LIVER TRAUMA. Jonathan R. Hiatt, MD
|
|
|
- Irma Washington
- 5 years ago
- Views:
Transcription
1 Jonathan R. Hiatt, MD
2
3
4

5

6 HISTORY MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS.
7 EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC STRATEGY NONOPERATIVE OPERATIVE MULTIDISCIPLINARY PORTA HEPATIS INJURY


8



9 INJURY PATTERNS COMMON BLUNT PENETRATING
10 PATIENTS BY MECHANISM HOSPITAL n STAB WD GSW BLUNT HOUSTON DETROIT NEW ORLEANS SAN FRANCISCO
11 MORTALITY BY MECHANISM HOSPITAL STAB WD GSW BLUNT HOUSTON DETROIT NEW ORLEANS SAN FRANCISCO SAN ANTONIO DENVER MOORE, CONTEMP SURG '79
12 INJURY PATTERNS ASSOCIATED INJURIES COMMON AFFECT MORTALITY
13 MALHOTRA, ANN SURG 2000 LIVER TRAUMA ASSOCIATED INJURIES (BLUNT)
14 MORTALITY BY NO. OF INJURIES NO. OF ASSOC. INJURIES n MORTALITY, % 0 (LIVER ONLY) or > 9 67 MIKESKY, SGO 1956
15 MORTALITY (n = 1842) TOTAL / LIVER RELATED RICHARDSON, ANN SURG 2000
16 MORTALITY: CAUSES TIME % < 48 HR. BLEEDING 8.2 > 48 HR. ORGAN FAILURE 2.3 FELICIANO, ANN SURG 1989
17 MORTALITY: RISK FACTORS 20-FOLD INCREASE WITH: BASE DEFICIT < - 6 OPERATIVE BLOOD LOSS > 5 l

18 CLASSIFICATION: AAST ORGAN INJURY SCALE Freq, % MOORE, J TRAUMA 1979 & '94
19 MORTALITY BY INJURY CLASS MORTALITY, % HEPATIC MORTALITY, % III IV V COGBILL, J TRAUMA 1988
20 OPERATIVE PRINCIPLES MOST NONBLEEDING GRADED APPROACH TAILORED TO INJURY MULTIPLE TECHNIQUES




21

22 LIVER TRAUMA
23 NONOPERATION: CURRENT STATUS ATTEMPT IN > 80% SUCCEED IN > 70% (90% OF ATT.) FAILURES: HIGHER INJURY GRADE HEMOPERITONEUM OUTCOME IMPROVED LOS, INFECTION, TRANSFUSION

24 NONOPERATIVE MGMT. J TRAUMA 12
25 NONOPERATIVE MGMT. (Blunt injury) Level 1 1. Urgent laparotomy: Hemodynamically unstable Diffuse peritonitis J TRAUMA 12
26 NONOPERATIVE MGMT. (Blunt injury) Stable w/o peritonitis: 1. No routine laparotomy Level 2 2. Abdominal CT w/ IV contrast 3. Transient responder: Consider angio/embolization as adjunct to operation 4. Grade, hemoperitoneum, neuro status, age>55y, associated injuries are not absolute contraindications 5. Angio/embolization with active contrast blush on CT 6. Environment: Monitoring, serial exams, available OR J TRAUMA 12
27 NONOPERATIVE MGMT. (Blunt injury) Level 2 Stable w/o peritonitis: 1. No routine laparotomy 2. Abdominal CT w/ IV contrast Angiography/embolization: 3. Consider as adjunct to op. for transient responder 5. With active contrast blush on CT 4. Grade, hemoperitoneum, neuro status, age>55y, associated injuries are not absolute contraindications J TRAUMA Environment: Monitoring, serial exams, available OR
28 NONOPERATIVE MGMT. (Blunt injury) Level 3 1. Repeat CT: persistent SIR, pain, jaundice, Hgb drop 2. Interventional modalities incl.ercp, angio, laparoscopy, IR drainage for complications (bile leak, biloma, bile peritonitis, liver abscess, bilious ascites, hemobilia) 3. Pharmacologic VTE prophylaxis can be used w/o increasing failure rate, but timing of safe initiation not determined J TRAUMA 12
29 NONOPERATIVE MGMT. (Blunt injury) Cannot make recommendations 1. Frequency of Hgb measurements 2. Frequency of abdominal exams 3. Intensity and duration of monitoring 4. Time to resuming oral intake 5. Duration/intensity of activity restriction (hospital and DC) 6. Optimal length of ICU and hospital stay 7. Timing of initiation of DVT prophylaxis J TRAUMA 12
30 NONOPERATION: PRINCIPLES MECHANISM BLUNT Tangential penetrating STABLE, EVALUABLE MINIMAL TRANSFUSION ICU MONITORING RESPONSIBLE SURGEON
31 669 pts; nonop 65% BP < 90 10% 23 deaths (5%) LIVER TRAUMA Nonoperation: Morbidity Risk Factors 2 hepatic deaths (MSOF) 87 hepatic complics. in 61 pts. (13%) Kozar, Arch Surg 2006

