Liver Trauma. Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa
|
|
|
- Blake Hudson
- 5 years ago
- Views:
Transcription



1 Liver Trauma Alastair J W Millar Red Cross War Memorial Children s Hospital Cape Town, South Africa

2 J Pediatr Surg. 20:1;1985: Pediatr Surg Int. 1990;5: Injury Jul;22(4): Blunt liver trauma in children. Cywes S, Bass DH, Rode H, Millar AJ. Department of Paediatric Surgery, University of Cape Town, South Africa. Liver injuries in children: The role of selective non-operative management A. Landau, A.B. van As, A. Numanoglu, A.J.W. Millar and H. Rode Trauma Unit, Department of Pediatric Surgery, Red Cross Children's Hospital. Injury :66-71
3 Blunt liver trauma The liver is the most frequently injured solid organ following blunt abdominal injury in children Selective non-operative management of blunt liver trauma in haemodynamically stable patients is well established and accepted by most paediatric surgical centres. Surgical intervention in paediatric liver trauma is based on haemodynamic instability that persists despite ongoing resuscitation Biliary injuries are often missed until clinically manifest Major liver trauma is still associated with a significant mortality
![Patterns of liver injury ] Peritoneal and vascular fixed attachments Pliable chest wall & exposure in a protuberant abdomen of a child The direction, velocity, grade and site of blunt force as well](/docs-images/92/109798448/images/4-0.jpg "as the position and motion of the victim contribute to the pattern and severity of the injury Subcapsular haematoma/contusion Parenchymal damage/laceration Hepatic vascular disruption contrast")
4 Patterns of liver injury ] Peritoneal and vascular fixed attachments Pliable chest wall & exposure in a protuberant abdomen of a child The direction, velocity, grade and site of blunt force as well as the position and motion of the victim contribute to the pattern and severity of the injury Subcapsular haematoma/contusion Parenchymal damage/laceration Hepatic vascular disruption contrast extravasation Bile duct injury intrahepatic & extrahepatic -

5 Schematic diagram of the liver noting the structures at each potential site of injury


![traffic] Anterior](/docs-images/92/109798448/images/6-2.jpg "acceleration")

6 Patterns of injury Oblique right chest [pedestrian traffic] Anterior acceleration injury - laceration to the L or R of the Falciform ligament



![traffic]](/docs-images/92/109798448/images/7-3.jpg "Compression")
7 Patterns of injury Deceleration injury [falls from a height, pedestrian traffic] Compression injury [roll over]
8 Natural History of different types of injury Retroperitoneal area tamponade but hepatic vein # may bleed ++ Glisson s capsule intact + bleeding expanding subcapsular haematoma Haematoma contained within the liver parenchyma - expansion & liquefaction - absorption 2 to 3 months - infection abscess - encysted Arterial rupture expansion on-going bleeding - pseudoaneurysm & delayed bleed # or haemobilia - arterio-portal fistula - peripheral: most close - central: may lead to portal hypertension Bile duct # - partial will heal if distal duct intact but may require intra-ductal pressure reduction for this to occur - larger # - on-going leak and bile ascites - stricture - biliary fistula if duct from a segment disrupted but otherwise viable

9 Diagnosis History + Physical examination ±tachycardia, ±hypotension, peritoneal irritation FAST better for unstable patients not stable enough for CT or as a screen for CT CT with contrast determine grade and look for active extravasation Coley et al. J Trauma 2000



