MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE
|
|
|
- Hilary Erin Ryan
- 5 years ago
- Views:
Transcription
1 MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center Clinical Assistant Professor, Department of Surgery University of Illinois-Chicago DISCLOSURES Gift of Hope: Consultant on Critical Care Advisory Board 1
2 OBJECTIVES To discuss the non-operative and operative management of splenic, renal and liver injuries To discuss the utilization of interventional radiology in solid organ injury and non-operative management To discuss cases that demonstrate the combined approach to solid organ injury. OBJECTIVES To discuss the non-operative and operative management of splenic, renal and liver injuries To discuss the utilization of interventional radiology in solid organ injury and non-operative management To discuss cases that demonstrate the combined approach to solid organ injury. 2

3 SPLENIC INJURY The most commonly injured solid organ. Mechanisms of splenic injury Blunt Penetrating Management Nonoperative Operative Expectant TRUTH OR MYTH Intentional injury of the spleen was a method of assassination. Giraffes were thought to have exceptional speed because they did not have a spleen. The amount of spleen needed to preserve immune and filtering functions of the spleen is about 30-50% Pediatric splenic capsules are thicker and the parenchyma firmer and thus are more likely to be managed successfully nonoperatively. About 45% of blunt splenic injuries will require emergency surgery 3

4 GRADES OF INJURY Grade I-V Low grade I-II Moderate III High grade IV-V Grade I: -Subcapsular hematoma <10% surface area -Laceration/Capsular tear <1cm deep LOW GRADE ATOM, 2 nd edition





5 LOW GRADE Grade II: Subcapsular hematoma 10-50% surface area Intra-parenchymal hematoma <5cm Laceration 1-3cm without vessel involvement ATOM, 2 nd edition MODERATE GRADE Grade III: -Subcapsular hematoma >50% surface area or expanding -Intra-parenchymal hematoma >5cm -Ruptured hematoma -Laceration >3cm or with trabecular vessel involvement ATOM, 2 nd edition

 ATOM, 2 nd")


6 HIGH GRADE Grade IV: Laceration of segmental or hilar vessels causing major devascularization (>25% of spleen) ATOM, 2 nd edition HIGH GRADE Grade V: -Shattered spleen -Injury of hilar vessels with completely devascularized spleen ATOM, 2 nd edition