32 Nonoperation: Morbidity Risk Factors Post-injury day Kozar, Arch Surg 2006
: CNS 7, MOSF 3, hepatic 0 Complications 7(3.")
33 Nonoperation: Morbidity in Children 185 nonop; successful in 90% 10 died (5.4%): CNS 7, MOSF 3, hepatic 0 Complications 7(3.8%) Giss, J Trauma 2006
34 CLASSIFICATION: LIMITATIONS MORBIDITY / MORTALITY related to: PARENCHYMAL DAMAGE INITIAL INJURY OPERATIVE INTERVENTIONS HEPATIC VEINS
35 OPERATIVE APPROACH WIDE PREP LONG MIDLINE INCISION CONTROL HEMORRHAGE MOBILIZE LIVER DIVIDE HEPATIC LIGAMENTS FIXED RETRACTOR
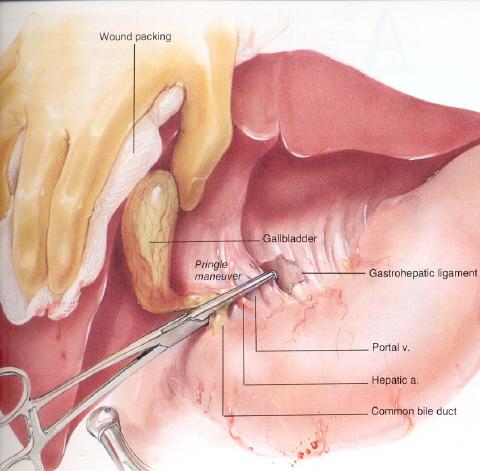

36 INITIAL HEMORRHAGE CONTROL
37 SCORE, ACS Surg

38 PRINGLE OCCLUSION STOPS FORWARD FLOW HEPATIC ARTERIAL PORTAL VENOUS? EXCLUDES HEPATIC VENOUS BLEEDING? DURATION
 (ischemic preconditioning) Richardson,")
39 Portal Occlusion - Elective (Portal triad clamping) (ischemic preconditioning) Richardson, HPB 2012
40 EXTENDED INCISION
41 OPERATIVE APPROACH WIDE PREP LONG MIDLINE INCISION CONTROL HEMORRHAGE MOBILIZE LIVER DIVIDE HEPATIC LIGAMENTS FIXED RETRACTOR


42 FALCIFORM LIGAMENT
43
44 SIMPLE INJURIES (GRADES I-II, OIS) > 70% OF PATIENTS LACERATIONS, CAPSULAR TEARS TECHNIQUES ELECTROCAUTERY, ARGON BEAM HEMOSTATIC AGENTS + CLOSED SUCTION DRAINAGE
45 TOPICAL HEMOSTATIC AGENTS
46 COMPLEX INJURIES (GRADES III-VI, OIS) DIRECT APPROACH HEPATOTOMY / HEPATORRHAPHY RESECTIONAL DEBRIDEMENT RESECTION DAMAGE CONTROL TECHNIQUES

47 HEPATORRHAPHY

48



49 RESECTIONAL DEBRIDEMENT Omental pedicle


50 PARENCHYMAL DIVISION EMERGENT ELECTIVE


51 SUBCAPSULAR HEMATOMA
52 SCORE, ACS Surg


53 STORM LONGMIRE CLAMP PARTIAL HEPATECTOMY

54 SELECTIVE HEPATIC ARTERY LIGATION


55 ABSORBABLE MESH HEPATORRHAPHY
56 HEPATIC VENOUS INJURIES HIGH MORTALITY INTRA- OR EXTRAHEPATIC THERAPEUTIC OPTIONS DIRECT REPAIR VASCULAR ISOLATION ATRIOCAVAL SHUNT DAMAGE CONTROL

