Problems with ARDS Trials: Time for more splitting and less lumping?
|
|
|
- Janis Warner
- 5 years ago
- Views:
Transcription
1 Problems with ARDS Trials: Time for more splitting and less lumping? B. Taylor Thompson MD Massachusetts General Hospital Professor of Medicine, Harvard Medical School
2 ARDS Disclosures Lilly - Co-PI, PROWESS-SHOCK Astra Zeneca - DSMB Chair, Cytofab for sepsis Hemodec - Co I, ECCO2R for severe ARDS US Biotest - ARDS
3 Problems ARDS Trials? Nitric oxide Surfactant Perflourocarbon Corticosteroids Prostaglandin E1 Lysophylline Ibuprofen Procysteine Ketoconazole Streptokinase Neutrophil elastase inhibitor spla 2 Inhibitor rhapc Albuterol/salmeterol Lower Vt? Furosemide (FACTT) Cisatricurium NEGATIVE TRIALS POSITIVE TRIALS
4 Still trying: current/recently completed trials 1. Surfactant Calfactant (Willson, n=480) 2. VIP (Said, Phase I) 3. Corticosteroids (Antonelli, n=400) 4. VEGF (Kaner, Phase II) 5. Tenecteplase (Ashley, Genentec, Phase II) 6. Rosuvastatin (SAIL, ARDSnet, Phase III, n=1000) 7. Others 170 trials on ClinTrials.gov!
5 Success in science is defined as moving from failure to failure with undiminished enthusiasm Winston Churchill
6 Problems with ARDS Trials ARDS is a Syndrome What are we studying? Do we really know if these drugs truly failed? Are we measuring the right outcomes?
7 THE CONCEPTUAL MODEL OF ARDS 1. ARDS is a type of acute diffuse lung injury associated with recognized risk factors, characterized by inflammation leading to increased pulmonary vascular permeability and loss of aerated lung tissue. 2. The hallmarks of the clinical syndrome are hypoxemia and bilateral radiographic opacities (standard chest x-ray or CT scan). Ranieri ESICM and CCCF, Proposed Berlin Definition of ARDS
8 ARDS Mild Moderate Severe Timing Acute onset within 1 week of a known clinical risk factor or new/worsening respiratory symptoms Hypoxemia PaO 2 /FiO with PEEP/CPAP 5 PaO 2 /FiO with PEEP 5 PaO 2 /FiO with PEEP 10 Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload** Radiological Abnormalities Bilateral opacities* Bilateral opacities* Opacities involving 3 + quadrants* Additional Physiological Derangement N/A N/A V E Corr > 10 L/min or C RS <40 ml/cmh 2 O *Not fully explained by effusions, nodules, masses, or lobar/lung collapse; use training set of CXRs **Need objective assessment if no risk factor present (See table) V E Corr = V E x PaCO 2 /40

9








10 PANCREATITIS DAD ASPIRATION SEVERE SEPSIS CMV S. pneumoniae Normal Hypersensitivity LEGIONELLA BOOP SARS PCP MYCOPLASMA MRSA VAP TRALI DAD VARICELLA ALVEOLAR HEMORRHAGE TRAUMA CONTUSION DAD
11 Potential enrichment strategies to identify responsive subsets Direct vs Indirect Lung Injury Duration of ARDS (Early vs Late) Acute oxgenation response to PEEP Vascular Involvement Biomarkers/genetics
12 Direct vs Indirect Lung Injury: Surfactant No benefit for surfactant replacement in adults Post-hoc analysis suggested benefit in the subset with direct lung injury (pneumonia and aspiration) RCT of rsp-c Surfactant in direct lung injury failed to improve gas exchange or mortality partial inactivation of rsp-c surfactant from re-suspension process introduced with this study Pediatric RCT in direct lung injury ongoing Anzueto NEJM 1996; Spragg NEJM 2004; Taut Chest 2008; Spragg AJRCCM 2011
13 Direct vs Indirect Lung Injury: not so easy Three senior intensivists who had extensive experience with mechanical ventilation and ARDS used information from the hospital records to classify the patients as having direct or indirect ARDS 37% of cases uncertain or mixed classification Thille et al. Anesthesiology 2007

14 Biomarker for Direct (epithelial) Injury Elevated RAGE responsers to VT reduction Large observational study on RAGE in ARDS began this year Calfee, Thorax 2008; Clermont-Ferrand Clin Trial.gov