10 AAST Liver Injury Grading [American Association for the Surgery of Trauma] Grade I Grade IV
11 CT-based Injury Severity of Blunt Hepatic Trauma CT-based Grade Criteria 1 Capsular avulsion, superficial laceration(s) less than 1 cm deep, subcapsular hematoma less than 1 cm in maximum thickness, periportal blood tracking only 2 Laceration(s) 1 3 cm deep, central-subcapsular hematoma(s) 1 3 cm in diameter 3 Laceration greater than 3 cm deep, central-subcapsular hematoma(s) greater than 3 cm in diameter 4 Massive central-subcapsular hematoma greater than 10 cm, lobar tissue destruction (maceration) or devascularization 5 Bilobar tissue destruction (maceration) or devascularization CT Criteria for Management of Blunt Liver Trauma: Correlation with Angiographic and Surgical Findings Pierre A. Poletti et al. 2000: Radiology 216;
12 Liver injuries at Red Cross Children s Hospital n=409 [32yrs] end [60%] [40%] 50 0 Isolated Associated
![Cause of Injury [n=409] 350 (86%) RTAs Pedestrian 303 (87%) Passenger 47](/docs-images/92/109798448/images/13-0.jpg "(13%) Cyclist 3 (0.")
13 Cause of Injury [n=409] 350 (86%) RTAs Pedestrian 303 (87%) Passenger 47 (13%) Cyclist 3 (0.4%0 17 (4%) Child abuse/assault 26 (6%) Falls from / on top of
14 Liver Injuries n = Right Left Bilateral Falciform ligament
15 Associated injuries [246 (60%) had multiple injuries] Head Abdominal Fractures Thorax
16 Intra abdominal injuries n = Spleen Renal Pancreas Bowel
17 Management outcome n = 409 Mean age:7 years (2-13) Non- operative management 368 (91%) [31% required blood transfusion - mean 17ml/kg] Operative management 38 (9%) [100% required blood transfusion - mean 30.4ml/kg] Died soon after arrival 3 Died after surgery 3 [2HI, 1 LI] Mean hospital stay: 7 days (r: 4-49)
18 APSA Guidelines APSA guidelines for hemodynamically stable children with isolated spleen or liver injury CT GRADE I II III IV Days in ICU None None None 1 day Hospital stay 2 days 3 days 4 days 5 days Pre discharge imaging Post discharge imaging Activity restrictions None None None None None None None None 3 weeks 4 weeks 5 weeks 6 weeks From Stylianos S, and APSA Trauma Committee: Evidence-based guidelines for resource utilization in children with isolated spleen or liver injury J Pediatr Surg 35: , 2000
19 Non-Operative Group (n=368) CT or liver scintigraphy [prior to 1984] NOM not conservative management High care or ICU Close monitoring of haemodynamic status Serial hemoglobin, electrolytes, LFT s, Blood pressure, serum lactate, base excess Transfusion requirements [<20ml/kg]
20 Non-Operative complications Ruptured sub-capsular haematoma 2 One delayed laparotomy One treated non-operatively Abscesses 7 Liver 3 Pelvic 1 Sub-phrenic 2 Infected abdominal wall 1 Pancreatic pseudocyst 1 Biliary fistula 2 Fat embolism 1 Adhesive bowel obstruction 1
![Operative Management - Surgical Techniques Simple Techniques [good access essential] Cautery, Pringle,](/docs-images/92/109798448/images/21-0.jpg "topical haemostatic agents, hepatotomy & suture ligation of superficial/deep vessels Complicated")
![Injuries Pringle to vascular exclusion & aortic clamping Mesh wrapping [not used] Packing Hepatic artery](/docs-images/92/109798448/images/21-1.jpg "ligation [used on 1 occasion only] Atrio-caval shunting [not used] Liver transplant [rare but life")
21 Operative Management - Surgical Techniques Simple Techniques [good access essential] Cautery, Pringle, topical haemostatic agents, hepatotomy & suture ligation of superficial/deep vessels Complicated Injuries Pringle to vascular exclusion & aortic clamping Mesh wrapping [not used] Packing Hepatic artery ligation [used on 1 occasion only] Atrio-caval shunting [not used] Liver transplant [rare but life saving] Pringle




