Part 3. Case #7 History:
|
|
|
- Barnaby Nelson
- 6 years ago
- Views:
Transcription


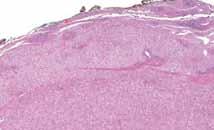
1 Part 3 Case #7 History: The patient is a 25 year old woman who had a colectomy for familial adenomatous polyposis 2 years ago. No carcinoma was found in her colectomy specimen. She presents now with 2 liver masses, suspected clinically to be metastases from an unrecognized colorectal adenocarcinoma, or from another unknown gastrointestinal primary site. The patient takes oral contraceptives. 1

2 2
3 3


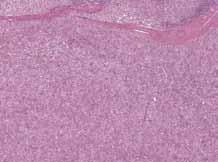
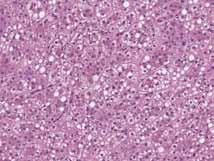
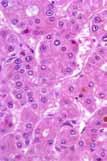
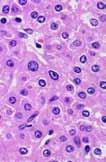
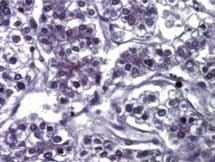
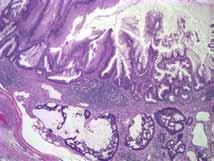
4 Summary: Hepatocellular lesion Sheet-like arrangement of cytologically bland hepatocytes No portal tracts; scattered arteries/arterioles and veins Small, inconspicuous nucleoli No mitoses Summary: Hepatocellular lesion Sheet-like arrangement of cytologically bland hepatocytes No portal tracts; scattered arteries/arterioles and veins Small, inconspicuous nucleoli No mitoses All of this in a young woman, without cirrhosis, taking oral contraceptives. So, this should be a liver cell adenoma. 4
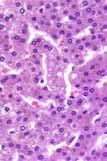
5 On the other hand, there are prominent pseudoglandular spaces, some of them containing bile, unusual in a liver cell adenoma. What is the appropriate classification of this liver nodule? We are all seeing increasing numbers of liver nodules. Why? Worldwide Incidence of Hepatocellular Carcinoma North America has been an area of the world with a relatively low incidence of hepatocellular carcinoma, until recent years 3.3 High (> 30:100,000) Intermediate (3-30:100,000) Low (< 3:100,000) The age-adjusted incidence rates for HCC consecutive 3-year periods between 1976 and 2002 Age-Adjusted Incidence Rate per 100, Year The incidence is expected to increase until 2008, then stay high for 20 years. El-Serag HB, Mason A, N Engl J Med 1999 El-Serag HB et al, Ann Intern Med
6 Only HCV-related HCC Increased Between 1993 and 1998 VA hospitals HCV-related HCC accounted for 50% of the increase Overall only a third of all cases were HCV-related Incidence Hospitalization / 100, El-Serag HB, Mason AC. Arch Intern Med Year HBV HCV ALD Idiopathic Diabetes Is Associated with a Two-fold Increase in Risk of HCC HCC Rate (%) Diabetes P< N=173,643 No Diabetes N=650, Years of Follow up El-Serag HB, Tran T, Everhart JE, Gastroenterology 2004 The increasing incidence of hepatocellular carcinoma in the US is certainly related to increased prevalence of Hepatitis C beginning in the 1960 s and 1970 s, and likely also due to the prevalence of diabetes, obesity and steatohepatitis. More patients undergoing surveillance for HCC Serum AFP Ultrasound 6


7 Algorithm for investigation of mass discovered in a cirrhotic liver Only a subset of masses will be biopsied. Even so, we are seeing more and more challenging biopsies The histologic diagnosis of hepatocellular carcinoma Hepatocellular differentiation Malignant features Classic hepatocellular carcinoma has cells that look like hepatocytes to a variable extent, but has cytologic and architectural abnormalities.. 7



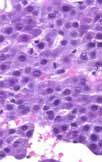
8 Cells resemble hepatocytes, with granular eosinophilic cytoplasm, but have increased nuclear:cytoplasmic ratio. Prominent nucleoli Bile pigment in canaliculi Abnormal, dilated bile canaliculi form pseudoglandular spaces 8



9 Intranuclear cytoplasmic invaginations may be prominent in some cases. The cells of HCC are classically arranged in abnormally wide trabeculae separated by sinusoidlike spaces lined by endothelial cells. Less commonly, the sinusoid-like vascular spaces are compressed, forming a sheet-like pattern. Stroma is usually sparse. 9

10 but occasional cases have sclerotic stroma. The histologic diagnosis of hepatocellular carcinoma a Hepatocellular differentiation Malignant features What is the differential diagnosis for a low grade hepatocellular mass lesion? Dysplastic nodule or macroregenerative nodule in the setting of cirrhosis (surveillance) Adenoma Focal nodular hyperplasia WD HCC How do we tell these apart? 10

11 Well differentiated HCC vs. macroregenerative nodule a common differential in the setting of a patient with cirrhosis who has a nodule detected. Cellular features that favor HCC HCC Increased N:C Often subtle benign Compare to normal liver to see subtle difference Cellular features that favor HCC Macronucleoli Intranuclear cytoplasmic invaginations Even one mitotic figure 11
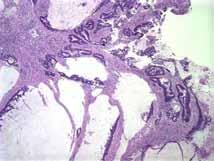
12 Architectural features that favor HCC Thick trabeculae Open, gaping sinusoids Unpaired arteries Pseudoglandular spaces Focal nodular hyperplasia Benign nodules in noncirrhotic liver that must be distinguished from HCC. Liver cell adenoma Focal Nodular Hyperplasia Benign lesion most common in young women Related to altered vasculature a vascular abnormality Not caused by, but may be stimulated to grow by oral contraceptives Central, radiating scar 12