7 MANAGEMENT ABCDE Physicical examination Left upper quadrant pain Left lower chest wall pain Kehr s sign Left shoulder pain INITIAL MANAGEMENT Labs IV access Hemodynamic instability SBP <90 HR >130 Response to initial resuscitation 7
 Splenic salvage")
8 UNSTABLE BLUNT ABDOMINAL TRAUMA Grade 3-5 FAST Grade 3 FAST + Triage to CT if initial resuscitation responsive Grade 4 FAST + then to the operating room Selective CT scan if other suspected explanation for instability Grade 5 FAST + / - To the operating room EVOLUTION OF SPLENIC INJURY MANAGEMENT Adult Splenic salvage to avoid overwhelming post splenectomy sepsis (OPSI) Splenic salvage techniques Pediatrics-Best way to salvage the spleen was to not operate Non-operative management initiaily 30-70% Concern for missing intra-abdominal injuries Contra-indications: advanced age, fear of missing hollow viscous injury, >2U PRBC, neurological impairment, high grade injuries) Non-operative management increased to 85% Non-operative management with angio-embolization: Decrease in the failure rate to 10-20% 8
9 NONOPERATIVE MANAGEMENT EVOLUTION Emergence of new-generation CT scanners High success rate of angiographic embolization Better understanding of the natural history of solid organ injuries Conventional 67% nonthereapeutic exploratory laparotomy rate Goffete PP, Laterre PF. Traumatic injuries: imaging and intervention in post-traumatic complications (delayed intervention) Eur Ra MANAGEMENT DECISIONS FOR SPLENIC INJURY Presence and severity of hemodynamic instability Results of the initial workup of blunt abdominal trauma Availability of angiography Definition of failure Use of followup abdominal ct scanning 9
10 OPERATIVE MANAGEMENT Splenectomy Splenic salvage Stable patients Reimplantation Unproven method to preserve splenic function INTERVENTIONAL RADIOLOGY IR suite Monitoring in the same standards of an ICU Therapeutic embolization Aneurysm Arteriovenous fistula Extravasation How to embolize? Main splenic artery Reduces bleeding, but does not prevent late pseudoaneurysm rupture and will not likely treat AVF. Distal selective Stop bloodflow causing infarction and abscess Combination 10
 High rate of complications Labor intensive RISK OF FAILURE OF NONOPERATIVE MANAGEMENT Advanced age Large hemoperitoneum Higher Injury Severity Score Brain Injury")
11 VASCULAR BLUSH Hemodynamically stable (Grade 3-5) Angiography OR if angiography not immediately available Hemodynamically unstable (nonresponder) OR Aggressive angiography Highest rates of non-operative management (80%) High rate of complications Labor intensive RISK OF FAILURE OF NONOPERATIVE MANAGEMENT Advanced age Large hemoperitoneum Higher Injury Severity Score Brain Injury Subcapsular Hematoma Scalafini SJ, et al. Non-operative salvage of computed tomography diagnosed splenic injuries: utilization of angiography from triage and embolization for hemostasis. Lopez JM, et al. Subcapsular hematoma in blunt splenic injury: A significant predictor of failure of nonoperative management. J Trauma,
12 10 DOGS IN 1975 Artifical splenic trauma Embolization of the splenic artery 7 survived for 2 months Arteries were patent Parenchyma smaller, but trauma could not be identified Chuang VP, Reuter SR. Selective arterial embolization for the control of traumatic splenic bleeding. Invest Radiol 1975 Jan-Feb; 10(1): Diagnostic peritoneal lavage was the most reliable method of identifying intraperitoneal injuries. Cannot determine who can be treated nonoperatively based on the DPL CT was found to be reliable alternative to DPL but not practical to replace all DPL CT allowed for the nonoperative management of blunt abdominal trauma-no longer mandatory exploration 12

13 Splenic injury on CT Urgent angiography in those that did not require immediate operation Selective embolization with extravasation of contrast. Exravasation into the peritoneum-main splenic arterial branch embolization 13
14 Coil embolization was the best methods of occlusion of the proximal splenic artery Did not result in splenic infarction Blood flow returned to normal in a few weeks Pitressin was temporary and unpredictable Gelfoam embolized to the distal collateral circulation and caused infarction 14
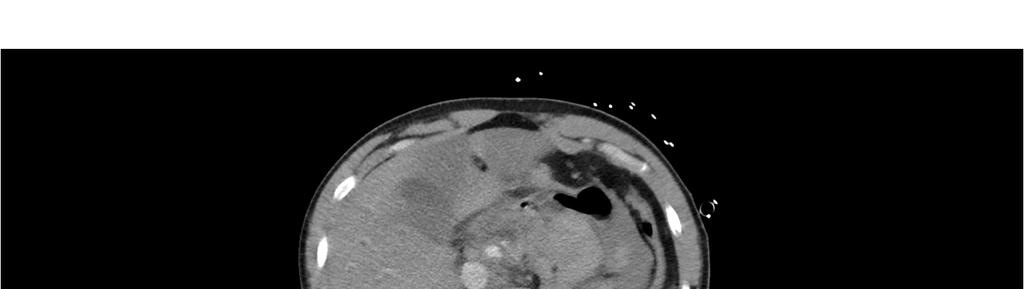
15 39 WOMAN YEAR OLD HIGH SPEED ROLLOVER History of ETOH abuse and cirrhosis Primary Survey ABC intact, GCS 15 Secondary Survey Contusion forehead C-spine tenderness Left upper quadrant pain Seatbelt sign across the chest and abdomen DIAGNOSIS Grade 2 splenic laceration with blush Mild hemoperitoneum 15
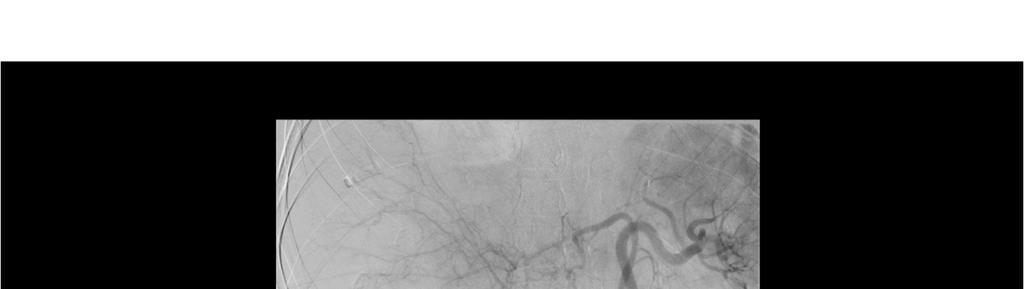
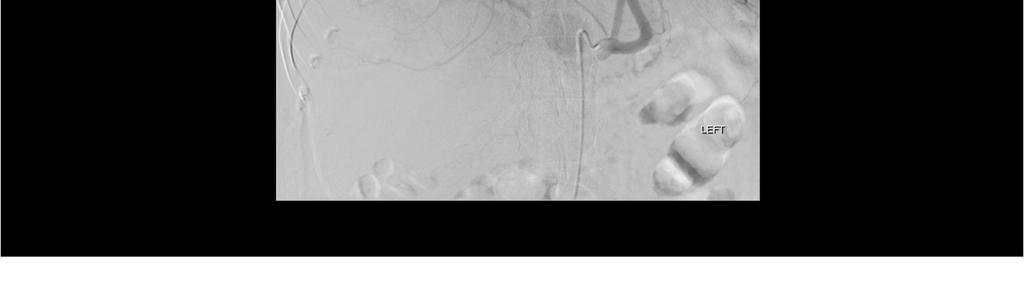
16 PLAN IR for angiography Findings Superselective splenic artery catheterization and subsequent arteriogram. Coil embolization of the branches of the splenic artery feeding the inferior spleen Coil embolization of the mid portion of the splenic artery. Discharged home HD #7 Return to the clinic HD #14 with abdominal pain 16

