. J. (1970). Pulmonary Oxygen Tolerance in Man and Derivation of Pulmonary Oxygen Tolerance Curves. IFEM Report No Symptoms of O2 toxicity in normal lungs 100% O2 12 h 80% O2 24 h 60% O2 36 h < 50% O2 seems completely safe

6 Atelectasis in Anaesthesia Pulmonary Atelectasis. A Pathogenic Perioperative Entity M. Duggan, BP Kavanagh. Anesthesiology 2005;102: Compresion Gas resorption Impaired surfactant



7 Atelectasis in Anaesthesia Pulmonary Atelectasis. A Pathogenic Perioperative Entity M. Duggan, BP Kavanagh. Anesthesiology 2005;102: Compresion Gas resorption Impaired surfactant

8 Atelectasis in anesthesia Optimal O2-concentration during induction of general anesthesia. Edmark, Anesthesiology 2003 Atelectasis FiO2 5,6% 100% 0,6% 80% 0,2% 60%

 Comparable atelectasis")

 6 4 2 0 30 80")
9 Atelectasis in the postoperative period Incidence: 85% 1st PO day (Lindberg, Acta Anaesth Scand 1992) Comparable atelectasis during and 2-h after colon resection Akca, Anesthesiology A t e l e c t a s i Atelectasis (%) FiO2 F i O 2 (%)



10 Supplemental O2 required for SpO2> 90% in PACU Scheduled adults yr; general endotracheal anesthesia, Expected hospital stay >24 h postoperatively. Exclusion criteria: major (open) abdominal, spine, or craniotomy; prone position Preoperative SpO2<90% OSA.

11 45 min PACU 1 day PO 45 min PACU 1 day PO
12 45 min PACU 1 day PO This suggests that absorption atelectasis induced by FiO2 is not sufficient to induce postoperative hypoxemia beyond that associated with anesthesia/surgery induced atelectasis. 45 min PACU 1 day PO Our results suggest that it is reasonable to use high inspired oxygen in surgical patients.


13 Oxygen-dependent microbial killing by phagocytes Babior, N Engl J Med 1978 Roos, Science 2002 Oxygen Oxidative killing is a function of tissue oxygen partial pressure.
14 Subcutaneous Oxygen Tension (n=30) P s q O 2 ( m m H g ) % F i O % F i O I n t r a - o p P o s t - o p T i m e ( h ) Greif 2000

15 Human blood samples incubated at 21 or 80% O2 following a 1 ng/ml lipopolysaccharide challenge Neutrophil phagocytosis intracellular killing mediator of host defense
16 Human blood samples incubated at 21 or 80% O2 following a 1 ng/ml lipopolysaccharide challenge Neutrophil phagocytosis intracellular killing mediator of host defense
17 Human blood samples incubated at 21 or 80% O2 following a 1 ng/ml lipopolysaccharide challenge Neutrophil phagocytosis intracellular killing mediator of host defense Hyperoxia exerts significant effects on multiple cellular and immunologic parameters, providing a potential mechanism for benefits from the use of supplemental oxygen.



18 Nature 2003,17: A single protein allows certain immune cells both to respond to low oxygen 10 levels de Marzo de and 2015 to induce inflammation

19 Belda FJ and the Spanish RETIQ group. JAMA 2005 Multicenter, prospective, randomized, double blind 300 patients, colorectal surgery 2 groups: 30% or 80% O2 in air, during OP + 4 h. post-op Infection rate: 24% The risk of SSI was reduced 54% in patients with 80% oxygen (RR: 0.46; 95% CI: ; P =.04)
20 Meyhoff et al.