57
58 SCORE, ACS Surg

59 YELLIN, ARCH SURG 1971
60 SCORE, ACS Surg


61 RETROHEPATIC INFERIOR VENA CAVA
62 VENOUS INJURIES: MORTALITY (n = 1842) RICHARDSON, ANN SURG 2000
63 VENOUS INJURIES: THERAPY (n = 1842) RICHARDSON, ANN SURG 2000
64 DAMAGE CONTROL: RATIONALE MORTALITY RELATED TO: INTERVENTIONS TIME BLOOD LOSS (6u = failed intervention)
65 DAMAGE CONTROL: INDICATIONS Inability to achieve hemostasis (coagulopathy) Inaccessible major venous injury Time-consuming procedure in patient with suboptimal response to resuscitation Mgmt. of extra-abd. life-threatening injury Reassessment of intra-abdominal contents Inability to close fascia (visceral edema) SHAPIRO, J TRAUMA 2000

66 PERIHEPATIC PACKING DECIDE EARLY VICIOUS CYCLE HYPOTHERMIA ACIDOSIS COAGULOPATHY REOP: when cycle reversed RISK: INFECTION


67 LIVER PACKS

68 SCORE, ACS Surg
69 CT SCAN LIVER INJURY HEMOPERITONEUM OTHER ORGAN INJURIES GUIDES NONOP MGMT.
70 MULTIDISCIPLINARY TECHNIQUES INVASIVE RADIOLOGY ANGIOGRAPHY / EMBOLIZATION CT GUIDED DRAINAGE ERCP LAPAROSCOPY
71 MULTIDISCIPLINARY TECHNIQUES PRIMARY THERAPY ADJUNCTIVE TO OP / NONOP FOR COMPLICATIONS OF OP / NONOP
72 ABDOMINAL COMPLICATIONS VASCULAR BLEEDING INTRA-ABDOMINAL INTRAHEPATIC ANEURYSMS, FISTULAE BILIARY LEAKS, STRICTURES INFECTION / ABSCESS
73 ANGIOEMBOLIZATION INITIAL CT: CONTRAST BLUSH LATE BLEEDING / HEMOBILIA AFTER DAMAGE CONTROL


74 ANGIOEMBOLIZATION Pseudoaneurysm Post - occlusion


75 VENOUS STENTING Disruption of R hepatic vein at IVC Wallstent > DENTON, J TRAUMA 1997
76 HEMOBILIA TRIAD GI bleeding, RUQ pain, jaundice ETIOLOGY Liver injury (incl. iatrogenic) Abscess, aneurysm, tumor (rare) DX / RX: angiography / embolization

77 ERCP DIAGNOSIS OF HEMOBILIA
78 PORTAL TRIAD INJURIES n MORTALITY PORTAL VEIN 42 57% HEPATIC ARTERY 16 56% BILE DUCT 26 19% TOTAL 84 45% MULTIPLE 15 80% JURKOVICH, J TRAUMA 2003
79 PORTAL TRIAD INJURIES JURKOVICH, J TRAUMA 2003



80 EXTRAHEPATIC BILIARY TRACT
81 EXTRAHEPATIC BILE DUCT Carrel patch w/ cystic duct
82 VENOVENOUS BYPASS BIFFL, J TRAUMA 1998

83

84
85 TRANSPLANTATION RINGE ESQUIVEL ANGSTADT n Veins injured Indic.: Bleeding Late necrosis Temporary PC shunt Retransplantation Survived BR J SURG 95 J TRAUMA 87 J TRAUMA 89
86 TRANSPLANTATION: CHALLENGES DECISION TIMING ORGAN AVAILABILITY ANHEPATIC MANAGEMENT ETHICAL ISSUES