22 Surgical techniques of haemorrhage control Pringle inflow occlusion Pringle + hepatotomy, control and suture


23 Grade 2-3 blunt injury with a blush of contrast requiring operation and hepatotomy to secure haemostasis +/- 25% failure of NOM with constant blush on CT +/- Angioembolization The failure rate of nonoperative management in children with splenic or liver injury with contrast blush on computed tomography: a systematic review C.H. van der Vlies et al. Journal of Pediatric Surgery (2010) 45,


24 11yr old blunt trauma increasing abdominal pain, distension & liver enlargement over 24hrs Huge sub-capsular haematoma under pressure with early necrosis of surrounding liver

25 CT and angio of grade IV injury with 2 areas of arterial bleeding First bleeder coiled note second still bleeding
26 Technique of peri-hepatic packing - Restoring the liver anatomy!
27 Follow-up Imaging used for follow-up Serial Ultrasound scan [long term] Serial Computer Tomography [clinical need] HIDA scan for suspected bile duct leak Of those who returned for follow-up all showed resolution and healing of hepatic injury after 3 to 9 months depending on the severity of the injury Intrahepatic vascular pedicle injury may be associated segmental atrophy
![Contrast Enhanced Ultrasound [CEUS] vs CT [in the acute phase]?](/docs-images/92/109798448/images/28-0.jpg "CEUS screening for pseudoaneurysms in children aged >10 yrs N Durkin et al.")
28 Contrast Enhanced Ultrasound [CEUS] vs CT [in the acute phase]? CEUS screening for pseudoaneurysms in children aged >10 yrs N Durkin et al., J Ped Surg ;2:
29 Liver injuries in children: The role of selective non-operative management A. Landau, A.B. van As, A. Numanoglu, A.J.W. Millar and H. Rode Trauma Unit, Department of Pediatric Surgery, Red Cross Children's Hospital. Injury :66-71 [updated to 2013] Management of liver injuries Died soon after arrival Non-operative 368 Operative 30 3 [severe polytrauma] Complications 25 (8%) Mortality Total [1 liver, 2 HI] Even though most patients can be treated non-operatively, the challenge is to identify the severely injured child early, institute aggressive resuscitation and expedite laparotomy.
30 Birmingham Children s Hospital West Midlands U.K. Tertiary / Quaternary Hepatobiliary and Transplant Centre Different spectrum of severity of injury + age up to 16yrs Fewer pedestrian injuries Bicycle - handle bar + High speed RTA with seat belt +


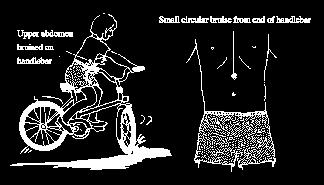
31 Liver trauma bicycle handle bar
32 Type & complications after local primary management in 15 patients referred to a tertiary centre Type of primary management Complications Types of complications Secondary management (no. of patients) Conservative Non-operative (n=8) Biliary (n=2) Biliary peritonitis ERCP, stenting Vascular (n=2) Rupture of arterial pseudo aneurysm Embolization Arterio-portal fistula Embolization Urgent Laparotomy (n=7) Biliary (n=4) Bile leaks Suture of duct (n=1) Transcystic biliary drain (n=3)
33 Biliary & vascular complications [ ] Type of biliary complication No. of Patients Day diagnosed Mode of diagnosis Biliary complications (n=13) Intra- hepatic biloma 3 2,3,4 Protocol TBIDA Bile leak into peritoneum 2 2,2 Protocol TBIDA Bile leak in the abdominal drain 4 3,3,5, 12, Bile in drain fluid Biliary peritonitis 3 12,22,18, Abdominal aspiration (n=2), Laparotomy (n=1) Others 1 2 At laparotomy Vascular complications (n=2) Intra-hepatic arterial pseudoaneurysm 1 22 Emergency angiography Arterioportal fistula Angio-embolization & follow-up ultrasound


34 11 year old female RTA Shocked resuscitation CT Intra-hepatic vascular injury Non-perfusion of left liver lobe Urgent laparotomy & left hepatectomy 3 year old boy RTA Shocked resuscitation CT with contrast blush Urgent laparotomy suture of laceration in portal vein