17 INTRAOPERATIVE FINDINGS Laparoscopic splenectomy. Pathology: Benign splenic tissue with hemorrhage, ischemia and necrosis. Search s Failure rate 31-48% of non-operative splenic management The vascular blush was seen in 67% of patients who failed nonoperative management Shackford SR, Molin M. Management of splenic injuries. Surg Clin North Am Godley CD, et al. Nonoperative management of blunt splenic injuries in adults: age over 55 year a powerful indicator for failure. J Am Coll Su Schurr MJ, et al. Management of blunt splenic trauma: computed tomographic contrast blush predicts failure of nonoperative management. J 17

18 year interval ending in June 1997 Hemodynamically stable and no immediate need for operation CT scan of the abdomen within an hour of presentation Followup CT hours after presentation Blush Well-circumscribed, intraparenchymal collection of contrastthat is hyperdense with respect to the surrounding splenic parenchyma Arteriography Confirm the pseudoaneurysm Selective embolization No main splenic artery embolization 18

19 524 patients 180 (34%) underwent urgent exploration 344 stable patients CT scan 61 % non-operative management in this study. PSEUDOANEURYSM 31 pseudoaneurysms Initial CT: 8 Followup CT: 23 Angiography Mean time: 4 days 30 underwent angiography 23 managed nonoperatively 20 pseudoaneurysm confirmed on angiogram 3 without pseudoaneurysm 7 patients OR Unable to be embolized OR for exploration Davis, et al

