ecompressive craniectomy in TBI
|
|
|
- Nora Heath
- 5 years ago
- Views:
Transcription



1 ecompressive craniectomy in TBI Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624 AZ ÉLETTUDOMÁNYI- KLINIKAI FELSŐOKTATÁS GYAKORLATORIENTÁLT ÉS HALLGATÓBARÁT KORSZERŰSÍTÉSE A VIDÉKI KÉPZŐHELYEK NEMZETKÖZI VERSENYKÉPESSÉGÉNEK ERŐSÍTÉSÉRE TÁMOP C-13/1/KONV
2 Definition Decompressive craniectomy is a method to open/expand the space that has defined closed by the Monro-Kellie doctrine in order to reduce ICP Primary DC: Preventive/preemptive craniectomy upon evacuation of a space occupying lesion Secondary DC: Decompressive craniectomy aimed at the reduction of ICP in lack of a space occupying lesion
3


4

5

6
7 Kocher, there is an ongoing debate about: Indications Timing Methods Cranium Dura Parenchyma EBM
8 Indications Primary indication is uncontrollable ICP......what does this mean?

9 CPP = MABP ICP 60 = 80-20


10 ICP-threshold of 20mmHg 6m outcome in 428 stbi cases Occurrence of ICP periods over 20 is associated with adverse outcome J. Neurosurg 75:S59-S66, 1991


11 In 207 stbi cases: ICP was over 20 if CT positive in 60% ICP was over 20 if CT negative in 13% ICP was over 20 if CT negative but two of the following occurred: age over 40 BPsyst under 90 decerebrate/decorticate posturing ICP J. Neurosurg 56: , 1982
12 Pécs Severe TBI Database- 308 cases ( )
13 Prolonged, refractory ICP is a bad prognosticator
14 Critical approach ICP and CPP are global measures Several studies, including the BEST TRIP trial highlight that treating ICP does not necessarily mean a treatment for brain injury
15 Deterioration is not exclusively caused by enlargement of the ICH cerebral infarction, measured by brain tissue oxygen monitoring, can occur despite normal ICP readings increased ICP detection is only responsible for half the episodes of cerebral ischemia. Van Santbrink H, Maas AI, Avezaat CJ. (1996). Continuous monitoring of partial pressure of brain tissue oxygen in patients with severe head injury. Neurosurgery; 38: Van Santbrink H, van den Brink WA, Steyerberg EW, Carmona Suazo JA, Avezaat CJ,Maas AI. (2003). Brain tissue oxygen response in severe traumatic brain injury. Acta Neurochirurgica; 145:
16 low PbO2 was associated with normal CPP, indicating that CPP could be an inadequate estimate of regional CBF in focal ischemic areas Stocchetti N, Chieregato A, De Marchi M, Coroci M, Benti R, Grimoldi N. (1998).High cerebral perfusion pressure improves low values of local brain tissue O2 tension (PtiO2) in focal lesions. Acta Neurochirurgica Supplementum (Wien); 71:
17 Multimodality monitoring in severe TBI MABP ICP CPP/PRx/CPPopt SATO 2 /Astrup Brain temperature Brain oxygenation/lycox Jugular bulb oxymetry ECG ECoG hemodynamics core/tympanic membrane temperature microdialisis/biomarkers


18 Causes of raised ICP following TBI
19 Timing of DC There is a lack of evidence to define when to perform DC Multimodality monitoring including trend- and waveform- analysis of ICP as well as PRx should provide a solid basis for this First exclude technical and extra-cns causes Next, define what measures had been done and what other second tier therapies can be applied The decision is based on local guidelines and individual decision, case-by case
20 Forms Frontal (bifrontal) With bony bridge over the SSS Without bony ridge over the SSS With cut over the frontal insertion of the falx (crista galli) Without Lateral (bilateral) fronto-temporo-parietal Dural opening Slit Curved-linear Wide radiate/stellate Dural closure None Approximating Watertight expansion (duroplasty)
21 Size The bigger the better... Any technical modification will be unnecessary when the size is adequate Minimum of 10cmx10cm Optimal is 12cmx12cm or over Large bone defect harbors more complications, particularly that of hydrocephalus