87 ALGORITHM FOR BLEEDING MGMT. SCORE, ACS Surg
88 MAJOR ADVANCES TRAUMA CENTERS NONOPERATIVE MGMT. ADJUNCTIVE THERAPIES LIVER TRANSPLANTATION
89 SUMMARY COMMON INJURIES MOST MGMT. NOW NONOPERATIVE COMPLEX INJURIES: TECHNICAL CHALLENGES REMAIN FORMIDABLE MULTIDISCIPLINARY THERAPIES
90 Ali M. Cheaito, MD Bach. Sci., University of Michigan MD, Boston University General Surgery: Henry Ford Hospital Multiorgan Transplantation: UCLA Assistant Professor of Surgery, Division of General Surgery
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Management of biliary complications following damage control surgery for liver trauma
 Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Blunt liver trauma- brief review and computed tomography role
 Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
Liver Trauma. Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa
 Liver Trauma Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa J Pediatr Surg. 20:1;1985: 14-18 Pediatr Surg Int. 1990;5:392-396 Injury. 1991 Jul;22(4):310-4. Blunt
Liver Trauma Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa J Pediatr Surg. 20:1;1985: 14-18 Pediatr Surg Int. 1990;5:392-396 Injury. 1991 Jul;22(4):310-4. Blunt
R E V I E W P A P E R S
 POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 11, 554 563 10.2478/v10035-009-0090-1 R E V I E W P A P E R S Surgical management of liver trauma Marek Krawczyk, Piotr Arkuszewski Departament of General, Transplant
POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 11, 554 563 10.2478/v10035-009-0090-1 R E V I E W P A P E R S Surgical management of liver trauma Marek Krawczyk, Piotr Arkuszewski Departament of General, Transplant
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical Selective Prospective Study
 Med. J. Cairo Univ., Vol. 84, No. 2, June: 97-103, 2016 www.medicaljournalofcairouniversity.net Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical
Med. J. Cairo Univ., Vol. 84, No. 2, June: 97-103, 2016 www.medicaljournalofcairouniversity.net Conservative Management of Blunt Hepatic Trauma for Patients with High Severity Grades Injuries A Clinical
INTRODUCTION. who should undergo a spiral CT of the abdomen are listed in Table 1. In patients with gunshot wounds to the right thoracoabdominal
 72 Scandinavian Journal of Surgery 91: 72 79, 2002 D. V. Feliciano, G. S. Rozycki HEPATIC TRAUMA D. V. Feliciano, G. S. Rozycki Emory University School of Medicine, Grady Memorial Hospital, Atlanta, Georgia,
72 Scandinavian Journal of Surgery 91: 72 79, 2002 D. V. Feliciano, G. S. Rozycki HEPATIC TRAUMA D. V. Feliciano, G. S. Rozycki Emory University School of Medicine, Grady Memorial Hospital, Atlanta, Georgia,
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN
 TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN Usman Ali, Ashab Noor, Mian Mujahid Shah*, Waqar Alam Department of Surgery, Postgraduate Medical Institute, Lady Reading Hospital, Peshawar
TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN Usman Ali, Ashab Noor, Mian Mujahid Shah*, Waqar Alam Department of Surgery, Postgraduate Medical Institute, Lady Reading Hospital, Peshawar
Management of traumatic liver injuries, Mafraq hospital experience, UAE
 International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE
 MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Classification of Liver Trauma
 HPB Surgery, 1996, Vol.9, pp.235-238 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V. Published in The
HPB Surgery, 1996, Vol.9, pp.235-238 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V. Published in The
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Surgical Management of Liver Trauma
 ORIGINL RTICLE STRCT Surgical Management of Liver Trauma Munawar Jamil, Tariq Hassan Choudry, Tahir Minhaas, Tahir Idrees, Humera Sobia Objective Study design Place & Duration of study Methodology Results
ORIGINL RTICLE STRCT Surgical Management of Liver Trauma Munawar Jamil, Tariq Hassan Choudry, Tahir Minhaas, Tahir Idrees, Humera Sobia Objective Study design Place & Duration of study Methodology Results
Liver Transplantation
 1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,700 108,500 1.7 M Open access books available International authors and editors Downloads Our
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
The role of non-operative management (NOM) in blunt hepatic trauma
 in blunt hepatic trauma") Alexandria Journal of Medicine (2013) 49, 223 227 Alexandria University Faculty of Medicine Alexandria Journal of Medicine www.sciencedirect.com ORIGINAL ARTICLE The role of non-operative management (NOM)
Alexandria Journal of Medicine (2013) 49, 223 227 Alexandria University Faculty of Medicine Alexandria Journal of Medicine www.sciencedirect.com ORIGINAL ARTICLE The role of non-operative management (NOM)
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
ORIGINAL ARTICLE. Complications Following Renal Trauma
 ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
Renal Transplant Surgery
 Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Inferior Vena Cava Filters
 Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Inferior Vena Cava Filters and the American Society of Hematology Choosing Wisely Campaign Kevin P. Hubbard, DO, HMDC MACOI Chief - Division of Specialty Medicine Professor and Chair - Section of Internal
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
CT - the prime instrument for the critical. Critical Decisions & Critical Bleeds
 Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
Critical Decisions & Critical Bleeds Bertil Leidner, MD Karolinska University Hospital Huddinge Stockholm, Sweden CT - the prime instrument for the critical patient t The critical patient Traumatized In
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Acute, Blood, Trauma /ecr2015/C-2116
 The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Advances in Treatment of Traumatic Aortic Transection
 Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Advances in Treatment of Traumatic Aortic Transection Himanshu J. Patel MD University of Michigan Medical Center Author Disclosures Consulting fees from WL Gore Inc. There is no disease more conducive
Successful Endoscopic Therapy of Traumatic Bile Leaks
 Published online: February 25, 2013 1662 0631/13/0071 0056$38.00/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license),
Published online: February 25, 2013 1662 0631/13/0071 0056$38.00/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution- NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license),
LIVER RESECTION WITH INFLOW OCCLUSION. 1/2 years, then the other 11 patients died between 4 and 30 months (average survival
 HPB INTERNATIONAL 297 tumour was more aggressive or more advanced at the time of diagnosis; the figures only demonstrate that, without resection, some patients can live for prolonged periods of time (60%
HPB INTERNATIONAL 297 tumour was more aggressive or more advanced at the time of diagnosis; the figures only demonstrate that, without resection, some patients can live for prolonged periods of time (60%
This is a recommended algorithm of the Western Trauma
 ORIGINAL ARTICLE Western Trauma Association Critical Decisions in Trauma: Nonoperative Management of Adult Blunt Hepatic Trauma Rosemary A. Kozar, MD, PhD, Frederick A. Moore, MD, Ernest E. Moore, MD,
ORIGINAL ARTICLE Western Trauma Association Critical Decisions in Trauma: Nonoperative Management of Adult Blunt Hepatic Trauma Rosemary A. Kozar, MD, PhD, Frederick A. Moore, MD, Ernest E. Moore, MD,
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention?
 Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Hepatic Injuries in Blunt Trauma Abdomen
 ORIGINAL ARTICLE GAZALA FIRDOUS, KHALID JAVEED ABID ABSTRACT Aim: To study the outcome of grade III to VI hepatic injuries in blunt trauma abdomen at Mayo Hospital, Lahore. Study design: Descriptive study
ORIGINAL ARTICLE GAZALA FIRDOUS, KHALID JAVEED ABID ABSTRACT Aim: To study the outcome of grade III to VI hepatic injuries in blunt trauma abdomen at Mayo Hospital, Lahore. Study design: Descriptive study
Tranjugular Intrahepatic Portosystemic Shunt
 Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Tranjugular Intrahepatic Portosystemic Shunt Christopher Selhorst July 25, 2005 BIDMC Radiology Overview Portal Hypertension Indications, Contraindications The Procedure Case Review Complications Outcomes
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
HEPATECTOMY. Surgical Potpourri Session. ACS NSQIP National Conference Salt Lake City 2012
 HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
Non Operative Management of Isolated Blunt Liver Trauma: A Task of High Skilled Surgeons
 Journal of Surgery 2017; 5(6): 118-123 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.16 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Non Operative Management of Isolated Blunt
Journal of Surgery 2017; 5(6): 118-123 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.16 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Non Operative Management of Isolated Blunt
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Trauma MedEd. Emphasis: Solid Organ - Spleen January 2012 T RAUMA C ALENDAR OF E VENTS WESTERN TRAUMA ASSOCIATION 42 ND ANNUAL MEETING
 The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
PRESENTATION AND MANAGEMENT OF HEPATIC TRAUMA AT MAYO HOSPITAL
 E:/Biomedica/New Journal 2004/Bio-2.doc (A) PRESENTATION AND MANAGEMENT OF HEPATIC TRAUMA AT MAYO HOSPITAL FRAZ FAHIM, SYED MAZHAR ABBAS Department of Surgery, Mayo Hospital, Lahore Hepatic injury is one
E:/Biomedica/New Journal 2004/Bio-2.doc (A) PRESENTATION AND MANAGEMENT OF HEPATIC TRAUMA AT MAYO HOSPITAL FRAZ FAHIM, SYED MAZHAR ABBAS Department of Surgery, Mayo Hospital, Lahore Hepatic injury is one
Posthepatectomy Liver Failure. C. Jeske
 Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Emergency Laparotomy. Open vs Closed Abdomen
 Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Visceral Artery Aneurysms Endovascular vs. Open?
 Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.