20 FAILURE ON NONOPERATIVE MANAGEMENT AND NO PSEUDOANEURYSM Number of patients: 15 7 clinical evidence of hemorrhage 6 Worsening appearance on CT 1 delay in diagnosis pancreatic injury 1 splenic infacrction Davis, et al Retrospective chart review 126 patients Angiography at admission 68% negative 32% embolization 8% laparotomy 92% salvage rate J Trauma,
 Median duration of mechanical ventilation Infectious Complications 12.8% had embolization 11% embolized failed 21.")
21 NONOPERATIVE MANAGEMENT IS AS EFFECTIVE AS IMMEDIATE SPLENECTOMY FOR ADULT PATIENTS WITH HIGH-GRADE BLUNT SPLENIC INJURY American College of Surgeons Trauma Quality Improvement Program (TQIP) Non-operative and Immediate Splenectomy Patients were matched (n=1516) Median duration of mechanical ventilation Infectious Complications 12.8% had embolization 11% embolized failed 21.4 not embolized failed ** ** Scarborough JE, et al. Nonoperative management is as effective as immediate splenectomy for adult patients with high-grade blunt sp J Am Col Surg, August 2016 National Trauma Databank 18 years or older with high grade blunt splenic injury Level 1-2 trauma centers Manage over 20 patients in one year Annals of Surgery, March
22 53689 patients Grade 3 or higher ** ** ** ** Patients treated in an angio center Higher ISS More commonly had Grade IV Lower admission Motor GCS scores More commonly Level 1 centers More commonly university affiliated Tended to be larger hospitals ** ** Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March % rate of angiography in 2008 to 14.1% in 2014 Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March
23 Splenectomy rates are the same at angio centers Spenectomy rates decreased in non-angiocenters in combined and grade 3 and 4 Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March 2017 Splenectomy within 6h of admission Reduction only in the splenectomy rate in Grade III injuries in non-angio centers Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March
24 Angio- Reduction 5.4% to 4.1% Non-angio Reduction 6.0% to 3.3% Reduction in the rate of late splenectomy in all groups except the Grade IV splenic injuries in the non-angio centers Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March 2017 No differences in mortality over time Late splenectomy overall associated with increased mortality in Grade III and IV Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March
25 CONCLUSIONS Angiography is not the only factor driving the decreased rate of late splenectomy Increase in total hospital costs with angiography Role of angiography in Blunt Splenic Injury needs to be further defined Dolejs SC, et al. Overall splenectomy rates stable despite increasing usage of angiography in the management of high-grade blunt splenic injury. Annals of Surgery March 2017 No difference in splenic embolization and observation 25

26 No difference in splenic embolization and observation No difference in splenic embolization and observation No difference in the mortality in the two groups 26

27 No difference in the mortality in the two groups Significant variation among Level 1 trauma centers. Higher rates of embolization have higher splenic salvage. SPLENIC ANATOMY AND FUNCTION White pulp B-cell follicles Marginal Zone Macrophages Memory B-cells Red Pulp Erythrocyte filtering Measure of Immune function Immune response upon vaccination or by evaluation of B-cell subsets. Erythrocyte filtering Radionucleotide tests (scintigraphy) Clearance of labelled erythrocytes Count of Howell Jolly bodies Count of pitted red blood cells Schimmer JAG, et al. Splenic function after angioembolization for splenic trauma in children and adults: Asystemic review. In 27
28 SPLENIC COMPLICATIONS Reported up to 8% Vascular Complications (70% occur within 2 weeks of injury) Delayed rupture Pseudoaneurysm Arteriovenous Fistula Pseudocyst Abscess Goffete PP, Laterre PF. Traumatic injuries: imaging and intervention in post-traumatic complications (delayed intervention) Eur Ra LATE COMPLICATIONS >48 hours from injury-5-8% incidence Splenic abscess Pseudoaneurysm Hemorrhage Most require splenectomy Cocanour, CS, et al. Delayed complications of nonoperative management of blunt adult spenic trauma, Arch Black JJ, et al. Subcapsular hematoma as a predictor of delayed splenic rupture. Am Surg,
29 OVERWHELMING POST-SPLENECTOMY SEPSIS (OPSS) Encapsulated organisms Pnemococcus Meningiococcus Hemophilus Influenza 2-5 per 1000 Asplenic patients All but one study demonstrate no compromise of immune function with splenic artery embolization. No reports of OPSS in the literature after splenic artery embolization 70% mortality Schimmer JAG, et al. Splenic function after angioembolization for splenic trauma in children and adults: Asystemic review. In EMBOLIZATION OF THE SPLEEN AND IMMUNE FUNCTION Clearance of opsonized autologous red blood cells in normal controls and in patient who underwent splenic artery ligation No significant difference The spleen undergoes hypertrophy and as much as 80% can be removed Short gastrics are adequate to protect against pneumococcal challenge Scintigraphy-reticulo-endothelial system remains viable. Schwalke, et al. Splenic artery ligation for splenic salvage: Clinical experience and immune function. JTrauma, 1991 Greco and Alvarez. Regeneration of the spleen after etopic implantation and partial splenectomy. Surg,
30 EAST PRACTICE GUIDELINES Level 1 Peritonitis or hemodynamic instability should go for urgent laparotomy Level 2 Routine laparotomy not necessary with isolate splenic in jury Grade of injury, age >55, neurologic status, and associated injuries do not exclude non-operative management Consider angiography in grade III or greater, presence of a blush, moderate hemoperitoneum, or evidence of ongoing bleeding. Nonoperative management should only be considered in an environment that allows. EAST.org, 2012 EAST PRACTICE GUIDELINES Level 3 Consider followup imaging with clinical changes Contrast blush is not an absolute indication for angiographic intervention Angiography can be used as an adjunct to non-operative management in high risk patients Venous thromboembolism can be used for patients with isolated blunt splenic injuries without increasing failure of nonoperative rate EAST.org,
31 THE LIVER INITIAL EVALUATION ABCDE Hemodynamically stable Associated abdominal injuries 31
32 GRADES OF LIVER INJURY trauma.org, 2017 APPROACH Operative Packing Hemostatic agents Suturing Total Hepatic Isolation Nonoperative % success Angiographic intervention ERCP (Endoscopic Retrograde Cholangiopancreatography) Percutaneous drainage Does surgery lead to further bleeding and unnecessary interventions and complications?? 32