35 14 yr. old 22 days post injury, pain and malaena requiring transfusion
 in the right hepatic lobe,")
36 Ruptured hepatocellular adenoma after relatively minor trauma. Contrast-enhanced CT image shows a large heterogeneous low-attenuation mass (arrow) in the right hepatic lobe, and a loss of liver capsule integrity antero-laterally



37 Missed bile duct injury 11 year old RTA, haemodynamic instability despite resuscitation laparotomy & haemostasis POD 4 bile leak

38 Bile leaks what options Drain (percutaneous) and wait ERCP and stent +/- sphincterotomy [biodegarable stents, BOTOX inj.] Operative repair [op. cholangiogram] Cholecystectomy & trans-cystic duct tube decompression Roux-en-Y drain for persistant fistula
 Percutaneous drain & endoscopically placed stent b)")
- Multifenestrated feeding tube inserted through the cystic duct")

39 Elective TBIDA scan + drain + biliary decompression a) Intra-hepatic biloma Bile duct decompression and drain concept to promote healing of biliary leaks a) Percutaneous drain & endoscopically placed stent b) Open drain & T-tube c) Open drain + cholecystectomy & trans-cystic tube b) Bile leak into peritoneum Transcystic, transpapillary tube (TCTPT)- Multifenestrated feeding tube inserted through the cystic duct into the distal common bile duct and duodenum Papilla splinted open to release the positive pressure within the bile ducts Cholecystectomy + Trans cystic duct tube decompression and drain (Feneryou B & J. de Ville 2002)


40 Bile Leaks ERCP and stent/spincterotomy A 13yr old RTA with major left sided injury CT shows fluid and left liver laceration ERCP shows left duct # - treated by stent/sphincterotomy
41 Liver trauma Assessment / Resuscitation Clinically stable + physical signs CEUS & Contrast CT Major liver trauma Parenchymal fracture >4cmCT, Involving the hilum Clinically unstable Hypotension, tachycardia, pallor, falling haemoglobin Not-responding to resuscitation Laparotomy TBIDA scan Day 2-4 Intra-hepatic biloma observe/drain Arterial blush sign Intra peritoneal bile leak Angiography +/- embolisation ERCP, Stenting of ampulla Laparotomy, Transcystic biliary drain