13 Focal Nodular Hyperplasia Normal-appearing hepatocytes in nodules partly surrounded by fibrous bands Bile ductules and thick walled muscular vessels in fibrous tissue Bile ductular proliferation Fibrous bands Not too tough a diagnosis when you see the whole thing.. But much more difficult in a needle biopsy! 13

 or in persons on anabolic steroids Hepatic adenoma Hepatic adenoma Uniform population of hepatocytes that may")
14 Fibrous bands and bile The usual ductules difficulty is distinguishing FNH Clinical setting from cirrhosis in a needle Imaging biopsy, studies when Characteristic the only history enough is that liver distinction biopsy! from HCC is not an issue. Focal Nodular Hyperplasia Rare hepatocellular neoplasm, almost exclusively in young women Rarely occurs in patients with metabolic disorders (tyrosinemia, glycogen storage, familial diabetes mellitus) or in persons on anabolic steroids Hepatic adenoma Hepatic adenoma Uniform population of hepatocytes that may be the same size, larger, or smaller than normal hepatocytes 14



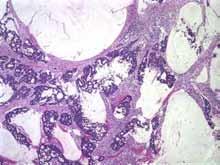
15 Hepatic adenoma Arranged in plates 1 to 3 cells thick Hepatic adenoma Sinusoids separating trabeculae often compressed, giving sheet-like arrangement Hepatic adenoma Usually eosinophilic cytoplasm, sometimes have glycogen or fat 15

16 Vessels of varying size, but no portal tracts Absent mitoses Differentiating adenoma from well differentiated hepatocellular carcinoma Clinical Setting Hepatocellular carcinoma: Older/male patient, with cirrhosis or predisposing condition for HCC Adenoma: Young female patient on OCP, without cirrhosis Differentiating adenoma from well differentiated hepatocellular carcinoma Histology architecture Hepatocellular carcinoma: Thick cords Pseudoglandular spaces Adenoma: 2-3 cell cords Lack of pseudoglandular spaces 16


17 HCC Adenoma Open sinusoids Pseudoglandular spaces No pseudoglandular spaces Compressed sinusoids Adenoma Trabeculae 2-3 cells thick HCC Irregular, wide trabeculae HCC 17


18 The histologic diagnosis of of hepatocellular carcinoma? What immunostains can help in the diagnosis Hepatocellular differentiation Malignant features What immunostains are useful in diagnosing hepatocellular carcinoma? The stains we choose depend on which problem we are facing. This is clearly malignant, but is it hepatocellular? This is clearly hepatocellular, but is it malignant? For the poorly differentiated carcinoma, we would like to prove it is hepatocellular Markers of hepatocytes? Hep Par 1 (hepatocyte paraffin 1) and Hepatocyte recognize an epitope that is part of hepatocyte mitochondria, so marks both normal and neoplastic hepatocytes. About 75% of HCC are positive for Hep Par 1, but carcinomas of other types may also occasionally be positive. Poorly differentiated HCC less likely to be positive. 18


19 Hep Par 1 Variable staining from one field to another. We can take advantage of the fact that only hepatocytes make bile canaliculi. Polyclonal CEA and CD 10 highlight bile canaliculi in normal liver. Bile canalicular staining is present in some cases of HCC unfortunately, not always the poorly differentiated ones! In normal liver polyclonal CEA highlights the bile canaliculi between hepatocytes 19
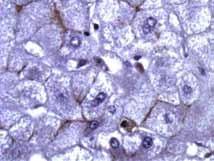
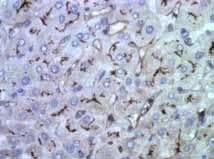
20 CD 10 immunostain does the same thing, only better! pcea in HCC 20




21 CD 10 in HCC In poorly differentiated HCC, bile canalicular staining with pcea can be very focal. The CD 10 is often works better than pcea to find bile canalicular staining. 21


22 Be aware, though, that CD 10 (and sometimes pcea) may stain the entire periphery of cells, looking like a membranous staining pattern. This membranous pattern has been noted in as many as a third of HCC! For the very well differentiated carcinoma, we would like to prove it is neoplastic. In benign liver, the sinusoids are lined by specialized endothelial cells. They lack basement membrane. They are also CD 34 negative. 22



23 CD 34 in non-neoplastic liver The cells lining the sinusoid-like spaces in HCC are endothelial cells without these specialized features. They stain with CD 34. Sometimes they stain diffusely. 23