33 SPLENIC AND LIVER BLUSH Patients with no blush on angiography were more than twice as likely to rebleed compared with those with angiographic evidence of blush. SPLEEN: 25% vs 10%, P <.05 LIVER 32% vs 11%, P =.046 Alarhayem, et al. Blush at first sight : Significance of computed tomographic and angiographic discrepancy in patient with blunt abdominal trauma. Am J Surgery,
34 CONSIDERATIONS No consistent correlation between the grade and failure on nonoperative management Hemodynamic status is more important Limitation of persistent bleeding or delayed bleeding with early angiography Poletti, et al CT grade III or higher Evidence of arterial injury (blush) Evidence of hepatic venous injury FAILURES OF NONOPERATIVE MANAGEMENT OF THE LIVER Hemodynamic instability is the cause of 75% of failures Delayed hemorrhage incidence is % Most common complication Most common cause of death Complication rate increases with the grade of injury 34
35 COMPLICATIONS LIVER 50-60% of patients with grade IV or V liver or splenic lacerations require some type of interventional treatment Vascular Delayed hemorrhage (2.4-5%) Vascular abnormalities 1-2% Pseudoaneurysm Arterivenous fistula Hemobilia (<1%) Liver and Biliary complications Bilhemia Bile leaks (biliary fistula and biloma) Bile peritonitis Biliary Stricture Sepsis Goffete PP, Laterre PF. Traumatic injuries: imaging and intervention in post-traumatic complications (delayed intervention) Eur R 30 YEAR OLD IN A MOTOR VEHICLE COLLISION Airway-Patent and breathing spontaneously Breathing-Saturation 100%, Breath sounds equal, crepitus left anterior chest wall Circulation-Intact. BP 130s, HR 90 GCS 3 Intubated for airway protection Left chest wall does not expand well and is smaller in volume than the right Desaturation Hypotension 35




36 36


37 Chest tube placement 900mL out Stabilized. Saturations improved 37

38 SECONDARY Left abdominal wall abrasion Left chest wall with crepitus. No rectal tone No extremity deformities FAST negative 38



39 39

40 40
41 41
42 TO THE OPERATING ROOM Pre-op diagnosis Left diaphragmatic rupture Free fluid/blood in the pelvis Hypoperfused left hepatic lobe Post-op diagnosis Left diaphragmatic rupture Grade 2 liver laceration stellate Grade 1 pancreatic hematoma Doppler signal in the porta hepatis, and palpable pulse Normal gallbladder THE NEXT DAY Hypotensive Acidotic Increased airway pressures Compartment syndrome Intestinal ischemia? 42