22
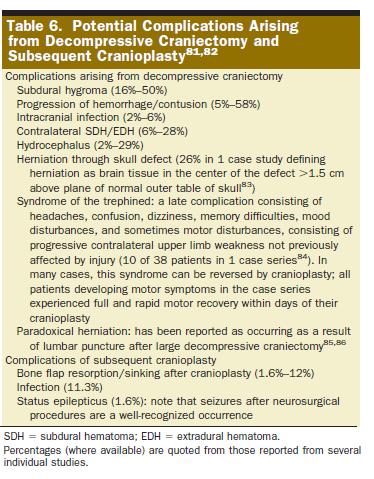
23 Complications related to DC (and CP)
24


25


26

27 Calvarial reconstruction using high-density porous polyethylene cranial hemispheres Nitin J Mokal, Mahinoor F Desai IJPS; 2011; Vol44

28


29

30

31 65 ys Sept Sept Sept



32 65 ys Sept Sept Sept
33 EBM...
34 Cochrane Database Syst Rev Sahuquillo J, Arikan F Decompressive craniectomy for the treatment of refractory high intracranial pressure in traumatic brain injury There is no evidence to support the routine use of secondary DC to reduce unfavorable outcome in adults with severe TBI and refractory high ICP. In the pediatric population DC reduces the risk of death and unfavorable outcome....this treatment maybe justified in patients below the age of 18 when maximal medical treatment has failed to control ICP. To date, there are no results from randomized trials to confirm or refute the effectiveness of DC in adults....results of non-randomized trials and controlled trials with historical controls involving adults, suggest that DC may be a useful option when maximal medical treatment has failed to control ICP.

35
36 Characteristics of the trial In 8y stbi patients (19-59y) in 15 tertiary care hospitals in Australia, New Zealand, and Saudi Arabia. treatment for ICP over 20 mm Hg early refractory elevation in intracranial pressure: a spontaneous (not stimulated) increase in intracranial pressure for more than 15 minutes (continuously or intermittently) within a 1-hour period, despite optimized first-tier interventions. interventions included optimized sedation, the normalization of arterial carbon dioxide pressure, and the use of mannitol, hypertonic saline, neuromuscular blockade, and external ventricular drainage
37 Randomization in 72 hours after injury to decompressive craniectomy plus standard care or to receive standard care alone Standard care: Brain Trauma Foundation - Guidelines. Second-tier options for refractory elevation of intracranial pressure: mild hypothermia (to 35 C), optimized use of barbiturates, both. Patients randomized to continued standard care: protocol permitted the use of lifesaving decompressive craniectomy after a period of 72 hours had elapsed since admission.

38

39

40
41 Conclusions of the study The method works The outcome is unaffected?????
42 Decompressive craniectomy does not improve outcome when it is done on patients who don t need it! (Chesnut, R., 2014, INTS, Budapest)
43 Why do patients not require DC? ICP is not elevated! Is ICP relevant to define the treatment options? Sometimes yes, sometimes not!
44 Let s forget the one size fits all approach! Individual pathobiology matters!
45 Mortality according to the main intracranial pathology & ICP monitoring 80% 70% 64.71% 60% 52.33% 50% 47.83% 40% 42.22% 42.86% 30% ICH ICH+SDH SDH Diffuse Penetrating Total ICP Monitoring+ ICP Monitoring-

46 Individual assessment of the pathobiology! Courtesy of Peter Smielewski
47 Conclusions In order to introduce a treatment we have to understand the pathobiology We also have to understand pathobiological processes evoked by/ operant at an individual level Treatment plans and decisions should be tailored to the actual patient

48
49 BEST:TRIP trial n = 324 Randomization to: Pressure monitoring group (n=157) Imaging - clinical examination group (n=167) Power calculation: 80% power to detect an increase of 10 percentage points in the % of patient with a favorable outcome (GOSE) Primary outcome measure: composite outcome at 6 months



50 Testing Two Protocols Courtesy of R.
51 Conclusions: BEST:TRIP Apparently sound hypothesis and design Groups comparable Care focused on maintaining monitored ICP 20 mm Hg was not shown to be superior to care based on imaging and clinical examination
52 BEST:TRIP Critical comments Conceptual: Any differences in outcome will be related to type and intensity of treatment, and not to the monitoring itself Both groups received ICP targeted treatment Statistical: Power calculations should NOT be based on the total number of patients but on the (expected) number with raised ICP Median/mean % of ICP > 20 mmhg: 7 and 20% In every fourth patient at the ICP group there was no raised ICP at all!!
53 BEST:TRIP Critical comments Composite outcome measures: half of them are neuropsychological GOSE: 5% benefit for ICP-group Confounding effects of: more agressive treatment in the cons. group, longer transfer times with no documetation on hypoxia/hypoperfusion
54 What is the problem?