 3 (43) 0 (0) Extremely well-differentiated HCC (n=10) 5 (50) 2 (20) HCC, well differentiated (n=16) b 9 (56) 5 (31) HCC, moderately differentiated (n=18) 15 (83) 10 (56) HCC, poorly")
24 Sometimes the stain is patchy. Liver cell adenomas may also have patchy CD 34 positivity. So, sinusoidal CD 34 positivity can support the lesion being neoplastic, but not necessarily malignant. Glypican-3 is a new antibody touted as specific for HCC Best for identifying poorly differentiated carcinoma in liver as HCC Liver lesions GPC-3 staining a Total positive Diffuse positive Benign hepatocellular lesions Cirrhotic nodules (n=35) 4 (11) 0 (0) Macroregenerative nodule (n=10) 0 (0) 0 (0) Hepatic adenoma (n=8) 0 (0) 0 (0) Borderline and malignant lesions High-grade dysplastic nodule (n=7) 3 (43) 0 (0) Extremely well-differentiated HCC (n=10) 5 (50) 2 (20) HCC, well differentiated (n=16) b 9 (56) 5 (31) HCC, moderately differentiated (n=18) 15 (83) 10 (56) HCC, poorly differentiated (n=24) 22 (89) 20 (83) Fibrolamellar HCC (n=11) 7 (64) 4 (36) HCC, hepatocellular carcinoma. a Figures in parenthesis reflect percentages. b Includes extremely welldifferentiated HCC. Shafizadeh N, et al. Mod Pathol 2008;21:
25 A panel of 3 immunohistochemical stains has recently been promoted as useful in the distinction of HCC from regenerative and dysplastic nodules in the setting of cirrhosis. Heat Shock Protein 70 Glypican 3 Glutamine Synthetase The percentages differ by study, but each of these has a 30-70% rate of positivity in HCC, but less than 10% positivity in dysplastic or regenerative nodules. Diagnostic accuracy of a panel of HSP 70, GPC 3, and GS in benign and malignant nodules (study did not include adenomas). At least 1 + At least 2 + All 3 + Benign nodule N=84 Malignant nodule N= Di Tommaso L, et al. J of Hepatol 2009;50; I can find varying results for each of these in adenomas HSP 70 usually negative, others variable, depending on study. Notes on other immunostains: AFP: So insensitive as to be useless we never order it MOC 31: + in most adenocarcinomas, including cholangioca, rarely + in HCC CK 5/6: + in about half of pancreatic adenoca, and 20% of cholangioca, negative in HCC 25
26 Notes on other immunostains: p63: Positive in cholangiocarcinoma p53: positive in 35% of HCC; negative in benign liver Proliferation markers (Ki-67): useful in diagnosing carcinoma if >15-20% of nuclei are positive How grade hepatocellular neoplasm in young woman on oral contraceptives.should be a liver cell adenoma. Sheet-like arrangement of bland hepatocytes should be an adenoma. 26


27 What about the history of colectomy for familial adenomatous polyposis? Are there any immunostains that might help? Hepatocellular differentiation Malignant features Hepatocyte/HepPar1 pcea/cd10 CD 34? p53? Ki67? Ki67? 27

28 Given the history of a risk factor for hepatocellular neoplasm, and the prominent pseudoglandular spaces: Diagnosis: Well-differentiated hepatocellular carcinoma. Case # 8 History: A patient presented with signs and symptoms of acute appendicitis. The surgeon found a large, cystically dilated appendix with mucus adherent to the tip, mucus in the pelvis surrounding the right fallopian tube and ovary, and small mucus implants on the serosa of the small bowel. She performed an appendectomy, and right salpingooophorectomy, and biopsied several of the peritoneal implants. 28


29 The dilated appendix Many, many sections of appendiceal wall are examined. 29


30 Big, dilated lumen, mostly surrounded by fibrous wall. Epithelium lining still present here and there. Most of the epithelium is pretty bland. 30


31 But, in some areas there is epithelium that is more atypical. On one slide there are irregularly shaped tubules in the appendiceal wall. tubules in the appendiceal wall 31


32 with epithelium mucus adhering to pelvic adnexa The epithelium in this pelvic mucus is bland, like most of the epithelium in the appendix. My first dilemma: What is the name for this neoplasm? Depending on the book or paper I read, I might consider a number of ways to sign out this case 32




33 Appendiceal adenocarcinoma with peritoneal carcinomatosis Mucinous cystadenoma of the appendix with pseudomyxoma peritonei Disseminated peritoneal adenomucinosis Low grade mucinous neoplasm of the appendix with peritoneal spread Appendiceal mucinous neoplasm of uncertain malignant potential (UMP) What is the correct name? This is clearly a mucinous neoplasm of the appendix with spread to the peritoneal cavity. What do we know about appendiceal mucinous neoplasms? This is a typical example Let s sample the wall 33



34 First 5 blocks Typical mucus extravasation rxn 10 blocks later Eventually. Characteristic appendiceal adenomatous epithelium 34




35 Undulating surfaces Tall cells with abundant cytoplasmic mucin Circumferential proliferation villi Progressive dilatation 35



36 Replacement of lamina propria, lymphoid follicles, muscularis mucosae, submucosa, muscularis propria by collagen Low grade epithelium High grade epithelium 36


37 This is an example of the adenomacarcinoma sequence. Low-grade High-grade Adenoma Carcinoma Extravasated mucus on the tip. 37


38 This might be just mucus. or could include epithelium How does the mucus get there? 2 routes. Mucus tracking throughout dilated, thinned wall 38



39 All the way to the peritoneal surface OR By way of an appendiceal diverticulum. lumen There is an association between appendiceal mucinous neoplasms and diverticula... Diverticulum May rupture and result in spread of mucinous neoplasm to peritoneal surfaces. 39