43 OPERATING ROOM Re-opened Compartment syndrome Gangrenous gallbladder Mottled liver at the gallbladder bed COURSE Hospitalized for 1.5 months Acute kidney Injury Acute respiratory failure Portal Hepatic Duplex Good flow in the heparic and portal vessels Limited study CT Abdomen and Pelvis 10 days later 43
44 10 DAYS LATER 2.5 MONTHS LATER 44



45 45

46 46

47 FINDINGS Proper hepatic artery occlusion and pseudoaneurysm Replaced left hepatic artery whic h cross collateralizes to the right l obe of the liver Ischemic dilation of biliary ducts in the right lobe of the liver 1.5 YEARS LATER 47
48 EAST PRACTICE GUIDELINES Level 1 Patients who are hemodynamically unstable or who have diffuse peritonitis after blunt trauma should be taken urgently for laparotomy Level 2 A routine laparotomy in hemodynamically stable patients with liver injury is not indicated Angiography may be considered first line intervention in the transient responder to resuscitation as and adjunct to possible operative intervention Grade of injury, age >55, neurologic status, and associated injuries do not exclude non-operative management Angiographic embolization should be considered in the hemodynamically stable patient with evidence of extravasation on CT scan Nonoperative management should only be considered in an environment that EAST.org, 2012 allows. 48