55 What should ICP monitoring provide to us? timely detection of space occupying lesions user friendly, reliable, cost- efficient tool with minimal complication rate, based upon evidence based medicine
56 Does ICP monitoring help to identify those patients who are at risk for late deterioration?
57 Deterioration is not exclusively caused by enlargement of the ICH several studies have demonstrated that cerebral infarction, measured by brain tissue oxygen monitoring, can occur despite normal ICP readings increased ICP detection is only responsible for half the episodes of cerebral ischaemia. Van Santbrink H, Maas AI, Avezaat CJ. (1996). Continuous monitoring of partial pressure of brain tissue oxygen in patients with severe head injury. Neurosurgery; 38: Van Santbrink H, van den Brink WA, Steyerberg EW, Carmona Suazo JA, Avezaat CJ, Maas AI. (2003). Brain tissue oxygen response in severe traumatic brain injury. Acta Neurochirurgica; 145:
58 low PbO2 was associated with normal CPP, indicating that CPP could be an inadequate estimate of regional CBF in focal ischaemic areas Stocchetti N, Chieregato A, De Marchi M, Coroci M, Benti R, Grimoldi N. (1998).High cerebral perfusion pressure improves low values of local brain tissue O2 tension (PtiO2) in focal lesions. Acta Neurochirurgica Supplementum (Wien); 71:
59 44y car accident, driver EO 1, VR 2, MR 4: GCS: 7, pupils equal, reactive left hemiparesis severe pulmonary and mild liver contusion, unstable rib cage



60
61 CT Hgmm :00-21:00 0 ICP ART MEAN




62
63 Hgmm :00-21:00 Part.O2 PbrO2




64




65
66 MMSE = 97/100, IQ (TONI-3) = 108 full recovery back to work practically unaffected social functions normal endocrine checkups
67 Does ICP-monitoring improve outcome?
68 In order to prove that ICP monitoring per se improves outcome, assuming a 9% mortality reduction, a prospective randomized study including approximately 768 patients would be required
69 On the basis of our present knowledge this is an irrelevant question as. We do not have pathobiology driven therapeutic targets/decisions to make Connors AF Jr, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT Investigators. JAMA 1996;276: Muizelaar JP et al. Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J. Neurosurg, 1991 Nov;75(5): Can we cool down the room with the thermometer? we do not have surrogate markers to compare with
70 General considerations about neuromonitoring ICP monitoring: the rationale ICP monitoring: the debate Current practice/future directions
71 Rethinking our approaches to ICP monitoring/treatment ICP monitoring should NOT be discarded Think in terms of understanding what is going on Think in terms of strategies
72 Trend - Time - Multimodality Trend is more important than a single, actual value Raised ICP in patients awakening is normal The more widespread, relevant physiological information we gather is the best!
73 CPP Management The concept: Increase flow by increased driving force CPP = MABP - ICP CPP : ICP MABP Treat ICP Treat MABP Limitation: not indicated if auto regulation severely disturbed PRX and CPP opt. CPP Management Courtesy of A. Maas


74 Dose of ICP Compared an ICP Dose based on correlation with disturbed autoregulation (PRx) versus standard ICP > 20 mmhg in predicting clinical outcome Courtesy of R.

75 Goal directed therapy in Neuro ICU ICP < 20 CPP > 60 PBrO2 > 15 SjO2 > 55% Understanding what is going on Courtesy of A. Maas
76 While recognizing certain limitations of ICP monitoring, the most important message for the near future is: Maintain ICP monitoring as a cornerstone of treatment Keep up the critical approach and pathophysiology-driven decision making with information gathered from multimodal monitoring

77
78 Thank you for your attention!
TBI in the elderly. Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624
 TBI in the elderly Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624 AZ ÉLETTUDOMÁNYI- KLINIKAI FELSŐOKTATÁS GYAKORLATORIENTÁLT ÉS HALLGATÓBARÁT
TBI in the elderly Andras Buki M.D., Ph.D.,D.Sc. Department of Neurosurgery, Medical Faculty of Pecs University, Pecs, Hungary, H-7624 AZ ÉLETTUDOMÁNYI- KLINIKAI FELSŐOKTATÁS GYAKORLATORIENTÁLT ÉS HALLGATÓBARÁT
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI
 The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
The Open Critical Care Medicine Journal,, 1, -3 Open Access Cerebral Oxygen Desaturation with Normal ICP and CPP in Severe TBI Sylvain Palmer *,1 and Mary Kay Bader 1 Orange County Neurological Associates,
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Decompressive craniectomy following traumatic brain injury
 Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
Decompressive craniectomy following traumatic brain injury Peter Hutchinson Division of Academic Neurosurgery University of Cambridge Escalating cycle of brain swelling Primary insult Brain swelling Secondary
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome?
 11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
11. Traumatic brain injury. Links between ICP, CPP, PRx monitoring and outcome after TBI. Does CT picture help in prediction of outcome? Critical levels of CPP, ICP and PRx Percentage of patients in outcome
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Multimodal monitoring to individualize care in TBI
 Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Multimodal monitoring to individualize care in TBI Critical Care Canada Forum 2017 October 4 th, 2017 Donald Griesdale MD MPH Associate Professor Department of Anesthesiology, Pharmacology & Therapeutics
Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality
 Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium
 CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
CPPopt: matters to be solved before or by an RCT? Geert Meyfroidt, MD, PhD Intensive Care Medicine University Hospitals Leuven Belgium Financial disclosures Research Foundation, Flanders (senior clinical
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Early Treatment of TBI A Prospective Study from Austria
 Early Treatment of TBI A Prospective Study from Austria Walter Mauritz MD, PhD Dept. of Anaesthesiology & Critical Care Trauma Hospital XX, 1200 Vienna, Austria International Neurotrauma Research Organisation,
Early Treatment of TBI A Prospective Study from Austria Walter Mauritz MD, PhD Dept. of Anaesthesiology & Critical Care Trauma Hospital XX, 1200 Vienna, Austria International Neurotrauma Research Organisation,
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury?
 Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Is Neuromonitoring an expensive waste of time, in Severe Traumatic Brain Injury? Edema Engorgement Contusion Hematoma Hypoxia Diffuse Axonal Injury Ross Bullock, MD, PhD. Director, Neurotrauma,- University
Precision Medicine in Neurocritical Care: Should we individualize care?
 Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
Precision Medicine in Neurocritical Care: Should we individualize care? Victoria McCredie Toronto Western Hospital Critical Care Canada Forum 2 nd November 2016 Conflicts of interest None Outline 1. Precision
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
To date, head injury remains the leading cause of. Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation
 J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
J Neurosurg 111:683 687, 2009 Outcome in patients with blunt head trauma and a Glasgow Coma Scale score of 3 at presentation Clinical article Ro u k o z B. Ch a m o u n, M.D., Cl a u d i a S. Ro b e r
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Cerebral autoregulation is a complex intrinsic control. Time course for autoregulation recovery following severe traumatic brain injury
 J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
J Neurosurg 111:695 700, 2009 Time course for autoregulation recovery following severe traumatic brain injury Clinical article Gi l l E. Sv i r i, M.D., M.Sc., 1 Ru n e Aa s l i d, Ph.D., 2 Co l l e e
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Update sulle lesioni emorragiche posttraumatiche
 Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Update sulle lesioni emorragiche posttraumatiche Corrado Iaccarino Neurochirurgia-Neurotraumatologia AOU Parma Neurochirurgia d'urgenza IRCCS ASMN Reggio Emilia LAW UPDATING This document provides recommendations
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
See the corresponding editorial in this issue, p 643. J Neurosurg 111: , 2009
 See the corresponding editorial in this issue, p 643. J Neurosurg 111:644 649, 2009 Management guided by brain tissue oxygen monitoring and outcome following severe traumatic brain injury Clinical article
See the corresponding editorial in this issue, p 643. J Neurosurg 111:644 649, 2009 Management guided by brain tissue oxygen monitoring and outcome following severe traumatic brain injury Clinical article
Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury
 J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
J Med Dent Sci 2010; 57: 133-138 Original Article Cerebral Blood Flow and Metabolism during Mild Hypothermia in Patients with Severe Traumatic Brain Injury Hiroyuki Masaoka Department of Neurosurgery,
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery
 Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Do Prognostic Models Matter in Neurocritical Care?
 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Trauma is the leading cause of death in the first four decades of life, with head injury being
 Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
Correspondence to: Mr PJ Hutchinson, Academic Department of Neurosurgery, University of Cambridge, Box 167, Addenbrooke s Hospital, Cambridge CB2 2QQ, UK: p.hutch@which.net ACUTE HEAD INJURY FOR THE NEUROLOGIST
ICP. A Stepwise Protocol
 ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples.
. Pressure-reactivity index, computational methods. Clinical examples.") Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Pressure reactivity: Relationship between ICP and arterial blood pressure (ABP). Pressure-reactivity index, computational methods. Clinical examples. Optimization of cerebral perfusion pressure: Relationship
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Cosa chiedo all autoregolazione cerebrale?
 Frank Update in Traumatologia Cranica FRANK A. RASULO ANESTHESIOLOGY, INTENSIVE CARE, PERIOPERATIVE CARE and PAIN MEDICINE Spedali Civili University Hospital Brescia, Italy Cosa chiedo all autoregolazione
Frank Update in Traumatologia Cranica FRANK A. RASULO ANESTHESIOLOGY, INTENSIVE CARE, PERIOPERATIVE CARE and PAIN MEDICINE Spedali Civili University Hospital Brescia, Italy Cosa chiedo all autoregolazione
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Severe Head dinjury Management and Recent Advances
 Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation
Severe Head dinjury ent and Recent Advances Presenter Dr Shejoy P Joshua Moderator Dr AK Mahapatra Dr Deepak Kumar Gupta 1 KEY Epidemiology Resuscitation Primary survey Secondary survey Neurological evaluation
Pediatric Trauma Initial Evaluation and management
 Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
Pediatric Trauma Initial Evaluation and management Head Injury Closed head injury Penetrating head injury Closed Head Injury without Fractures Head injury is the most common cause of death and disability
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN
 Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
Marshall Scale for Head Trauma Mark C. Oswood, MD PhD Department of Radiology Hennepin County Medical Center, Minneapolis, MN History of Marshall scale Proposed by Marshall, et al in 1991 to classify head
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
RESEARCH HUMAN CLINICAL STUDIES
 TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES The Relationship Between Intracranial Pressure and Brain Oxygenation in Children With Severe Traumatic Brain Injury Ursula K. Rohlwink,
TOPIC RESEARCH HUMAN CLINICAL STUDIES RESEARCH HUMAN CLINICAL STUDIES The Relationship Between Intracranial Pressure and Brain Oxygenation in Children With Severe Traumatic Brain Injury Ursula K. Rohlwink,
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury
 Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
Neurosurg Focus 9 (5):E2, 2000 Bedside microdialysis for early detection of cerebral hypoxia in traumatic brain injury ASITA S. SARRAFZADEH, M.D., OLIVER W. SAKOWITZ, M.D., TIM A. CALLSEN, M.D., WOLFGANG
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
Head injury in children
 Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Head injury in children Michael Kim, MD Department of Emergency Medicine University of Wisconsin- Madison #1 cause of death and disability Bimodal distribution 62,000 hospitalization 564,000 ED visits
Medicines Protocol HYPERTONIC SALINE 5%
 Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Medicines Protocol HYPERTONIC SALINE 5% HYPERTONIC SALINE 5% v1.0 1/4 Protocol Details Version 1.0 Legal category POM Staff grades Registered Paramedic Registered Nurse Specialist Paramedic (Critical Care)
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature
 Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Intraoperative contralateral extradural hematoma during evacuation of traumatic acute extradural hematoma: A case report with review of literature Anand Sharma 1, Arti Sharma 2, Yashbir Dewan 1 1 Artemis
Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction
 Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
Elmer Press Case Report Surgical Management of an Unusual Case of Malignant Middle Cerebral Artery Infarction Jon Durrani a, c, Mohammed Rahman b, Phillip Porcelli a, Keith Kattner a Abstract Decompressive
A bs tr ac t. n engl j med 364;16 nejm.org april 21,
 The new england journal of medicine established in 1812 april 21, 2011 vol. 364 no. 16 Decompressive Craniectomy in Diffuse Traumatic Brain Injury D. James Cooper, M.D., Jeffrey V. Rosenfeld, M.D., Lynnette
The new england journal of medicine established in 1812 april 21, 2011 vol. 364 no. 16 Decompressive Craniectomy in Diffuse Traumatic Brain Injury D. James Cooper, M.D., Jeffrey V. Rosenfeld, M.D., Lynnette