40 Then how do we recognize invasive carcinoma? Desmoplastic stromal reaction 40


41 High grade epithelium floating in mucin pools Naked neoplastic tubules imbedded in the muscular wall without desmoplasia? This can be diagnostically tough. The surgeon found: Mucinous neoplasm on ovary Where is the primary? And mucin on small bowel serosa. Mucinous neoplasm in appendix 41
42 Mucinous tumors in both appendix and ovary: which is the primary? 7 studies between 1991 and 1999 Looking at synchronous mucinous tumors of ovary and appendix, many with pseudomyxoma peritonei: Based on clinicopathologic and immunohistochemical data, all but one conclude that appendix is by far the most common primary site. Mucinous tumors in both appendix and ovary: which is the primary? 7 studies between 1991 and 1999 Looking at synchronous mucinous tumors of ovary and appendix, many with pseudomyxoma peritonei: Genetic studies among these confirm that, in almost all cases, these synchronous tumors are the same. Appendiceal Mucinous Neoplasms how do they behave? # Epithelium Peritoneal spread LAMN 88 Low grade MACA 16 High grade Discordant 3 LG in app HG in perit Survival with peritoneal spread 3 year 5 year 10 year 56% 100% 86% 45% 75% 90% 44% No data All No data LAMN : low But grade stage appendiceal is important mucinous too: neoplasm MACA: mucinous adenocarcinoma No pt with LAMN confined to the appendix died. 2 of 3 with LAMN and localized periapp spread died. Misdraji, et al, Am J Surg Pathol, 27:1089,
43 What about the peritoneal mucin and epithelium in our case? Pseudomyxoma peritonei (literally means 'false mucinous tumor of the peritoneum') is described as a slowly progressive disease process characterized by copious amounts of mucoid fluid and tumor that, over time, fills the peritoneal cavity. What happens to patients with Pseudomyxoma Peritonei? 108 of 109 cases with epithelium, not all appendiceal DPAM (low grade) PMAC (high grade) Epithelium App primary Organ invasion Scant, low grade like app adenoma Abundant, high grade or carcinoma 57% known 43% c/w appendix 40% known 43% colon 12% usually ovary 97% Intestine Ovary Nodal Mets 5 yr survival 3% 84% 50% 7% Indeterminant Mixed 79% 79% 21% 38% DPAM: diffuse peritoneal adenomucinosis PMAC: peritoneal mucinous adenocarcinoma Ronnett, et al, Am J Surg Pathol, 19:1398,
44 Patients with appendiceal mucinous neoplasms with localized extra-appendiceal mucin devoid of epithelium are unlikely to develop disseminated peritoneal disease and do not die of their disease. However, even scant mucin present in such deposits indicates the patient is at risk to develop disseminated disease and die from disease. Submit all extracellular mucin from such localized deposits to examine for presence of epithelium! Yantiss RK, et al. Ruptured appendiceal mucinous neoplasms: prognostic significance of localized extra-appendiceal mucin deposition Mod Pathol 2008;21(Suppl 1):142A Conclusions based on these studies: Low grade appendiceal mucinous neoplasms are likely to stay confined to the appendix, or may spread to peritoneal surfaces. They have a good prognosis. High grade appendiceal mucinous neoplasms are likely to spread to the peritoneum and have a worse prognosis. Conclusions based on these studies: Pseudomyxoma peritonei with low grade epithelium has a protracted clinical course. Pseudomyxoma peritonei with high grade (carcinomatous) epithelium has a bad prognosis. What does this suggest about our case? 44
45 In our case the appendiceal tip was dilated and filled with mucus and there was a partial epithelial lining. Most of the epithelium was low grade (good prognosis) but some was high grade.. (bad prognosis) 45
 There was also peritoneal mucus with")

46 There were invasive tubules in the wall. (bad prognosis) There was also peritoneal mucus with strips of low grade epithelium (bad) Is this a good prognosis or a bad prognosis case? Peritoneum and appendix Appendix 46
47 Diagnosis: Appendix, resection: Low grade appendiceal mucinous neoplasm, with extra-appendiceal mucin (pseudomyxoma peritonei), containing low grade neoplastic epithelium. Terminologies for neoplastic peritoneal mucin accumulations Pseudomyxoma peritonei Disseminated peritoneal adenomucinosis (DPAM) and Peritoneal mucinous carcinomatosis (PMCA) Mucinous adenoma/ neoplasm of uncertain malignant potential/ neoplasm of uncertain malignant potential/ carcinoma Where did the term Pseudomyxoma peritonei come from? Werth, in 1884, first described pseudomyxoma peritonei as the presence abundant gelatinous material in the peritoneal cavity as a result of perforation of an ovarian mucinous cystadenoma. Frankel, in 1901, described the association of PMP with a ruptured mucocele of the appendix. 47
48 Pseudomyxoma peritonei What s wrong with this term? The term has been used too broadly, to include low grade appendiceal neoplasm, neoplasms from other sites, and also mucinous carcinomas. It does not sufficiently describe the findings. Solution: Invent new terms! DPAM and PMCA Disseminated peritoneal adenomucinosis Peritoneal mucinous carcinomatosis Ronnett and colleagues classified 109 cases of multifocal peritoneal mucinous tumors according to a set of criteria. Ronnett BM, Zahn CM, Kurman RJ, Kass ME, Sugarbaker PH, Shmookler BM. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to pseudomyxoma peritonei. AJSP 1995;19(12): DPAM disseminated peritoneal adenomucinosis A clinicopathologic entity characterized by mucinous ascites and noninvasive mucinous implants with a characteristic distribution and containing histologically benign mucinous epithelium derived from an appendiceal mucinous adenoma and having an indolent course. 48