15 Potential enrichment strategies to identify responsive subsets Direct vs Indirect Lung Injury Duration of ARDS (Early vs Late) Acute oxgenation response to PEEP Vascular Involvement Biomarkers
16 Diffuse Alveolar Damage Acute exudative phase (hrs to days) intraalveolar and interstitial edema necrosis of type I alveolar lining cells hyaline membranes, hemorrhage Fibroproliferative phase (days to wks) cellular inflammation alveolar and peribronchial fibrosis vascular remodeling
17 Mortality with Steroids after 14d of ARDS Interaction p=.0170 Adjusted p=.0878 GMCSF VEGF Steroids Steinberg NEJM 2006; Thompson Crit Care 2007
18 Potential enrichment strategies to identify responsive subsets Direct vs Indirect Lung Injury Duration of ARDS (Early vs Late) Acute oxgenation response to PEEP Vascular Involvement Biomarkers
19 Fi0 2 1, PEEP 10 PaO 2 = 410 mm Hg PaO 2 = 176 mm Hg Fi0 2 1, PEEP 0 PaO 2 = 125 mm Hg

20 Disparities in: Mortality Effects of interventions Risk/Benefit ratio PaO 2 = 410 mm Hg Fi0 2 1, PEEP 10 PaO 2 = 176 mm Hg
21 Potential enrichment strategies to identify responsive subsets Direct vs Indirect Lung Injury Duration of ARDS (Early vs Late) Acute oxgenation response to PEEP Vascular Involvement Biomarkers


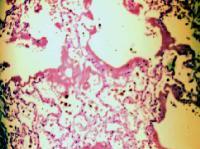
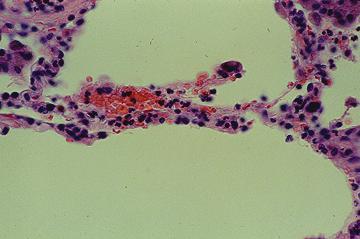
22 Microvascular Obstruction and Remodeling in ARDS Normal human lung capillaries Lung capillaries p 14 d ARDS Morphometric analysis -> Thrombosis, medial thickening, decreased vascular density of pre- and intra-acinar vessels Zapol Chest, 1977; Snow ARRD 1982
 BOPA + in 19 of 40")
 presence of DIC 3) PA HTN 4) fatal outcome Green et")
23 Macrovascular Obstruction in ARDS: Detection with Balloon Occlusion Pulmonary Angiography (BOPA) BOPA + in 19 of 40 between 1-17 days after ARDS onset Filling defects a/w 1) ARDS severity 2) presence of DIC 3) PA HTN 4) fatal outcome Green et al ARRD 1982
24 Pulmonary Dead-Space Fraction and Risk of Death in ARDS Nuckton et al. NEJM 2002
25 Hospital mortality (%) Hospital mortality (%) Vd/Vt and Prognosis in ARDS Mayo Clinic n=118 ARDSnet n=1,616 Vd/Vt = 1- [(0.86 x VCO2) / (VE x PaCO2) <= >=0.8 0 < > 0.8 Estimated death-space fraction on day 1 Estimated death-space fraction on day 1 Gajic, Critical Care 2011

26 Biomarkers of a procoagulant ARDS phenotype Ware et al, Crit Care Med, 2007
27 Summary: Opportunities for enrichment? Surfactant for direct lung injury with RAGE HFO/RMs/Prone for the new severe ARDS Vascular targeted therapies for patients with elevated dead space, RV dilation, elevated BNP/troponin (vascular phenotype) Anticoagulants (aerosol heparin, rhapc) for patients with hyper-coagulable phenotype Frank and Thompson, Curr Opinion in Crit Care 2010
28
29 One last comment Do we really know that the drugs tested for ARDS are ineffective? Are we measuring the right outcomes? Let s examine the results of a hypothetical trial and see if it changes your practice?
30 Post-traumatic Stress Disorder (PTSD) and corticosteroids? Less PTSD and improved emotional well-being in sepsis survivors treated with corticosteroids in the ICU Lower cortisol levels during ARDS a/w higher PTSD rates in long term survivors Haller CCM 1999; Hauer Brain Research 2009
31 Hypothetical Trial (n=6,000) Hydrocortisone is inexpensive, easy to administer, extensive clinical experience RCT of Hydrocortisone vs Placebo: Mortality primary No change in mortality with small CIs No change in VFDs or ICU LOS No side effects, including no secondary infections or muscle weakness. Mild hyperglycemia. Marked improvement in 6 and 12 months in rates of PTSD (40% -> 10%)? 75% back to work vs 40% in placebo Positive or Negative? Would you use hydrocortisone?
32 Summary 1. New and old definitions identify a heterogeneous group of pts Need enrichment strategies to identify subsets most likely to benefit Potential for hysiologic, proteomic, and?genomic stratification 2. We do not know if these drugs truly failed Need to take a more complete measure of the effect of an intervention, including long term functional outcomes
33 Thank you
34 Beta Adrenergic receptor (ADBR2) polymorphism and outcome AA genotype of the ADBR2 rs is associated with reduced beta receptor translation and function Single center (n=589) and multicenter (VASST, n=616) AA genotype a/w: Higher resting heart rate, higher norepinephrine dose Higher mortality (HR 2.23, ) replicated in VASST (HR 2.82) Less inhibition of IL-6 in vitro with norepinphrine Genotypic effect eliminated with steroids Nakada et al AJRCCM 2010
35 Corticosteroids may improve outcomes in the subset with AA ADRB2 genotype Nakada et al AJRCCM 2010
36 60d Mortality (95%CI) P 28.6% ( ) MP 29.2% ( )
37 It is now clear that survivors of critical illness and ALI experience a substantial and prolonged negative impact across many domains of their subsequent quality of life. Study of the impact of interventions on long-term quality of life and other functional outcomes after hospital discharge is of high value and should be a fundamental part of Phase III trials
38 ARDS Study Endpoints Mortality remains the most important endpoint No proven surrogate marker for mortality Mortality preferred over survival analysis (time to death) Ventilator free days to day 28 Not patient centered, may not change when mortality does. No longer recommended as the sole primary endpoint. No consensus on composite endpoints
39 The reporting and interpretation of results of ALI clinical studies could be improved by use of a standardized description of methods, endpoints, and results. A standardized format in ALI trials for collecting data, including long-term quality-of-life and functional status outcomes, would facilitate patient-level metaanalyses from multiple trials and enhance collaborative efforts
40 Biological Markers with Diagnostic or Prognostic Potential in ARDS Inflammation - IL-6, IL-8, stnfri, CRP Disordered Coagulation - Protein C, PAI-1 Endothelial injury - Von Willebrand factor antigen Myocardial Injury Troponin, BNP Alveolar epithelium - SP-D, stnfri, & RAGE Adhesion molecule - sicam-1 Fibroblast proliferation - PCPIII Elastin breakdown product - Desmosine (urine) Nitric Oxide Levels exhaled NO Ware et al. Chest 2010; Matthay et al. AJRCCM 2010
41 William Osler "... uncontrolled septicemia leads to frothy pulmonary edema that resembles serum, not the sanguineous transudative fluid seen in dropsy or congestive heart failure." Osler W. McCrae T. The principles and practice of medicine, designed for the use of practioners and students of medicine. 10th ed., 1233 pp. New York, Appleton; 1925
42 ARDS is a syndrome, not a diagnosis Steroid responsive conditions may present as ARDS Cryptogenic Organizing Pneumonia (COP) 1 Acute Eosinophilic Pneumonia 2 PCP complicating AIDS 3 Open Lung Biopsy for unresolving ARDS often changes therapy 4 1 Epler NEJM 85 2 Allen NEJM 89, Buchheit ARRD 92 3 Gagnon NEJM 90, Montaner, Ann Int Med 90 4 Patel Chest 2004, others
43 Conservative 25.5% Liberal 28.4% p=0.3 Probab 2.5 more VFDs (p<0.002) 3.2 less days on vent in survivors (p<0.001)
44 No Difference at One Year
45 Low Quality of Life with Con or Lib Fluid Rx Health Utilities Index Mark 2 by Fluid Rx p=0.004 for trend
46 Vent Free Days (± SD) Placebo 6.8 ± 8.5 Steroid 11.2 ± 9.4

47 Mortality with Steroids after 14d of ARDS Interaction p=.0170 Adjusted p=.0878 Exudative Proliferative Fibrosis/Repair Steinberg NEJM 2006; Thompson Crit Care 2007
48 Conservative 25.5% Liberal 28.4% p=0.3 Probab 2.5 more VFDs (p<0.002) 3.2 less days on vent in survivors (p<0.001)
49 No Difference at One Year


50 AJRCCM 2007 RMs, PEEP HFO High Risk Rx
51 ALI and ARDS: AECC Definition, 1994 Acute onset (7 days) P a 0 2 /F I 0 2 < 200 = ARDS < 300 for Acute lung Injury or ALI Bilateral infiltrates c/w pulmonary edema No evidence of LA Hypertension
52 Low Quality of Life with Con or Lib Fluid Rx Health Utilities Index Mark 2 by Fluid Rx p=0.004 for trend
53 AECC Definition: Strengths and Limitations Good Predictive Validity for mortality Luhr et al ALI (not ARDS) ARDS Rubenfeld et al ALI 42% mortality 41% mortality 38% mortality Identifies responders to low tidal volume Limited Specificity for DAD Autopsy series show no evidence of DAD in 33% majority without DAD had pneumonia, hemorrhage, pulmonary edema Luhr AJRCCM 1999; Rubenfeld NEJM 2005; Esteban Ann Int Med 2004; Gattinoni JAMA 2008
54 Tidal Volume Reduction Beneficial In All Subsets Mortality (%) ml/kg 6 ml/kg Sepsis Pneumonia Overall (N=236) (N=330) (N=902) Eisner et al. AJRCCM 2001
55 AECC Definition: Strengths and Limitations Good Predictive Validity for mortality Luhr et al ALI (not ARDS) ARDS Rubenfeld et al ALI 42% mortality 41% mortality 38% mortality Identifies responders to low tidal volume Limited Specificity for DAD Autopsy series show no evidence of DAD in 33% majority without DAD had pneumonia, hemorrhage, pulmonary edema Luhr AJRCCM 1999; Rubenfeld NEJM 2005; Esteban Ann Int Med 2004; Gattinoni JAMA 2008
 58.5% (24 patients) had P/F > 200 at 30 minutes (mean 310 +/- 74) ICU mortality 12.")
56 41 patients with ARDS by AECC criteria Placed on standardized ventilator settings (Vt 7-8, PEEP 10, FiO 2 1.0) 58.5% (24 patients) had P/F > 200 at 30 minutes (mean 310 +/- 74) ICU mortality 12.5% vs 53% (persistent ARDS)
57 THE CONCEPTUAL MODEL OF ARDS 3. Physiological derangements include increased pulmonary right-to-left venous admixture, increased physiological dead-space, decreased respiratory system compliance. 4. morphological hallmarks are lung edema, inflammation, hyaline membrane, and alveolar hemorrhage (i.e., diffuse alveolar damage) Ranieri ESICM and CCCF, Proposed Berlin Definition of ARDS
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Is ARDS Important to Recognize?
 Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Oregon Health and Science University Portland, Oregon USA
 Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
1/26/16. Prone Position How does asynchrony impact LPV and how should it be managed? Is there a role for NIV and HFNC in ARDS?
 What is ARDS?: how our understanding changed over time What are the risk factors and major etiologies? How does MV exacerbate or attenuate lung injury? Ventilator managment of ARDS Rich Kallet MS RRT FAARC
What is ARDS?: how our understanding changed over time What are the risk factors and major etiologies? How does MV exacerbate or attenuate lung injury? Ventilator managment of ARDS Rich Kallet MS RRT FAARC
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
PETAL Network. Challenges and Opportunities. Critical Care Canada Forum Toronto. November 1, 2016
 PETAL Network Challenges and Opportunities Critical Care Canada Forum Toronto November 1, 2016 Roy Brower, MD Johns Hopkins University Chair, PETAL Network Steering Committee PETAL Network History Objectives,
PETAL Network Challenges and Opportunities Critical Care Canada Forum Toronto November 1, 2016 Roy Brower, MD Johns Hopkins University Chair, PETAL Network Steering Committee PETAL Network History Objectives,
PETAL Network. Critical Care Canada Forum Toronto. October 27, 2015
 PETAL Network Critical Care Canada Forum Toronto October 27, 2015 Roy Brower, MD Johns Hopkins University School of Medicine Chair, PETAL Network Steering Committee Disclosures None PETAL Network History
PETAL Network Critical Care Canada Forum Toronto October 27, 2015 Roy Brower, MD Johns Hopkins University School of Medicine Chair, PETAL Network Steering Committee Disclosures None PETAL Network History
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Replacement of air with fluid, inflammatory. cells or cellular debris. Parenchymal, Interstitial (Restrictive) and Vascular Diseases.
 and Vascular Diseases.") Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Parenchymal, Interstitial (Restrictive) and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Replacement of air with fluid, inflammatory cells Pulmonary Edema Pneumonia Hemorrhage Diffuse alveolar
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Imaging Cancer Treatment Complications in the Chest
 Imaging Cancer Treatment Complications in the Chest Michelle S. Ginsberg, MD Objectives Imaging Cancer Treatment Complications in the Chest To understand the mechanisms of action of different classes of
Imaging Cancer Treatment Complications in the Chest Michelle S. Ginsberg, MD Objectives Imaging Cancer Treatment Complications in the Chest To understand the mechanisms of action of different classes of
Phenotyping of ARDS and non ARDS Patients
 Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
The ARDS is characterized by increased permeability. Incidence of ARDS in an Adult Population of Northeast Ohio*
 Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care
 28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Oxygen:..Nothing is without poison.. the poison is in the dose..
 Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Interdepartmental Division of Critical Care Medicine Mount Sinai Hospital/University Health Network University of Toronto Toronto, Canada Oxygen:..Nothing is without poison.. the poison is in the dose..
Adjunct Approaches to the Care of the PARDS Patient. Doug Willson, MD Children s Hospital of Richmond April 21, 2015
 Adjunct Approaches to the Care of the PARDS Patient Doug Willson, MD Children s Hospital of Richmond April 21, 2015 Disclosures! I am a consultant for Discovery Laboratories! No other conflicts to disclose
Adjunct Approaches to the Care of the PARDS Patient Doug Willson, MD Children s Hospital of Richmond April 21, 2015 Disclosures! I am a consultant for Discovery Laboratories! No other conflicts to disclose
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Effect of ARDS Severity and Etiology on Short-Term Outcomes
 Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES
 DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
DISEASES OF THE RESPIRATORY SYSTEM 2017 DR HEYAM AWAD LECTURE 1: RESPIRATORY DISTRESS SYNDROMES This lecture covers two topics: neonatal respiratory distress syndrome (neonatal RDS) and adult respiratory
clinical investigations in critical care The Role of Open-Lung Biopsy in ARDS*
 clinical investigations in critical care The Role of Open-Lung Biopsy in ARDS* Sanjay R. Patel, MD; Dimitri Karmpaliotis, MD; Najib T. Ayas, MD; Eugene J. Mark, MD; John Wain, MD, FCCP; B. Taylor Thompson,
clinical investigations in critical care The Role of Open-Lung Biopsy in ARDS* Sanjay R. Patel, MD; Dimitri Karmpaliotis, MD; Najib T. Ayas, MD; Eugene J. Mark, MD; John Wain, MD, FCCP; B. Taylor Thompson,
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
ARDS Endotypes and Phenotypes
 ARDS Endotypes and Phenotypes Jason D. Christie, MD, MS Associate Professor of Medicine Associate Professor of Epidemiology University of Pennsylvania School of Medicine Disclosures No relevant commercial
ARDS Endotypes and Phenotypes Jason D. Christie, MD, MS Associate Professor of Medicine Associate Professor of Epidemiology University of Pennsylvania School of Medicine Disclosures No relevant commercial
Endothelial Biomarkers in Human Sepsis Pathogenesis and Prognosis for ARDS
 Endothelial Biomarkers in Human Sepsis Pathogenesis and Prognosis for ARDS Carolyn M. Hendrickson, MD, MPH 1 2, 3, 4 and Michael A. Matthay, MD 1. Department of Medicine, Division of Pulmonary and Critical
Endothelial Biomarkers in Human Sepsis Pathogenesis and Prognosis for ARDS Carolyn M. Hendrickson, MD, MPH 1 2, 3, 4 and Michael A. Matthay, MD 1. Department of Medicine, Division of Pulmonary and Critical
Reporting Heterogeneity of Treatment Effect in Critical Care Trials
 Reporting Heterogeneity of Treatment Effect in Critical Care Trials CCCF, Toronto November 1, 2016 B. Taylor Thompson MD Professor of Medicine Massachusetts General Hospital Harvard Medical School Boston,
Reporting Heterogeneity of Treatment Effect in Critical Care Trials CCCF, Toronto November 1, 2016 B. Taylor Thompson MD Professor of Medicine Massachusetts General Hospital Harvard Medical School Boston,
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA?
 WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
WHAT S NEW-ISH IN ARDS MANAGEMENT AFTER TRAUMA? Bryce Robinson MD, MS, FACS, FCCM Associate Professor of Surgery Associate Medical Director, Critical Care Harborview Medical Center Department of Surgery
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Intravenous Vitamin C. Severe Sepsis Acute Lung Injury
 Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases
 i and Vascular Diseases") Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Pulmonary Diseases: Structure-Function Correlation II Parenchymal, Interstitial i (Restrictive) i and Vascular Diseases Alain C. Borczuk, M.D. Dept of Pathology Pulmonary Diseases: Structure-Function Correlation
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Introduction Definition Etiology Epidemiology Lung injury prediction score. Pathophysiology Diagnosis Clinical presentation Management Conclusion
 Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Disclosures. Learning Objectives. Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach 3/10/2017
 Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Critical Care Medicine Update for Non-Intensivists 2015
 27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The