42 The use of Recombinant Activated Factor VII in Damage-Control Surgery for Abdominal Trauma RJ Wood, CJ Westgarth-Taylor, H van Niekerk, O Hodges, J Thomas, AJW Millar. Department of Paediatric Surgery and Anaesthesia, Red Cross War Memorial Children s Hospital. University of Cape Town Introduction Recombinant FVIIa (NovoSeven) was developed for use in the treatment of severe haemophilia complicated with inhibitors against FVIII/FIX (1). It has subsequently been used successfully in treating massive haemorrhage, following cardiac surgery in non-haemophilia patients (2, 3). Few studies have looked at the use of rfviia in paediatric non-haemophiliac patients. We present 2 cases in which it has been used in conjunction with damage control surgery in the treatment of unresponsive Haemorrhagic shock, following blunt and penetrating abdominal trauma in paediatric patients at the Red Cross War Memorial Children s Hospital. Case A Patient A, a 20kg, seven year old male, presented to the trauma unit in June 2009 following a motor vehicle accident. He had sustained blunt abdominal trauma as well as a fractured right femur. He had unresponsive Grade 4 Haemorrhagic shock mandating an emergency laparotomy. At laparotomy he was found to have a grade 4 laceration to the Right Hepatic lobe. Intra-operative resuscitation with 45ml/kg of packed red cells and damage control surgical techniques: in-flow control (Pringle manoeuvre) and liver packing with abdominal swabs were instituted. rfviia (120 KIU) was administered in order to secure adequate haemostasis. The patient made a successful recovery after relook laparotomy in 48hrs to remove abdominal packs. Novo Nordisk Case B Patient B, a 40kg, nine year old female, presented to the trauma unit in July 2009 after sustaining 2 abdominal gunshot wounds. She had unresponsive Grade 4 Haemorrhagic shock and underwent emergency laparotomy. At laparotomy extensive intra-abdominal vascular injuries were found. She had sustained a through and through injury of the inferior vena cava and left iliac vein. Damage control techniques were employed and both vessels were ligated. Intra-operative resuscitation included 100ml/kg packed red cell transfusion as well as 15ml/kg of fresh frozen plasma and 15ml/kg of platelets. rfviia was administered intra-operatively and satisfactory hemostasis was secured. The patient made a successful recovery after a prolonged ICU stay Patient A, a 20kg, seven year old male, presented to the trauma unit in June 2009 following a motor vehicle accident. He had sustained blunt abdominal trauma as well as a fractured right femur. He had unresponsive Grade 4 Haemorrhagic shock Mechanism of action: mandating an emergency laparotomy. At laparotomy he was found to have a grade 4/5 laceration to the Right Hepatic lobe. Intra-operative resuscitation with 45ml/kg of packed red cells, FFP and damage control surgical techniques: in-flow control Discussion The management of unresponsive and transiently responsive Grade 3 & 4 Haemorrhagic shock usually requires surgical haemorrhage control. Abbreviated Laparotomy and Damage control techniques are well established in adult and paediatric practice(7). Major haemorrhage and extensive fluid resuscitation leads to dilution of coagulation factors, platelet dysfunction and impaired production of clotting factors because of tissue hypoxia caused by hypotension. Acidosis and hypothermia further aggravates coagulopathy. The use of rfviia in adult patients undergoing surgery has been extensively reported, but large randomized controlled trials are lacking (3). Fewer reports are available on its use in the paediatric patient group, but reports indicate that rfviia could significantly decrease blood-product administration (2, 4). Although expensive, the cost must be balanced against the potential risk of transmission of blood-borne pathogens, the cost of surgery and the cost of blood and plasma products (4). While rfviia may be extremely useful it can only be used in conjunction with timely surgery and resuscitation, after correction of Acidosis and Hypothermia (1, 5). Recommended target blood levels before administration are: hematocrit >24%, fibrinogen >0.5 to 1 g/l, platelets >50 to 100, /L, and ph 7.2 (5). Coagulopathy in the trauma patient is a complicated condition with numerous role-players (as outlined above); several protocols advocating specific transfusion ratio s (RBC:FFP:Plt) have been published (6). The role of rfviia in resuscitation protocols needs to be clarified and large trials are needed to elucidate this. (Pringle manoeuvre) and liver packing with abdominal swabs were instituted. rfviia (120 KIU) was administered in order to secure adequate