49 DPAM disseminated peritoneal adenomucinosis Peritoneal mucin Low grade epithelium Noninvasive implants Appendiceal adenoma 49
 epithelium Invasion Appendiceal or intestinal mucinous adenocarcinoma")
50 PMCA Peritoneal mucinous carcinomatosis cases with histologically malignant peritoneal tumors derived from appendiceal or intestinal mucinous carcinomas PMCA Peritoneal mucinous carcinomatosis Peritoneal mucin High grade (carcinomatous) epithelium Invasion Appendiceal or intestinal mucinous adenocarcinoma 50
51 51
52 DPAM 65 cases 8 parenchymal organ invasion 7 ovary 1 bowel wall 2 lymph node involvement 1 extra-abdominal disease 84% age-adjusted 5 year survival PMCA 30 cases 29 parenchymal organ invasion 11 ovary, 17 bowel wall, 4 liver, 1 uterus 15 lymph node involvement 0 extra-abdominal disease 6.7% age-adjusted 5 year survival Terminology akin to that for ovarian surface epithelial tumors Mucinous adenoma Sessile, circumferential, not extending through wall or present in peritoneum Simple to stratified columnar cells, slight to moderate cytologic atypia Appendix dilated, may perforate and extravasate mucin Clinically benign Pai RK, Longacre TA. Appendiceal mucinous tumors and pseudomyxoma peritonei. Histologic features, diagnostic problems, and proposed classification. Adv Anat Pathol 2005;12: Terminology akin to that for ovarian surface epithelial tumors Mucinous neoplasm of uncertain malignant potential Features of mucinous adenoma, but.. Proximal margin involved, or Epithelium in wall, but not clearly invasive, or Uncertain if epithelium in peritoneal mucin Clinical behavior uncertain 52
53 Terminology akin to that for ovarian surface epithelial tumors Mucinous neoplasm of low malignant potential Features of mucinous adenoma, but.. Neoplastic cells penetrate wall and are present in peritoneal mucin Abundant peritoneal mucin, may be extensive, but. No lymph node, lung, liver mets Protracted clinical course Terminology akin to that for ovarian surface epithelial tumors Mucinous adenocarcinoma Infrequently associated with PMP when present should be called peritoneal carcinomatosis Cytoarchitectural features of frank carcinoma Lymph node, lung, liver mets Clinically malignant with poor prognosis DPAM PMCA MNUMP MNLMP PMP 53
54 Peritoneal mucin accumulations with low grade epithelium are primarily treated surgically, often followed by various types of chemotherapy So, what language do the surgeons understand? PubMed search using terms Appendiceal mucinous neoplasms peritoneal Peritoneal adenomucinosis Looking for the diagnostic terms used in article titles PMP 20 Descriptive 8 DPAM 3 Subtract pathology journals PMP 17 Descriptive 8 DPAM 2 My conclusion: (yours may be different) Tell them exactly what is there descriptively Grade of neoplasm in appendix Grade of epithelium in peritoneal mucin The term pseudomyxoma peritonei should appear somewhere in the report for low grade lesions, since that is what the surgeons call it. The term carcinoma or carcinomatosis should appear for high grade (carcinomatous) cases 54



55 Case #9 An appendectomy specimen in a patient with appendicitis-like symptoms: At low power there are pale areas in the thick muscularis propria Clusters of goblet cells mixed with other cells 55



56 Paneth cells Nests of cells that look endocrine This is an uncommon component of such neoplasms. Chromogranin immunostain 56
 for this is")

57 Neurotropism Many names have been used or proposed for this tumor: Adenocarcinoma Goblet cell carcinoid tumor Mucinous carcinoid Intermediate type of carcinoid Crypt cell carcinoma Microglandular carcinoma Adenocarcinoid tumor Carcinoid tumor NOS The accepted name (WHO) for this is Goblet cell carcinoid tumor Patients generally present with acute appendicitis, and neoplasm is seldom suspected preoperatively. Some examples are so small and subtle that it is easy to miss them. Calling this a carcinoid tumor contributes to confusion as to its significance and management. 57

58 Goblet cell carcinoid tumor of the appendix Is this a type of carcinoid tumor, a type of adenocarcinoma, or what? How does it behave? Endocrine cells are a minor component of this tumor There are 3 questions that often are asked when these tumors are found: 1. Is this really a type of carcinoid tumor? 2. How will it behave? 3. Should a more extensive resection be done, and under what circumstances? Ideally, we would answer these questions using solid data. 58


59 Until recently, most of the literature about this tumor consists of case reports or tiny series, as well as a few review articles by surgeons who did not understand the histologic variations. The first question. Is this really a carcinoid tumor? WHO classifies this as an endocrine tumor Why has it been categorized this way? Is this really a carcinoid tumor? Its presence at the base of the mucosa is taken as evidence that it originates in the mucosa (like a carcinoid tumor). 59


60 Is this really a carcinoid tumor? There are endocrine cells, but they are never the dominant cells; they are always a distant second to the goblet cells. Is this really a carcinoid tumor? Goblet cell carcinoids share a number of genetic abnormalities with ileal carcinoid tumors, including allelic loss of chromosomes 11q, 16q, and 18q, suggesting similar events in the pathogenesis of these tumors. Stancu M, Wu TT, Wallace C, Houlihan PS, Hamilton SR, Rashid A. Genetic alterations in goblet cell carcinoids of the vermiform appendix and comparison with gastrointestinal carcinoid tumors. Mod Pathol Dec;16(12): In fact, these are heterogeneous tumors One of the proposed names: Crypt cell carcinoma that differentiate along a number of epithelial lines 60

61 However, WHO classifies this as an endocrine tumor and calls it goblet cell carcinoid But it has some adenocarcinoma-like features: Mucin production Paneth cells A propensity for spread to ovaries and peritoneal surfaces May cause death! So, if this tumor can be aggressive.. What is known about the long term results following appendectomy? Two large studies have dealt with this issue: The authors identify 2 types of goblet cell carcinoid tumors, a pure form and a form that had a mixture of pure areas and carcinoma. 61