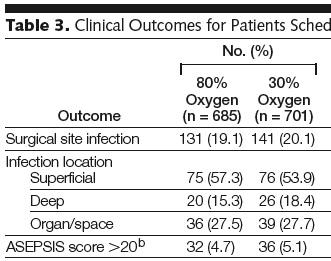
21 Meyhoff et al.
22 SEVEN Meta-analysis Chura et al. Surgical site infections and supplemental perioperative oxygen in colorectal surgery patients: a systematic review.surg Infect 2007; 8: 455 Brar MS et al. Perioperative supplemental oxygen in colorectal patients: a meta-analysis. J Surg Res 2009; 166: 227 Al-Niaimi A, Safdar N. Supplemental perioperative oxygen for reducing surgical site infection: a meta-analysis. J Eval Clin Pract 2009;15:360 Qadan M et al. Perioperative supplemental oxygen therapy and surgical site infection: a meta-analysis of randomized controlled trials. Arch Surg 2009;144:359 Togioka B et al. The role of perioperative high inspired oxygen therapy in reducing surgical site infection: a meta-analysis. Anesth Analg 2012;114:334 Kao LS et al. Should perioperative supplemental oxygen be routinely recommended for surgery patients? A Bayesian meta-analysis. Ann Surg 2012;256:894
23 Bayesian methods directly assess the probability of benefit Probability of reduction in SSIs Any reduction: Probability 77% to 85% Reduction of 10% Probability 57% to 68% Reduction of 20% : Probability 31% to 41%. Colorectal surgery Any reduction: Probability 86% to 92%, Ann Surg 2012;256:


24 Anesthesiology 2013;119:
25 Included all surgeries. Colorectal, appendectomy, abdominal, major abdominal, and gynecologic inclusive breast any except cardiac or one-lung
26 Included colorectal surgery only
27 Included colorectal surgery only What This Article Tells Us That Is New Intraoperative high inspired oxygen fraction decreases the risk of surgical site infection in surgical patients receiving prophylactic antibiotics and does not increase the risk of postoperative atelectasis.


28
 Fixed effects ES (95% CI) % Weight 0.61 (0.38, 0.98) 12.37 0.41 (0.16, 1.03) 5.25 0.46 (0.25, 0.88) 9.08 0.67 (0.13, 3.55) 1.96 0.95 (0.77, 1.18) 19.88 0.74 (0.56, 0.98) 17.89 2.22 (1.08, 4.")
29 Study Belda 2005 Bickel 2011 Greif 2000 Mayzler 2005 Meyhoff 2009 Myles 2007 Pryor 2004 Schietroma 2011 Thibon 2012 Schietroma 2012 Random effects (I-squared = 52.5%, p = 0.025) Fixed effects ES (95% CI) % Weight 0.61 (0.38, 0.98) (0.16, 1.03) (0.25, 0.88) (0.13, 3.55) (0.77, 1.18) (0.56, 0.98) (1.08, 4.58) (0.20, 1.39) (0.46, 1.84) (0.40, 0.98) (0.59, 0.95) 0.80 (0.69, 0.91) Belda FJ, Catala F 2015 Unpublished data


30 J Trauma Acute Care Surg. 2013;75: FiO2 80% during the perioperative period is safe and shows a trend toward reduction of surgical site infection


31 PeerJ 2:e613; DOI /peerj.613 October 2014
32
33

34

35
 O2 30%: 128 /701 (18.3%) Hazard Ratio: 1.30 (1.03-1.64) P =0.03 Cancer surgery: HR: 1.45 (1.10-1.90) P = 0.009 Noncancer surgery: HR: 1.06 (0.69-1.65) P = 0.")
36 Follow-up study of the PROXI trial 1382 patients median follow-up of 2.3 years (range 1.3 to 3.4 years). At follow up: Deaths over the period O2 80%: 159/685 (23.2%) O2 30%: 128 /701 (18.3%) Hazard Ratio: 1.30 ( ) P =0.03 Cancer surgery: HR: 1.45 ( ) P = Noncancer surgery: HR: 1.06 ( ) P = 0.79
37 In animals. In healthy humans. Summary of cons
38 In animals. In healthy humans. Summary of cons
39 In animals. In healthy humans. Apart from its effects on the lungs, oxygen may also lead to systemic toxicity. NO REFERENCE It has been associated with an increase in vascular resistance and a decrease in cardiac output Lodato RF: Decreased O2 consumption and cardiac output during normobaric hyperoxia in conscious dogs. J Appl Physiol 1989, 67:
40 Mortality De Jonge CC 2008
41 Mortality PaO2 (n patients) OR 95%CI <65 (6937) 1,2 1,03-1, Reference (7466) (6430) 1,11 1,02-1, (7278) 1,08 1,00-1,18 >110 (8196) 1,23 1,13-1,34 Indicating severity It is possible that physicians recognised some marker of severity and purposefully gave higher concentrations of oxygen to achieve higher levels of PaO2 in these high-risk patients. De Jonge CC 2008
42 Although oxygen toxicity is a well known entity Mao C et al. A quantitative assessment of how Canadian intensivists believe they utilize oxygen in the intensive care unit. Crit Care Med 1999,27: it appears that physicians are more concerned about avoiding hypoxia and ischaemia than about the risks of hyperoxia. Prospective, controlled trials are necessary to show a causal relationship between high FiO2 and mortality. De Jonge CC 2008
43 Hyperoxia after nontraumatic cardiac arrest Kilgannon JH et al. Emergency Medicine Shock Research Network (EMShockNet) Investigators: Association between arterial hyperoxia following resuscitation from cardiac arrest and inhospital mortality. JAMA 2010,303: ,326 USA patients after nontraumatic cardiac arrest Bellomo R et al. Study of Oxygen in Criticial Care Group. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit Care 2011, 15:R90. 12,108 AUS patients after nontraumatic cardiac arrest Hyperoxia higher mortality: OR
44 Bellomo R et al. Crit Care 2011, 15:R90.

45 Bellomo R et al. Crit Care 2011, 15:R90. Covariates: Apache without O2 component Treatment limitation on admission Lowest glucose 24 h Hospital characteristics Hyperoxia was not independently associated with mortality
46 Bellomo R et al. Crit Care 2011, 15:R90. Our findings are against policies of deliberate decreases in FiO2 unless accurate and reliable SpO2 monitoring is available. Crit Care Med 2013; 41:


47 Crit Care Med 2013; 41: Perioperative care 2.Critical care 3.Resuscitation.
48 Human response to hypobaric hypoxia (high altitude) is well described and characterized by the restoration of convective oxygen delivery through increases in alveolar ventilation, cardiac output, and red blood cell mass. It is unlikely that critically ill patients mount such effective cardiorespiratory countermeasures to increase oxygen delivery as a result of their underlying pathology

49 Clinical studies of ARDS concluded that P/F ratio was not a reliable predictor of outcome
50 Permissive hypoxemia Implementation of PH is more speculative (and potentially harmful) and evaluation of the safety and feasibility of this approach in perioperative and critical care settings is needed before clinical trials are contemplated.
51 Can we optimize long-term outcomes in acute respiratory distress syndrome by targeting normoxemia? Mikkelsen ME et al. Ann Am Thorac Soc, 2014 Mar 12. [Epub ahead of print] The association between lower oxygenation values and long-term cognitive impairment is observed in 25% of ARDS survivors Am J RCCM 2012;185: PLoS One 2011;6(7):e22512 BMJ 2013;346;f1532

52 Can we optimize long-term outcomes in acute respiratory distress syndrome by targeting normoxemia? Mikkelsen ME et al. Ann Am Thorac Soc, 2014 Mar 12. [Epub ahead of print] It seems plausible that raising the target range for PaO2 to mm Hg and SpO % may reduce the risk of long-term cognitive impairment in ARDS survivors
53 Conclussions: Perioperative hyperoxia Does not increase the risk of postoperative atelectasis. Does not induce postoperative hypoxemia Reduce the risk of SSI and maybe infections No demonstrated long-term mortality No real toxicity demonstrated in critical patients Permisive hypoxemia seems a dangerous concept

54 THANK YOU VERY MUCH FOR YOUR ATTENTION
Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB
 Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB Mortality and morbidity in acutely ill adults treated with liberal vs. conservative oxygen therapy: systematic review and meta-analysis
Canadian Society of Internal Medicine Annual Meeting 2018 Banff, AB Mortality and morbidity in acutely ill adults treated with liberal vs. conservative oxygen therapy: systematic review and meta-analysis
Current oxygen management in mechanically ventilated patients: A prospective observational cohort study
 Journal of Critical Care (2013) 28, 647 654 Ventilation Current oxygen management in mechanically ventilated patients: A prospective observational cohort study Satoshi Suzuki MD, PhD a, Glenn M. Eastwood
Journal of Critical Care (2013) 28, 647 654 Ventilation Current oxygen management in mechanically ventilated patients: A prospective observational cohort study Satoshi Suzuki MD, PhD a, Glenn M. Eastwood
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley
 Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Contraindications to time critical surgery; when not to proceed from the perspective of: The Physician A/Prof Peter Morley British Journal of Surgery 2013; 100: 1045 1049 The risk of 30 day mortality
Oxygen:..Nothing is without poison.. the poison is in the dose..
 Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
No Excellence Without Evidence: The Therapeutic Use of Oxygen
 No Excellence Without Evidence: The Therapeutic Use of Oxygen Penelope S. Benedik PhD, CRNA, RRT Associate Professor of Clinical Nursing UTHealth Houston, Texas Oxygen is a DRUG Oxygen overuse is toxic
No Excellence Without Evidence: The Therapeutic Use of Oxygen Penelope S. Benedik PhD, CRNA, RRT Associate Professor of Clinical Nursing UTHealth Houston, Texas Oxygen is a DRUG Oxygen overuse is toxic
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Post Arrest Ventilation/Oxygenation Management
 Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Post Arrest Ventilation/Oxygenation Management Richard Branson MSc RRT Professor of Surgery University of Cincinnati Editor-In-Chief Respiratory Care 0 Presenter Disclosure Information Richard Branson
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Mechanical Ventilation Strategies in Anesthesia
 Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
PA Catheters - Useful or Not
 PA Catheters - Useful or Not Perioperative in Liver Transplantation ILTS/ASA, San Francisco, 2003 Claus U. Niemann, MD Department of Anesthesia and Perioperative Division of Liver Transplantation University
PA Catheters - Useful or Not Perioperative in Liver Transplantation ILTS/ASA, San Francisco, 2003 Claus U. Niemann, MD Department of Anesthesia and Perioperative Division of Liver Transplantation University
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 THE EVIDENCE BASIS REGARDING POSTOPERATIVE PULMONARY COMPLICATIONS
 EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 THE EVIDENCE BASIS REGARDING POSTOPERATIVE PULMONARY COMPLICATIONS 05RC1 JAUME CANET, VALENTÍN MAZO, ZAHARA BRIONES Department of Anaesthesiology
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 THE EVIDENCE BASIS REGARDING POSTOPERATIVE PULMONARY COMPLICATIONS 05RC1 JAUME CANET, VALENTÍN MAZO, ZAHARA BRIONES Department of Anaesthesiology
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
The effects of high perioperative inspiratory oxygen fraction for adult surgical patients (Review)
") The effects of high perioperative inspiratory oxygen fraction for adult surgical patients (Review) Wetterslev J, Meyhoff CS, Jørgensen LN, Gluud C, Lindschou J, Rasmussen LS This is a reprint of a Cochrane
The effects of high perioperative inspiratory oxygen fraction for adult surgical patients (Review) Wetterslev J, Meyhoff CS, Jørgensen LN, Gluud C, Lindschou J, Rasmussen LS This is a reprint of a Cochrane
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view
 Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Senior Visceral Surgery Fast-Track in Colorectal Surgery The anesthetist s point of view 1st Geneva International SCIENTIFIC DAY February 3 rd 2010 E. Schiffer Dept APSI, HUG 1 Fast-Track in colorectal
Management of Post Cardiac Arrest Syndrome
 Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
Management of Post Cardiac Arrest Syndrome Wilhelm Behringer Associated Professor of Emergency Medicine Medical University of Vienna, Austria Patients % What happens after ROSC? 35 30 25 20 15 10 5 ROSC
PREVENT COMPLICATIONS IN MAJOR SURGERY
 PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
PREVENT COMPLICATIONS IN MAJOR SURGERY Dept of Anesthesia and ICM (Prof. G. Della Rocca) Azienda Ospedaliero-Universitaria University of Udine. Udine, Italy CLINICAL TRIAL OF SURVIVORS CARDIORESPIRATORY
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital
 Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Show Me the Evidence: Epidurals, PVBs, TAP Blocks Christopher L. Wu, MD Professor of Anesthesiology The Johns Hopkins Hospital Overview Review overall (ERAS and non-eras) data for EA, PVB, TAP Examine
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Methods ROLE OF OPEN LUNG BIOPSY IN PATIENTS WITH DIFFUSE LUNG INFILTRATES AND ACUTE RESPIRATORY FAILURE
 ROLE OF OPEN LUNG BIOPSY IN PATIENTS WITH DIFFUSE LUNG INFILTRATES AND ACUTE RESPIRATORY FAILURE Li-Hui Soh, Chih-Feng Chian, Wen-Lin Su, Horng-Chin Yan, Wann-Cherng Perng, and Chin-Pyng Wu Background
ROLE OF OPEN LUNG BIOPSY IN PATIENTS WITH DIFFUSE LUNG INFILTRATES AND ACUTE RESPIRATORY FAILURE Li-Hui Soh, Chih-Feng Chian, Wen-Lin Su, Horng-Chin Yan, Wann-Cherng Perng, and Chin-Pyng Wu Background
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Thanks to Ben Taylor for his Grand Rounds talk which looks at the problems that may result from whacking on a bit of oxygen.
 EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Hooray for Hypoxia (or don t give too much oxygen)
") Hooray for Hypoxia (or don t give too much oxygen) Geoff Bellingan Medical Director University College London Hospitals British Thoracic Society Guideline for emergency oxygen use in adult patients Endorsed
Hooray for Hypoxia (or don t give too much oxygen) Geoff Bellingan Medical Director University College London Hospitals British Thoracic Society Guideline for emergency oxygen use in adult patients Endorsed
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES
 EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
EMERGING EVIDENCE AND BEST PRACTICES TO PREVENT SSI IN COLON PROCEDURES Clifford Ko, MD, MS, MSHS, FACS, FASCRS Professor of Surgery UCLA Director, ACS NSQIP, American College of Surgeons EVIDENCE Ban
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Disclosures. Objectives. OSA Death and Near Miss Registry The path to creation.
 OSA Death and Near Miss Registry The path to creation. October 23, 2015 Norman Bolden, M.D. Vice-Chairman, Department of Anesthesiology Associate Professor, Case Western Reserve University n None Disclosures
OSA Death and Near Miss Registry The path to creation. October 23, 2015 Norman Bolden, M.D. Vice-Chairman, Department of Anesthesiology Associate Professor, Case Western Reserve University n None Disclosures
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Tracheal Intubation in ICU: Life saving or life threatening?
 Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care
 28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
Preventing Surgical Site Infections: The SSI Bundle
 Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
Preventing Surgical Site Infections: The SSI Bundle 1 Why SSI? New York State 30,000 hospital discharges 1984 3.7% of patients experience serious adverse events related to medical management The top three
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Update on the Prevention of Surgical Site Infections
 Update on the Prevention of Surgical Site Infections Scientific Seminar on Infection Control May 9, 2012 Tom R. Talbot, MD MPH Associate Professor of Medicine and Preventive Medicine Vanderbilt University
Update on the Prevention of Surgical Site Infections Scientific Seminar on Infection Control May 9, 2012 Tom R. Talbot, MD MPH Associate Professor of Medicine and Preventive Medicine Vanderbilt University
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Designing Clinical Trials in Perioperative Sleep Medicine
 Designing Clinical Trials in Perioperative Sleep Medicine A Rationale and Pragmatic Approach Daniel J. Gottlieb, MD, MPH Director, Sleep Disorders Center, VA Boston Healthcare System Program in Sleep and
Designing Clinical Trials in Perioperative Sleep Medicine A Rationale and Pragmatic Approach Daniel J. Gottlieb, MD, MPH Director, Sleep Disorders Center, VA Boston Healthcare System Program in Sleep and
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
PCV and PAOP Old habits die hard!
 PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery
 Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Respiratory Depression and Considerations for Monitoring Following Ophthalmologic Surgery Athir Morad, M.D. Division of Neurocritical care Departments of Anesthesiology/ Critical Care Medicine and Neurology
Preoperative Pulmonary Evaluation. Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine
 Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
Preoperative Pulmonary Evaluation Michelle Zetoony, DO, FCCP, FACOI Board Certified Pulmonary, Critical Care, Sleep and Internal Medicine No disclosures related to this lecture. Objectives Identify pulmonary
TEMPERATURE MANAGEMENT
 TEMPERATURE MANAGEMENT Unintentional Hypothermia and the Maintenance of Normothermia Ian Sampson, M.D. SURGICAL CARE IMPROVEMENT PROJECT Temperature Management SCIP INF 7: Colorectal surgery patients with
TEMPERATURE MANAGEMENT Unintentional Hypothermia and the Maintenance of Normothermia Ian Sampson, M.D. SURGICAL CARE IMPROVEMENT PROJECT Temperature Management SCIP INF 7: Colorectal surgery patients with
Hyperoxemia in Mechanically Ventilated, Critically Ill Subjects: Incidence and Related Factors
 Hyperoxemia in Mechanically Ventilated, Critically Ill Subjects: Incidence and Related Factors Taiga Itagaki MD, Yuuki Nakano, Nao Okuda MD, Masayo Izawa MD, Mutsuo Onodera MD, Hideaki Imanaka MD PhD,
Hyperoxemia in Mechanically Ventilated, Critically Ill Subjects: Incidence and Related Factors Taiga Itagaki MD, Yuuki Nakano, Nao Okuda MD, Masayo Izawa MD, Mutsuo Onodera MD, Hideaki Imanaka MD PhD,
Sleep Labs are Obsolete for Perioperative Assessment of Sleep-Disordered Breathing: Pro
 Sleep Labs are Obsolete for Perioperative Assessment of Sleep-Disordered Breathing: Pro Lawrence J. Epstein, MD Brigham and Women s Hospital Harvard Medical School Welltrinsic Sleep Network Conflicts of
Sleep Labs are Obsolete for Perioperative Assessment of Sleep-Disordered Breathing: Pro Lawrence J. Epstein, MD Brigham and Women s Hospital Harvard Medical School Welltrinsic Sleep Network Conflicts of
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines
 TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Anaesthetic considerations for laparoscopic surgery in canines
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Resuscitation fluids in critical care
 Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Pre-op Clinical Triad - Pulmonary. Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018
 Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
Pre-op Clinical Triad - Pulmonary Sammy Pedram, MD FCCP Assistant Professor of Medicine Pulmonary & Critical Care Medicine March 16, 2018 Disclosures none Case Mr. G is a 64 year-old man who presents to
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Les solutés de remplissage. Philippe Van der Linden MD, PhD
 Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Les solutés de remplissage Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Fluid Resuscitation Morbidity Procedure Co-morbidities
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Buffering a Permissive Hypercapnia The Evidence
 Buffering a Permissive Hypercapnia The Evidence John Laffey Department of Anesthesia, St Michael s Hospital, University of Toronto, CANADA Disclosures Funding European Research Council [FP-7] Health Research
Buffering a Permissive Hypercapnia The Evidence John Laffey Department of Anesthesia, St Michael s Hospital, University of Toronto, CANADA Disclosures Funding European Research Council [FP-7] Health Research
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
Evidence-Based Recommendations for Intraoperative Prevention of SSI. Intraoperative Antiseptic Skin Preparation of the Patient
 Sven Scheffler, MD PhD Sporthopaedicum Berlin, Germany Symposium: Prevention and Management of Infection in ACL Reconstruction General Considerations for Prevention of Infection Intraoperative Precautions
Sven Scheffler, MD PhD Sporthopaedicum Berlin, Germany Symposium: Prevention and Management of Infection in ACL Reconstruction General Considerations for Prevention of Infection Intraoperative Precautions
Anaesthesia for the Over 75s. Chris Edge
 Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
Anaesthesia for the Over 75s Chris Edge Topics to be Covered Post-operative cognitive management Morbidity and mortality General anaesthesia a good idea or not? Multiple comorbidities and assessment of
Supplemental Digital Content 1. Incidence of early nausea: Cumulative incidence 0-6h postoperatively
 Supplemental Digital Content. Incidence of early nausea: Cumulative incidence 0-h postoperatively Piper 0 Purhonen 0 Turan 0 5 2 2 5 34 2 4 4 3 2 0 2 0 2 3 4.2%.%.% 3.% 3.% 4.0% 5.2% 4.% 4.3% M-H, Fixed,
Supplemental Digital Content. Incidence of early nausea: Cumulative incidence 0-h postoperatively Piper 0 Purhonen 0 Turan 0 5 2 2 5 34 2 4 4 3 2 0 2 0 2 3 4.2%.%.% 3.% 3.% 4.0% 5.2% 4.% 4.3% M-H, Fixed,
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial
. A randomized controlled trial") CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
CPAP Reduces Hypoxemia After Cardiac Surgery (CRHACS Trial). A randomized controlled trial Backgrounds Postoperative pulmonary complications are most frequent after cardiac surgery and lead to increased
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
seminaires iris CPR 2015 : how much oxygen? PaO 2 target - routinely > 60 mmhg
 CPR 15 : how much oxygen? Serge Brimioulle PaO 2 target - routinely > 6 mmhg - ALI - ARDS 55-8 mmhg - chronic hypercapnia ~ 5 mmhg - paraquat intoxication ~ 4 mmhg (lactate) Oxygenation O 2 pressure Department
CPR 15 : how much oxygen? Serge Brimioulle PaO 2 target - routinely > 6 mmhg - ALI - ARDS 55-8 mmhg - chronic hypercapnia ~ 5 mmhg - paraquat intoxication ~ 4 mmhg (lactate) Oxygenation O 2 pressure Department
Science Behind CPR Update from Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 Science Behind CPR Update from 2010 Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences FRAMING THE DISCUSSION NO ONE SURVIVES CARDIAC ARREST, EXCEPT ON TV Conflicts of
Science Behind CPR Update from 2010 Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences FRAMING THE DISCUSSION NO ONE SURVIVES CARDIAC ARREST, EXCEPT ON TV Conflicts of
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Is ARDS Important to Recognize?
 Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
PulsioFlex Patient focused flexibility
 PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
PulsioFlex Patient focused flexibility Modular platform with intelligent visualisation for advanced patient Minimally invasive perioperative cardiac output trend with ProAQT Enables calibrated cardiac
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CENTRAL VENOUS OXYGEN SATURATION (SCVO 2 ): INTEREST AND LIMITATIONS
: INTEREST AND LIMITATIONS") EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CENTRAL VENOUS OXYGEN SATURATION (SCVO 2 ): INTEREST AND LIMITATIONS 12RC2 SHAHZAD SHAEFI 1 RUPERT M. PEARSE 2 1 Department of Anesthesia and
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 CENTRAL VENOUS OXYGEN SATURATION (SCVO 2 ): INTEREST AND LIMITATIONS 12RC2 SHAHZAD SHAEFI 1 RUPERT M. PEARSE 2 1 Department of Anesthesia and