haemostasis. The patient made a successful recovery after re-look laparotomy in 48hrs to remove abdominal packs. References 1. Mechanism of action, development and clinical experience of recombinant FVIIa; U. Hedner; Journal of Biotechnology issue 124, March 2006, p Paediatric off-label use of Recombinant Factor VIIa; J.A. Alten et al; Pediatrics vol 3, number 123, March 2009, p Recombinant Activated Factor VII in Cardiac Surgery: a Meta Analysis; A. Zangrillo et al; Journal of Cardiothoracic and Vascular Anaesthesia Vol 23, issue 1, Feb 2009, p Use of rfviia in Traumatic Liver Injuries in Children; R. Kulkarni et al; The Journal of Trauma number 56, June 2004, p Monitoring Recombinant Factor VIIa Treatment: Efficacy Depends on High Levels of Fibrinogen in a Model of Severe Dilutional Coagulopathy; M.T.Ganter et al; Journal of Cardiothoracic and Vascular Anaesthesia Vol 22, issue 5, October 2008, p Massive Transfusion Protocols: The Role of Aggressive Resuscitation Versus Product Ratio in Mortality Reduction; D.J. Riskin et al; Journal of American College of Surgeons, volume 209, issue 2, Aug 2009, p Damage control Surgery in Children, J. Hamil, Injury, July 2004, 35(7), p
43 Retro-hepatic IVC haemorrhage 1. Transverse incision with midline cranial extension 2. Packing of the liver and volume resuscitation with Rapid Infusion System prior to vascular isolation 3. Isolation of the intra-pericardial vena cava through a trans-diaphragmatic pericardial window 4. Control the suprarenal vena cava and porta hepatis 5. Repair of vein lacerations with vascular occlusion & continuous saline irrigation for improved visualization
44 Conclusions Contrast blush on initial CT scan is a useful indicator of ongoing haemorrhage and the need for urgent laparotomy or angiographic intervention. Bile duct injuries are more frequently seen in the select group of children suffering severe liver trauma. TBIDA scan is a sensitive investigation for bile duct injury in severe liver trauma in children. Adjunctive procedures such as angiography and embolization play an essential role in treating vascular injuries. The challenge is to identify early the severe injury requiring immediate life saving surgical intervention. Factor VII and packing can be life saving.
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I
 IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
IMAGING OF BLUNT ABDOMINAL TRAUMA, PART I QuickTime and a TIFF (Uncompressed) decompressor are needed to see this picture. Ruedi F. Thoeni, M. D. D University of California, San Francisco SCBT-MR Summer
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Blunt liver trauma- brief review and computed tomography role
 Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
Blunt liver trauma- brief review and computed tomography role Poster No.: C-2193 Congress: ECR 2015 Type: Authors: Keywords: DOI: Educational Exhibit S. C. S. Silva, R. Amaral, D. N. Silva, D. Garrido,
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון
 Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Surgical management of hepatic complications HELLP ד"ר ערן שדות יחידת ניתוחי כבד לבלב ודרכי מרה מרכז רפואי רבין, קמפוס בלינסון Outline Introduction HELPP and surgical liver complications 5 slides Real-life
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists
 Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
Splenic blunt trauma - from diagnostic MDCT to embolisation: The role of the radiologists Poster No.: C-1859 Congress: ECR 2010 Type: Educational Exhibit Topic: Interventional Radiology Authors: J. Cazejust,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
Case Conference. Discussion. Indications of Trauma Blue. Trauma Protocol In SKH. Trauma Blue VS. Trauma Red. Supervisor:VS 楊毓錚 Presenter:R1 周光緯
 Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Case Conference Supervisor:VS 楊毓錚 Presenter:R1 周光緯 Discussion 2010.7.14 2/81 Trauma Protocol In SKH Indications of Trauma Blue Trauma Blue VS. Trauma Red 3/81 Severe trauma mechanism : 1. Trauma to multiple
Citation for published version (APA): Nellensteijn, D. (2015). Pediatric abdominal injury: initial treatment and diagnostics [S.l.]: [S.n.
![Citation for published version (APA): Nellensteijn, D. (2015). Pediatric abdominal injury: initial treatment and diagnostics [S.l.]: [S.n.](/thumbs/87/97397435.jpg "Citation for published version (APA): Nellensteijn, D. (2015). Pediatric abdominal injury: initial treatment and diagnostics [S.l.]: [S.n.") University of Groningen Pediatric abdominal injury Nellensteijn, David IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
University of Groningen Pediatric abdominal injury Nellensteijn, David IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Guideline for the Management of Blunt Liver and Spleen Injuries
 Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
Pediatric Trauma Practice Guideline Management of Blunt Liver and Spleen Guideline for the Management of Blunt Liver and Spleen Background: Children are more vulnerable to blunt abdominal injury than adults.
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE
 MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
MANAGEMENT OF SOLID ORGAN INJURIES: NON- OPERATIVE, INTERVENTIONAL AND OPERATIVE April 4, 2017 Ellen Omi, MD, FACS Trauma and Critical Care Site Program Director, Surgery Advocate Christ Medical Center
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
ABDOMINAL TRAUMA MODULE
 INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
INTRODUCTION ABDOMINAL TRAUMA MODULE Blunt abdominal trauma most commonly occurs in the setting of motor vehicle accidents, pedestrian related trauma, direct blows and falls. 1 In these situations, blunt
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY
 NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
NON-OPERATIVE MANAGEMENT OF PEDIATRIC SOLID ORGAN INJURY JESSICA A. NAIDITCH, MD TRAUMA MEDICAL DIRECTOR, DELL CHILDREN S MEDICAL CENTER OF CENTRAL TEXAS ASSISTANT PROFESSOR OF SURGERY AND PERIOPERATIVE
TEVAR FOR! THORACIC AORTIC TRAUMA"
 10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
10th HKL Vascular Surgery Conference and Workshop" TEVAR FOR! THORACIC AORTIC TRAUMA" Dr Hanif Hussein" Vascular and General Surgeon" Department of Surgery" Hospital Kuala Lumpur" Source: MIROS! Thoracic
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Abdominal Solid Organ Injury 9th Nordic Trauma Radiology Course Aarhus, Denmark May 23-26, 2016 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD
 Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Fall down stairs. Left rib fractures. John A Cieslak III, MD, PhD Charan Singh, MD ? Splenic lacerations, hemoperitoneum, and traumatic pseudoaneurysm formation. High attenuation extraluminal contrast
Laparotomy for Abdominal Injury in Traffic Accidents
 Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Qasim O. Al-Qasabi, FRCS; Mohammed K. Alam, MS, FRCS (Ed); Arun K. Tyagi, FRCS; Abdulla Al-Kraida, FRCS; Mohammed I. Al-Sebayel, FRCS From the Departments of Surgery, Riyadh Central Hospital (Drs. Al-Qasabi,
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
Abdominal Solid Organ Injury
 Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
Abdominal Solid Organ Injury 8 th Nordic Course Stockholm, Sweden May 19-22, 2014 K.SHANMUGANATHAN M.D. ABDOMINAL TRAUMA OBJECTIVES Splenic injury Late arterial / early p-v phase imaging Liver injury Blunt
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Medical - Clinical Research & Reviews
 Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Renal Transplant Surgery
 Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
R E V I E W P A P E R S
 POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 11, 554 563 10.2478/v10035-009-0090-1 R E V I E W P A P E R S Surgical management of liver trauma Marek Krawczyk, Piotr Arkuszewski Departament of General, Transplant
POLSKI PRZEGLĄD CHIRURGICZNY 2009, 81, 11, 554 563 10.2478/v10035-009-0090-1 R E V I E W P A P E R S Surgical management of liver trauma Marek Krawczyk, Piotr Arkuszewski Departament of General, Transplant
Management of biliary complications following damage control surgery for liver trauma
 Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
Eur J Trauma Emerg Surg DOI 10.1007/s00068-013-0304-4 ORIGINAL ARTICLE Management of biliary complications following damage control surgery for liver trauma M. Hommes G. Kazemier N. W. L. Schep E. J. Kuipers
Imaging in abdominal trauma
 Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Imaging in abdominal trauma Dilyana Baleva Medical University Varna Landesklinikum Mistelbach-Gänserndorf Learning objectives Definition, demographics and etiology Imaging modalities and protocols Common
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Splenic Injury Evaluation and Management Guideline ADULT Practice Management Guideline Contact: Trauma Center Medical
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY
 CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
CT IMAGING OF BLUNT SPLENIC INJURY: A PICTORIAL ESSAY Radhiana H, Azian AA, Ahmad Razali MR, Amran AR, Azlin S, S Kamariah CM Department of Radiology International Islamic University Malaysia Kuantan,
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Management of traumatic liver injuries, Mafraq hospital experience, UAE
 International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning
 Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D5 Statement on Abdominal Scanning Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA)
") The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
The Management and Treatment of Ruptured Abdominal Aortic Aneurysm (RAAA) Disclosure Speaker name: Ren Wei, Li Zhui, Li Fenghe, Zhao Yu Department of Vascular Surgery, The First Affiliated Hospital of
TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN
 TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN Usman Ali, Ashab Noor, Mian Mujahid Shah*, Waqar Alam Department of Surgery, Postgraduate Medical Institute, Lady Reading Hospital, Peshawar
TRAUMA MANAGEMENT IN A TERTIARY CARE HOSPITAL IN PESHAWAR, PAKISTAN Usman Ali, Ashab Noor, Mian Mujahid Shah*, Waqar Alam Department of Surgery, Postgraduate Medical Institute, Lady Reading Hospital, Peshawar
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
CLINICAL MANAGEMENT GUIDELINE PAGE 1 NO REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12
 CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
CLINICAL MANAGEMENT GUIDELINE PAGE 1 REVISION NO. 1 EFFECTIVE DATE: 03/01/2015 SUPERSEDES: 9/26/12 DEPARTMENT (DIVISION): Trauma TITLE: Management of Abdominal Solid Organ Injuries PURPOSE The vast majority
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Internal Injury Documentation Guidelines
 Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Internal Injury Documentation Guidelines General Open Wound of Thorax Injury to Heart Identify episode of care Initial Subsequent Sequela Laterality Sequela of injury Place of occurrence of injury Activity
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
2014 Deleted CPT Codes
 2014 Deleted CPT Codes Surgery 13150 - Repair, complex, eyelids, nose, ears and/or lips; 1.0 cm or less 19102 - Biopsy of breast; percutaneous, needle core, using imaging guidance 19103 - Biopsy of breast;
2014 Deleted CPT Codes Surgery 13150 - Repair, complex, eyelids, nose, ears and/or lips; 1.0 cm or less 19102 - Biopsy of breast; percutaneous, needle core, using imaging guidance 19103 - Biopsy of breast;
Intra- abdominal Solid Organ Injuries in Blunt Injury Abdomen in Tertiary Care Medical College Hospital, Madurai: A Prospective study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. III (Nov. 2017), PP 46-50 www.iosrjournals.org Intra- abdominal Solid Organ Injuries
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 16, Issue 11 Ver. III (Nov. 2017), PP 46-50 www.iosrjournals.org Intra- abdominal Solid Organ Injuries
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
NYU School of Medicine Department of Radiology Rotation-Specific House Staff Evaluation
 Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Vascular & Interventional Radiology Rotation 1 Core competency in vascular and interventional radiology during the first resident rotation consists of clinical objectives, technical objectives and image
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Index Note: Page numbers of article titles are in boldface type. A Abdominal injuries clinical presentation of, 23 24 Abdominal trauma evaluation for pediatric surgeon, 59 74 background of, 60 colon and
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool
 Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
Delayed Splenic Rupture After Non-Operative Management of Blunt Splenic Injury A AAST Multi-Institutional Prospective Trial Data Collection Tool Enrolling Center: Patient Number (sequential within center):
The Role of the FAST exam in the EDRU
 The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
The Role of the FAST exam in the EDRU A. Robb McLean, MD, MHCM Vice Chair of Clinical Operations, Department of Emergency Medicine Joint Trauma Conference June 20, 2017 Disclosures Goals Describe the performance,
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Pediatric Solid Organ Injury
 Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
Pediatric Solid Organ Injury Grand Rounds St. Charles Medical Center Bend, OR July 20, 2018 Disclosures Disclosure of relevant financial relationships in the past 12 months: I have had no relevant financial
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA. LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital
 MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
MEDICAL MANAGEMENT OF ABDOMINAL TRAUMA LUIS H. TELLO MV, MS, DVM, COS Portland Hospital Classic International Medical Advisor Banfield Pet Hospital ABDOMINAL TRAUMA 70-80% of multiple trauma patients 55%
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Biliary Anatomy in Living-related Liver Transplantation
 The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No