62 Goblet cell carcinoid with adenocarcinoma Goblet cell Carcinoids and Related Tumors Type Extent Mets Outcome Pure GCC App NO A & W Mixed GCC/Adenoca App/Invasion Yes 80% Fatal AdenoCA Burke, et al, Am J Clin Pathol. 94:27-35, 1990 Study of 63 cases of appendiceal goblet cell carcinoid tumor Goblet Cell Carcinoid Adenocarcinoma Ex GCC, Moderately Differentiated Adenocarcinoma Ex GCC, Poorly Differentiated by Tang, et al, from MSK and AFIP MORPHOLOGIC CRITERIA FOR CLASSIFICATION Well differentiated goblet cells arranged in clusters or in a linear pattern Minimal cytologic atypia Minimal desmoplasia Degenerative change with extracellular mucin is acceptable Recognizable GCC tumor cells arranged or fused into irregular clusters; Recognizable GCC tumor cells with easily identifiable single file or single cell infiltration Significant cytologic atypia Marked desmoplasia Requires at least focal evidence of goblet cell morphology A component (> 1 high power field or >0.5 mm 2 ) is not otherwise distinguishable from a poorly adenocarcinoma confluent sheets of signet ring cells or undifferentiated cells malignant cribriform glands or glandular epithelium 62
63 Study of 63 cases of appendiceal goblet cell carcinoid tumor by Tang, et al, from MSK and AFIP N Mean F/U (mo) Mean survival (mo) NED AWD DOD All (46%) 19 (31%) 14 (23%) GCC (86%) 3 (11%) 1 (4%) WD Ca ex GCC (15%) 15 (58%) 7 (27%) PD Ca ex GCC (0%) 1 (14%) 6 (86%) 30 cases of appendiceal goblet cell carcinoids that presented with ovarian metastases 25 involved both ovaries, and all were large masses Appendices all had transmurally invasive tumors All had mixed patterns, including GCC pattern and adenocarcinoma Follow up on 25 patients: 17 DOD, 8 AWD Median survival 19 months 1- and 2-year survival rates 63% and 34% Conclusion: Should be reported as metastatic appendiceal adenocarcinomas, rather than GCC to reflect prognosis This means that high grade, high stage tumors have a bad prognosis. Hristov AC, et al. Ovarian metastases of appendiceal tumors with goblet cell carcinoidlike and signet ring cell patterns: a report of 30 cases. AJSP 2007 Oct;31(10): Stage matters,too: Mayo Clinic study of 57 patients with goblet cell carcinoid 5 year survival (%) Recurrence rate (%) Stage I 100 Stage II 76 Stage III 22 Stage IV 14 T 1 or 2 0 T 3 33 T 4 71 Pham, et al. Surgical and chemotherapy treatment outcomes of goblet cell carcinoid: a tertiary cancer center experience. Ann Surg Oncol 2006;13:


64 Pure low grade GCC confined to the appendix do very well. GCC that have a component of frank adenocarcinoma, and those that are advanced at presentation do worse. If it looks like a duck, and quacks like a duck, then it must be a duck! The third question Should a more extensive resection be done, and, if so, under what circumstances? This is a great question and one that commonly accompanies our consults on this tumor. Unfortunately, there are no hard data and no controlled studies. The primary treatment is surgical. Which patients need a hemicolectomy is the issue, and there are no universally accepted guidelines. 64
 Clear adenocarcinomatous")
65 Which patients require a hemicolectomy? In general, there seems to be consensus on the following: Extension outside appendix (no clear appendiceal margin, peritoneal or ovarian involvement, lymph node mets) Clear adenocarcinomatous component Undifferentiated cuboidal cells What do we need to tell the surgeon about a goblet cell carcinoid? Pure GCC or adenocarcinoma TNM Appendiceal margin Other staging information, if we have the tissue: lymph nodes, ovaries, peritoneal spread 65