49 EAST PRACTICE GUIDELINES Level 3 Consider followup imaging with clinical changes Interventional modalities including ERCP, angiography, laparoscopy, and drainage percutaneously may be required to manage complications Venous thromboembolism can be used for patients with isolated blunt splenic injuries without increasing failure of nonoperative rate EAST.org, 2012 CONCLUSIONS Splenic injury has evolved to increase the success of nonoperative management Need to define further the optimal role for angiographic embolization in splenic injuries. Liver injuries utilize both interventional, endoscopic and surgical strategies for salvage of function and have a high nonoperative rate 49
50 THANK YOU Questions? 50
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists
 Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Blunt liver trauma- brief review and computed tomography role
 Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Trauma MedEd. Emphasis: Solid Organ - Spleen January 2012 T RAUMA C ALENDAR OF E VENTS WESTERN TRAUMA ASSOCIATION 42 ND ANNUAL MEETING
 The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
The Trauma Professional s Blog Trauma MedEd Emphasis: Solid Organ - Spleen January 2012 Grading Spleen Injuries - Simplified Spleen injury grading is not as complicated as people think! The grading system
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY
 CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury
 Chin J Radiol 2005; 30: 1-7 1 Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury YU-SAN LIAO YU-FAN CHENG TUNG-LIANG HUANG PAO-CHU YU CHUNG-CHENG HUANG
Chin J Radiol 2005; 30: 1-7 1 Efficacy of Emergent Splenic Artery Embolization in Conservative Treatment of High Grade Splenic Injury YU-SAN LIAO YU-FAN CHENG TUNG-LIANG HUANG PAO-CHU YU CHUNG-CHENG HUANG
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications
 Clinical Radiology (2004) 59, 342 348 CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications L.A. Miller, S.E. Mirvis, K. Shanmuganathan, A.S. Ohson*
Clinical Radiology (2004) 59, 342 348 CT diagnosis of splenic infarction in blunt trauma: imaging features, clinical significance and complications L.A. Miller, S.E. Mirvis, K. Shanmuganathan, A.S. Ohson*
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Splenic Trauma Where to Occlude and with what
 Splenic Trauma Where to Occlude and with what Trauma session, Thurday May 5, 2016 Pierre GOFFETTE St-Luc University Hospital Brussels Pierre Goffette, M.D. Consultant/Advisory Board: Covidien (Neuro) and
Splenic Trauma Where to Occlude and with what Trauma session, Thurday May 5, 2016 Pierre GOFFETTE St-Luc University Hospital Brussels Pierre Goffette, M.D. Consultant/Advisory Board: Covidien (Neuro) and
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Endovascular management of blunt trauma to the
 Endovascular Management of Abdominal Solid Organ Trauma Indications and embolic agents for successful noninvasive treatment. BY RICARDO YAMADA, MD; MARCELO GUIMARAES, MD, FSIR; AND CLAUDIO SCHÖNHOLZ, MD
Endovascular Management of Abdominal Solid Organ Trauma Indications and embolic agents for successful noninvasive treatment. BY RICARDO YAMADA, MD; MARCELO GUIMARAES, MD, FSIR; AND CLAUDIO SCHÖNHOLZ, MD
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Conservative Management of Splenic Injuries
 Conservative Management of Splenic Injuries *Satyanarayana Rao S. V. 1, Ramkishan 1, Prabakar Rao P. V. 2 Research Article 1. Department of Surgery, Katuri Medical College and Hospital, Guntur-5222019,
Conservative Management of Splenic Injuries *Satyanarayana Rao S. V. 1, Ramkishan 1, Prabakar Rao P. V. 2 Research Article 1. Department of Surgery, Katuri Medical College and Hospital, Guntur-5222019,
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Blunt Abdominal Trauma Evaluation and Management Guideline PEDIATRIC Practice Management Guideline Contact: Trauma Center
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention?
 Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Does a Blush on CT following Blunt Abdominal Injury Necessitate an Invasive Intervention? Ragavan V Siddharthan, MD, Martha-Conley Ingram, BS., Andrew Morris, MD, Curtis Travers, MPH, Courtney McCracken,
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
ORIGINAL ARTICLE. Complications Following Renal Trauma
 ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Acute, Blood, Trauma /ecr2015/C-2116
 The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
The Baltimore CT Severity Index (CTSI) versus the American Association of Surgical Trauma (AAST) for grading splenic Injury on CT: Use and implications of an imaging based grading system for splenic injury
Radiation dose considerations. > 80 million total CT scans / year in USA in 2010 (25% ED)
") Martin Gunn Department of Radiology University of Washington I have no actual or potential conflict of interest in relationship to this presentation. I do have the following declarations: Grant support:
Martin Gunn Department of Radiology University of Washington I have no actual or potential conflict of interest in relationship to this presentation. I do have the following declarations: Grant support:
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings
, DSA and Homeostatic Embolization Findings") Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings Poster No.: C-2495 Congress: ECR 2012 Type: Educational Exhibit Authors: B. ALPARSLAN, N. YILDIRIM,
Intraabdominal Active Bleeding: Helical CT, MDCT (64slice), DSA and Homeostatic Embolization Findings Poster No.: C-2495 Congress: ECR 2012 Type: Educational Exhibit Authors: B. ALPARSLAN, N. YILDIRIM,
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Role of the Radiologist
 Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
Diagnosis and Treatment of Blunt Cerebrovascular Injuries NORDTER Consensus Conference October 22-24, 2007 Clint W. Sliker, M.D. University of Maryland Medical Center R Adams Cowley Shock Trauma Center
MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY
 GRADING FOR SOLID ABDOMINAL ORGAN INJURY") MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY AUTHORS & DISCLOSURE OF COMMERCIAL INTEREST: Jennifer Thomas 1
MAKING THE GRADE FOR PEDIATRIC TRAUMA THE REVIEW AND IMPLEMENTATION OF COMPUTED TOMOGRAPHIC (CT) GRADING FOR SOLID ABDOMINAL ORGAN INJURY AUTHORS & DISCLOSURE OF COMMERCIAL INTEREST: Jennifer Thomas 1
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy
 The Ochsner Journal 13:259 263, 2013 Ó Academic Division of Ochsner Clinic Foundation Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy Cara Irwine,
The Ochsner Journal 13:259 263, 2013 Ó Academic Division of Ochsner Clinic Foundation Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy Cara Irwine,
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Transcatheter Arterial Embolization of Traumatic Lumbar Artery Injury: Experience in One Institution
 J Radiol Sci 2011; 36: 31-36 Transcatheter Arterial Embolization of Traumatic Lumbar Artery Injury: Experience in One Institution Sheng-Che Hung 1,2,3,5 Huan-Wu Chen 3,5 Yon-Cheong Wong 3,5 Cheng-Hsien
J Radiol Sci 2011; 36: 31-36 Transcatheter Arterial Embolization of Traumatic Lumbar Artery Injury: Experience in One Institution Sheng-Che Hung 1,2,3,5 Huan-Wu Chen 3,5 Yon-Cheong Wong 3,5 Cheng-Hsien
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma
 Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Med. J. Cairo Univ., Vol. 80, No. 1, September: 575-584, 2012 www.medicaljournalofcairouniversity.com Conservative Versus Delayed Laparoscopic Exploration for Blunt Abdominal Trauma TAMER M. NABIL, M.D.*;
Case Endovascular management of non maturing dyalisis vascular access
 Case 10238 Endovascular management of non maturing dyalisis vascular access Guedes Pinto 1, Erique; Madeira 2, Célia; Sousa 3, Marta; Penha 1, Diana; Rosa 1, Luís; Germano 1, Ana; Baptista 1, Manuela 1
Case 10238 Endovascular management of non maturing dyalisis vascular access Guedes Pinto 1, Erique; Madeira 2, Célia; Sousa 3, Marta; Penha 1, Diana; Rosa 1, Luís; Germano 1, Ana; Baptista 1, Manuela 1
Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children
 Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children Poster No.: B-0862 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Paper A. Petraikin, T. Akhadov,
Multiphase contrast-enhanced MRI for control of subacute trauma of abdomen and chest in children Poster No.: B-0862 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Paper A. Petraikin, T. Akhadov,
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway
 MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
MISSED FINDINGS IN EMERGENCY RADIOLOGY: CASE BASE SESSION 5 th Nordic Trauma Radiology Course Oslo, Norway K.SHANMUGANATHAN M.D. EASILY MISSED FINDINGS IN EMERGENCY RADIOLOGY OBJECTIVES Commonly missed
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
The role for contrast-enhanced ultrasonography outside of focal liver lesions
 The role for contrast-enhanced ultrasonography outside of focal liver lesions Paul S. Sidhu King s College Hospital, London, UK Introduction Contrast-enhanced ultrasonography (US) of focal liver lesions
The role for contrast-enhanced ultrasonography outside of focal liver lesions Paul S. Sidhu King s College Hospital, London, UK Introduction Contrast-enhanced ultrasonography (US) of focal liver lesions
Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1
 Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1 1 Department of Vascular Surgery, 2 Department of Radiology/Interventional Radiology Unit and 3 Department of
Tasopoulou KM 1, Argyriou C 1, Mantatzis M 2, Kantartzi K 3, Passadakis P 3, Georgiadis GS 1 1 Department of Vascular Surgery, 2 Department of Radiology/Interventional Radiology Unit and 3 Department of
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Multidetector CT of Blunt Abdominal Trauma 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Reviews and Commentary
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Liver Trauma. Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa
 Liver Trauma Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa J Pediatr Surg. 20:1;1985: 14-18 Pediatr Surg Int. 1990;5:392-396 Injury. 1991 Jul;22(4):310-4. Blunt
Liver Trauma Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa J Pediatr Surg. 20:1;1985: 14-18 Pediatr Surg Int. 1990;5:392-396 Injury. 1991 Jul;22(4):310-4. Blunt
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience
 Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE. T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar
 ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
ACUTE PANCREATITIS: NEW CLASSIFICATION OF AN OLD FOE T Barrow, A Nasrullah, S Liong, V Rudralingam, S A Sukumar LEARNING OBJECTIVES q Through a series of cases illustrate the updated Atlanta symposium
CHIEF COMPLAINT & HPI
 THE GREAT HOUDINI Resident: Marc Lim, MD Attending: Shekher Maddineni, MD Program/Department: Westchester Medical Center/New York Medical College/Department of Radiology CHIEF COMPLAINT & HPI Chief Complaint
THE GREAT HOUDINI Resident: Marc Lim, MD Attending: Shekher Maddineni, MD Program/Department: Westchester Medical Center/New York Medical College/Department of Radiology CHIEF COMPLAINT & HPI Chief Complaint
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,