66 66
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Chapter 6 Frozen Section Evaluation of the Appendix
 Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
Chapter 6 Frozen Section Evaluation of the Appendix Abstract Appendiceal tumors are rarely diagnosed preoperatively, and their classification is both challenging and controversial owing to their tendency
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Despite advances in our understanding of appendiceal. An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms
 REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
REVIEW ARTICLE An Update on the Diagnosis, Grading, and Staging of Appendiceal Mucinous Neoplasms Mark A. Valasek, MD, PhD* and Reetesh K. Pai, MD Abstract: Despite advances in our understanding of appendiceal
Pitfalls in the diagnosis of well-differentiated hepatocellular lesions
 2013 Colorado Society of Pathology Pitfalls in the diagnosis of well-differentiated hepatocellular lesions Sanjay Kakar, MD University of California, San Francisco Outline Hepatocellular adenoma: new WHO
2013 Colorado Society of Pathology Pitfalls in the diagnosis of well-differentiated hepatocellular lesions Sanjay Kakar, MD University of California, San Francisco Outline Hepatocellular adenoma: new WHO
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
PATHOLOGY OF LIVER TUMORS
 PATHOLOGY OF LIVER TUMORS Pathobasic, 31.05.2016 WHO Classification Approach to a Liver Mass Lesion in a patient with chronic liver disease? Lesion in a patient without chronic liver disease? Malignant
PATHOLOGY OF LIVER TUMORS Pathobasic, 31.05.2016 WHO Classification Approach to a Liver Mass Lesion in a patient with chronic liver disease? Lesion in a patient without chronic liver disease? Malignant
Pathological Classification of Hepatocellular Carcinoma
 3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
3 rd APASL Single Topic Conference: HCC in 3D Pathological Classification of Hepatocellular Carcinoma Glenda Lyn Y. Pua, M.D. HCC Primary liver cancer is the 2 nd most common cancer in Asia HCC is the
Liver Specialty Evening Conference. Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle
 Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case
 Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Surg Today (2001) 31:646 650 Disseminated Peritoneal Adenomucinosis Associated with a Panperitonitis-Like Onset: Report of a Case Yoshito Kuroki 1, Shunyou Otagiri 1, and Kazuhiro Tsukada 2 1 Department
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Basic Data. Birthday: Gender:Female Admission date:
 Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
O Farrell Legacy UPDATE ON WHO NOMENCLATURE. World Health Organization, 2010 DISCLOSURES WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS
 O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
O Farrell Legacy UPDATE ON WHO NOMENCLATURE WITH EMPHASIS ON PROBLEM HEPATOCELLULAR TUMORS Linda Ferrell, MD University of California San Francisco Vice Chair, Director of Surgical Pathology World Health
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Synonyms. Nephrogenic metaplasia Mesonephric adenoma
 Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
Nephrogenic Adenoma Synonyms Nephrogenic metaplasia Mesonephric adenoma Definition Benign epithelial lesion of urinary tract with tubular, glandular, papillary growth pattern Most frequently in the urinary
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei
 and Cytoreductive Surgery for treatment of Pseudomyxoma Peritonei") Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Specialised Services Policy: CP02 Hyperthermic Intraperitoneal Chemotherapy (HIPEC) of Pseudomyxoma Peritonei Document Author: Assistant Medical Director Executive Lead: Medical Director Approved by: Management
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays
 2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
2018 Current Issues in Surgical Pathology Summary (not actual lecture) Intrahepatic cholangiocarcinoma Histologic spectrum, novel markers and molecular assays Sanjay Kakar, MD University of California,
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Neoplasms of the Canine, Feline and Lemur Liver:
 Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Neoplasms of the Canine, Feline and Lemur Liver: Classification and Prognosis Annual Seminar of the French Society of Veterinary Pathology John M. Cullen VMD PhD DACVP North Carolina State University Primary
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Mucinous tumours of appendix and ovary: an overview and evaluation of current practice
 Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Department of Pathology, Laboratory Medicine Program, University Health Network, University of Toronto, Toronto, Canada Correspondence to Dr Marjan Rouzbahman, Department of Pathology, 11th floor, Eaton
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Biliary tract tumors
 Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
Short Course 2010 Annual Fall Meeting of the Korean Society for Pathologists Biliary tract tumors Joon Hyuk Choi, M.D., Ph.D. Professor, Department of Pathology, Yeungnam Univ. College of Medicine, Daegu,
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Outline. Hepatocellular Carcinoma Histologic variants. HCC: Histologic variants
 2018 Park City AP Update Hepatocellular Carcinoma Histologic variants Sanjay Kakar, MD University of California, San Francisco Outline Histologic variants of HCC Morphologic and Immunohistochemical pitfalls
2018 Park City AP Update Hepatocellular Carcinoma Histologic variants Sanjay Kakar, MD University of California, San Francisco Outline Histologic variants of HCC Morphologic and Immunohistochemical pitfalls
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Papillary Lesions of the Breast A Practical Approach to Diagnosis. (Arch Pathol Lab Med. 2016;140: ; doi: /arpa.
 Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Papillary Lesions of the Breast A Practical Approach to Diagnosis (Arch Pathol Lab Med. 2016;140:1052 1059; doi: 10.5858/arpa.2016-0219-RA) Papillary lesions of the breast Span the spectrum of benign,
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Detection and Characterization of Hepatocellular Carcinoma by Imaging
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S136 S140 Detection and Characterization of Hepatocellular Carcinoma by Imaging OSAMU MATSUI Department of Imaging Diagnosis and Interventional Radiology,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S136 S140 Detection and Characterization of Hepatocellular Carcinoma by Imaging OSAMU MATSUI Department of Imaging Diagnosis and Interventional Radiology,
Invited Re vie W. Analytical histopathological diagnosis of small hepatocellular nodules in chronic liver diseases
 Histol Histopathol (1 998) 13: 1077-1 087 http://www.ehu.es/histoi-histopathol Histology and Histopathology Invited Re vie W Analytical histopathological diagnosis of small hepatocellular nodules in chronic
Histol Histopathol (1 998) 13: 1077-1 087 http://www.ehu.es/histoi-histopathol Histology and Histopathology Invited Re vie W Analytical histopathological diagnosis of small hepatocellular nodules in chronic
Adenocarcinoma of the Cervix
 Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Question 1. Each of the following statements about cervical adenocarcinoma is true except: Adenocarcinoma of the Cervix SAMS a) A majority of women with cervical adenocarcinoma have stage I tumors at diagnosis.
Papillary Lesions of the Breast
 Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
Papillary Lesions of the Breast Laura C. Collins, M.D. Associate Professor of Pathology Associate Director, Division of Anatomic Pathology Beth Israel Deaconess Medical Center and Harvard Medical School
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee
 TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
Gastric and Oesophageal Neuroendocrine tumours. Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath
 Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
Gastric and Oesophageal Neuroendocrine tumours Dr Tim Bracey, Consultant Pathologist MBChB PhD MRCS FRCPath Intestinal (and BO) endocrine cells in crypt bases NE cell (granules towards vessels) Paneth
XIII. Tumours of the liver and biliary system
 XIII. Tumours of the liver and biliary system V. PONOMARKOV 1 & L. J. MACKEY 2 In this histological classification of liver and gall bladder tumours the tumour types largely correspond to those found in
XIII. Tumours of the liver and biliary system V. PONOMARKOV 1 & L. J. MACKEY 2 In this histological classification of liver and gall bladder tumours the tumour types largely correspond to those found in
number Done by Corrected by Doctor Maha Shomaf
 number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
number 16 Done by Waseem Abo-Obeida Corrected by Zeina Assaf Doctor Maha Shomaf MALIGNANT NEOPLASMS The four fundamental features by which benign and malignant tumors can be distinguished are: 1- differentiation
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Alastair Burt Newcastle University
 Alastair Burt Newcastle University Benign Hepatocellular adenoma 8170/0 Focal nodular hyperplasia Malignancy-associated and premalignant lesions Large cell change (formerly dysplasia ) Small cell change
Alastair Burt Newcastle University Benign Hepatocellular adenoma 8170/0 Focal nodular hyperplasia Malignancy-associated and premalignant lesions Large cell change (formerly dysplasia ) Small cell change
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis.
 Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Fig. 59 Malignant phaeochromocytoma, hepatic metastasis. X 120 Hyperte nsion Fig. 60 Malignant sympathetic paraganglioma, lymph node metastasis Primary in bladder. x 1 20 Hypertension Fig. 61 Malignant
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
Papillary Lesions of the Breast: WHO Update
 Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Papillary Lesions of the Breast: WHO Update Stuart J. Schnitt, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA, USA Papillary Lesions of the Breast
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm
 Mitchell et al. Diagnostic Pathology 2014, 9:39 CASE REPORT Open Access Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm Andrew Mitchell
Mitchell et al. Diagnostic Pathology 2014, 9:39 CASE REPORT Open Access Dysplastic intestinal-type metaplasia of appendiceal endometriosis: a mimic of low grade appendiceal mucinous neoplasm Andrew Mitchell
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT
 Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Case: The patient is a 62 year old woman with a history of renal cell carcinoma that was removed years ago. A 2.4 cm liver mass was found on CT during follow- up. ALT, AST, Alk Phos and bilirubin were
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Video Microscopy Tutorial 8
 Video Microscopy Tutorial 8 Common and Uncommon Lesions of the Liver Gladwyn Leiman, MD There are no disclosures necessary. Common and Uncommon Lesions in Liver FNA Gladwyn Leiman University of Vermont
Video Microscopy Tutorial 8 Common and Uncommon Lesions of the Liver Gladwyn Leiman, MD There are no disclosures necessary. Common and Uncommon Lesions in Liver FNA Gladwyn Leiman University of Vermont
بسم هللا الرحمن الرحيم. Prof soha Talaat
 بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Raga Ramachandran, MD, PhD Assistant Professor and Director of Medical Education, UCSF Pathology
 Variants of Hepatocellular Carcinoma: Practical Issues Raga Ramachandran, MD, PhD Assistant Professor and Director of Medical Education, UCSF Pathology raga.ramachandran@ucsf.edu A full copy of the presentation
Variants of Hepatocellular Carcinoma: Practical Issues Raga Ramachandran, MD, PhD Assistant Professor and Director of Medical Education, UCSF Pathology raga.ramachandran@ucsf.edu A full copy of the presentation
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Colon and Rectum: 2018 Solid Tumor Rules
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Colon and Rectum: 2018 Solid Tumor Rules 1 Colon and Rectum Solid Tumor Rules Separate sections for: Introduction Changes from 2007 MP/H rules Equivalent
NEOPLASMS AND TUMOR-LIKE CONDITIONS OF LIVER
 NEOPLASMS AND TUMOR-LIKE CONDITIONS OF LIVER Epithelial Tumors Focal nodular hyperplasia Focal nodular hyperplasia is a localized hyperplasic overgrowth of hepatocytes around a vascular anomaly, particularly
NEOPLASMS AND TUMOR-LIKE CONDITIONS OF LIVER Epithelial Tumors Focal nodular hyperplasia Focal nodular hyperplasia is a localized hyperplasic overgrowth of hepatocytes around a vascular anomaly, particularly
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor
 of the Ovary Arising in an Atypical Proliferative Serous Tumor") Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
ONCOLOGY. Csaba Bödör. Department of Pathology and Experimental Cancer Research november 19., ÁOK, III.
 ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
ONCOLOGY Csaba Bödör Department of Pathology and Experimental Cancer Research 2018. november 19., ÁOK, III. bodor.csaba1@med.semmelweis-univ.hu ONCOLOGY Characteristics of Benign and Malignant Neoplasms
04/09/2018. Follicular Thyroid Tumors Updates in Classification & Practical Tips. Dissecting Indeterminants. In pursuit of the low grade malignancy
 Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a
 G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
G3.02 The malignant potential of the neoplasm should be recorded. CG3.02a Conventional adrenocortical neoplasm. Each of the below parameters is scored 0 when absent and 1 when present. 3 or more of these
Atypical Well differentiated Hepatocellular Neoplasms Cruising through the maze of criteria, terminology and risk assessment
 2016 Hans Popper Companion Meeting Atypical Well differentiated Hepatocellular Neoplasms Cruising through the maze of criteria, terminology and risk assessment Disclosure Dr. Kakar has nothing to Disclose
2016 Hans Popper Companion Meeting Atypical Well differentiated Hepatocellular Neoplasms Cruising through the maze of criteria, terminology and risk assessment Disclosure Dr. Kakar has nothing to Disclose
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS
 USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Division of Gynecologic Pathology The Johns Hopkins Hospital Table of contents: Powerpoint handout Text
USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Division of Gynecologic Pathology The Johns Hopkins Hospital Table of contents: Powerpoint handout Text
LIVER IMAGING TIPS IN VARIOUS MODALITIES. M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly
 LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary