Presented by : Shashwat Mishra
|
|
|
- Opal Gibbs
- 5 years ago
- Views:
Transcription
1 Presented by : Shashwat Mishra
2 Named after Hans Chiari ( ). Professor of Pathology in Prague, Czechoslovakia, Paper entitled Concerning alterations in the cerebellum resulting from cerebral hydrocephalus Published in Deutsche Medizinische Wochenscriff in 1891 Autopsy series, 40 cases Described cerebellar anomalies in congenital hydrocephalus
3 Initially described three malformations 5 years later he revised the second and added a fourth Arnold described a single case with Chiari II features The chiari II malformation also known as Arnold-Chiari malformation.
4 Series of hindbrain anomalies No anatomical or embryological correlation between them Four types
5 Type Chiari I Chiari II Chiari III Chiari IV Definition Caudal descent of cerebellar tonsils > 5mm below foramen magnum Hydrocephalus uncommon Caudal herniation of cerebellar vermis, brainstem and fourth ventricle Almost all have hydrocephalus and myelomeningocele Chiari II and posterior fossa contents herniating into occipital/ high cervical encephalocele Cerebellar aplasia or hypoplasia with aplasia of tentorium cerebelli
6 Traditionally defined as > 5mm tonsillar descent below the foramen magnum. Tonsils ascend with age Abnormal for age > 6mm in first decade > 5 mm in second and third decade > 4 mm in fourth through eighth decade > 3 mm in ninth decade.
7 more important than absolute tonsillar descent may be Peg like shape of tonsils Attenuation of posterior fossa cisternal spaces Suggestive clinical picture Primarily chiari I is manifestation of underdevelopment and malformation of occipital cranium Cerebellar ectopia due to reduced posterior fossa volume and crowding of contents
8 Other manifestations of hypodeveloped post fossa Increased slope of the tentorium Reduced height of the supraocciput Reduced length of the clivus Retroflexion of odontoid process
9 Acquired tonsillar ectopia Due to reduced volume of cranial cavity (Rickets, Craniosynostosis, Pagets disease) Due to increase in volume of intracranial contents (acute hydrocephalus, tumour, cerebral edema )
10 Chiari I malformation
11 Skull Shortened supraocciput Shortened clivus Larger than normal foramen magnum Empty sella Clival concavity, platybasia, basilar impression
12 Spine Klippel-flail deformity and atlanto axial assimilation Retroflexed odontoid process Thickened ligamentum flavum Scoliosis Meninges Elevated slope of tentorium cerebelli Thickened arachnoid at foramen magnum level Dural thickening/ at the level of arch of atlas
13 Spinal cord 50 to 75 % have cavitation within the cord (syrinx) Lower cervical and thoracic cord mostly involved. Segment of cord caudal to 4 th ventricle may be spared from cavitation. Brain usually normal except for tonsillar abnormality Hydrocephalus described in 3 to 10 %.
14
15 Pain is the most common complaint Occipital and cervical region pain aggravated by Valsalva, cough-laugh headaches Signs and symptoms related to brainstem / cranial nerve and cerebellar compromise Ataxia, downbeating nystagmus, incordination, dizziness Dyspahgia, dysarthria,hiccoughs, glossal atrophy Impaired gag, facial numbness Extreme cases cerebellar fits
16 Signs and symptoms related to syrinx Dissociative sensory loss, upper limb weakness and thinning, lower limb spasticity. Neuropathic pain in the extremities. Neuropathic joints in upper extremities. Uncommonly, JPS loss leading to sensory ataxia. Presentation usually in the 2 nd and 3 rd decades with a female preponderance
17 Gardner s hydrodynamic theory Blocked fourth ventricular outlet Pulsatile CSF pressure transmitted to central canal through obex Water hammer William s craniospinal dissociation theory Valve like obstruction to free flow of CSF between cranial and spinal subarachnoid space at FM Equalisation of CSF pressure between cranial and spinal compartments hindered CSF sucked into the syrinx.
18 Oldfield s theory Systolic downward motion of the tonsils creates a piston effect on the cervical spinal cord Interstitial fluid driven into the central canal distending it. No theory however, successfully explains all observations
19
20 asymptomatic chiari I Exclude hydrocephalus, ventral compression, cervical instability syrinx No syrinx Chiari decompression >7mm caudal descent <7mm caudal descent Exercise clinical judgement Observation
21 Symptomatic chiari I Exclude hydrocephalus, ventral compression, cervical instability syrinx No syrinx Chiari decompression >7mm caudal descent 3-7mm <3mm caudal descent Exercise clinical judgement Observation with frequent evaluation
22 Aim of the surgical procedure Establishment of normal CSF outflow from the ventricles Increasing posterior fossa volume
23 Surgical options Suboccipital bone removal Dural opening with or without closure Arachnoid opening and hitching Tonsillar reduction and opening of fourth ventricular outlet Fourth ventricular shunting
24 Suboccipital bone removal + C1 laminectomy 3 X 3 cm suboccipital craniectomy Dura left intact Dura inelastic hence, decompression inadequate Larger craniectomies with dural opening result in cerebellar ptosis. Dural opening with or without closure Options Only superficial layer divided Durotomy with intact arachnoid Augmentation duraplasty Williams procedure dural edges sutured to the muscle At craniocervical juction, division of thick dural band
25 Opening the arachnoid Required when significant tonsillar descent with syringomyelia Arachnoid bands divided Arachnoid pegged to the dural edges Augmentation duraplasty
26 Tonsil reduction Subpial coagulation Subpial resection when tonsils gliotic Fourth ventricular shunting When tonsils encased in dense arachnoid scar Shunt tubing inserted under USG guidance into the fourth ventricle and communicated to cervical subarachnoid space Obex plugging redundant
27 Complications Aseptic meningitis (most common) Wound dehiscence, pseudomeningocele CSF leak
28 Defining features Caudal descent of vermis, fourth ventricle and brainstem Almost always associated with hydrocephalus and associated anomalies Seen in almost all patients with myelomeningocele 0.02% of all births with female preponderance
29 Chiari s theory Hydrocephalus leading to secondary chiari % may not have hydrocephalus Associated anomalies not explained Chairi II features precede hydrocephalus Small post fossa, low lying tentorium, upward cerebellar herniation not explained
30 Cleland s theory Primary dysgenesis of the hindbrain Fails to explain supratentorial anomalies Induced small posterior fossa Due to CSF leaking out from the open spinal cord defect Fails to explain associated anomalies
31 Penfield s traction theory Traction by tethering of cord at the site of myelomeningocele pulls the post fossa contents Traction effect however dissipated four spinal levels rostral Fails to explain associated cranial deformities
32 Unified theory of Mclone and Knepper Currently most accepted Both the open neural tube defect and incomplete occlusion of central canal responsible Temporary occlusion of the neural tube (day23-32) mandatory for upstream ventricular distension Post fossa not fully developed due to inadequate ventricular distension Rapid growth of hindbrain later leads to herniation


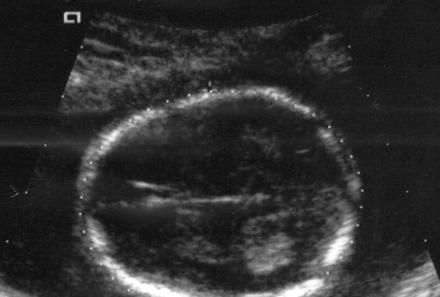
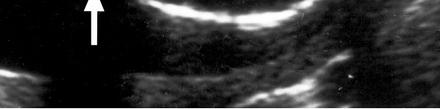
33 skull Luckenschadel/ craniolacunia Frontal bone scalloping lemon sign Scalloping of petrous bone and jugular tubercles Concavity of the clivus Low inion,small post fossa Enlarged foramen magnum Clival concavity Basilar invagination and atlas assimilation


34 Frontal bone scalloping - Lemon sign Normal fetus


35 Scalloped petrous bones in chiari II Normal skull in 50 yr old man
36 Spine Cervical spinal canal enlarged. Scalloping of the odontoid process Incomplete posterior arch of C1 Klippel-Feil deformity
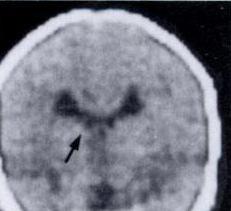
37 Ventricle and cistern Hydrocephalus seen in 90%. Fourth ventricular outlet obstruction responsible Aqueductal stenosis uncommonly responsible for hydrocephalus Medial pointing of the inferior margins of floor of lateral ventricles colpocephaly Fourth ventricle typically small, flat and elongated Lateral recesses not well defined

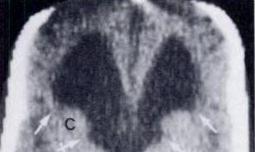
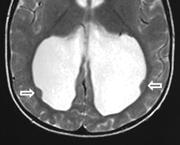


38 colpocephaly Pointed frontal horns Slit like fourth ventricle


39 bat wing appearance


40 Meninges Tentorium cerebelli usually widened heart shaped Low lying,hypoplastic Falx cerebri fenestrated/hypoplastic Low lying tent Normal hiatus Hiatus in chiari II

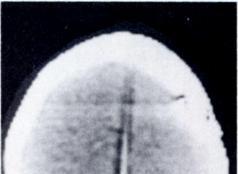


41 CECT head showing interruptions in falx blush suggestive of falx fenestrations
42 Spinal cord Myelomeningocele always associated with Chiari II Syringomyelia in 20-95% Shortened cervical cord Telencephalon Complete partial agenesis of corpus callosum/septum pellucidum Polygyria chinese lettering - interdigitation of occipital /parietal lobes
43 Gray matter heterotopia Agenesis of olfactory tract/bulb/cingulate gyrus

44 Diencephalon Enlarged massa intermedia


45 Mesencephalon Tectal beaking due to fusion of the colliculi Midbrain typically elongated Cranial nerve nuclei may be malformed Aqueduct may be stenotic, stretched,posteriorly kinked or forked
46 Metencephalon Cerebellum grossly smaller and may tower above tentorium Cerebellum may be displaced laterally spreading around the brainstem banana sign Lateral cerebellar edges may touch brainstem and basilar artery cerebellar inversion Pons elongated and flattened


47 Banana sign Normal fetus
48 Cerebellar inversion Chinese lettering


49 Myelencephalon Medullary kinking, elongation and flattening Pyramidal decussation more cephalad than normal
50 Most common is with open neural tube defects Symptomatic chiari II is the most common cause of death in children <2 yrs of age with MMC. Symptomatic patients can be classified according to age at presentation Whatever be the age of child, hydrocephalus/ shunt malfunction should be excluded
51 Age at presentation less than 2yrs Most frequent symptoms related to brain stem and cranial nerve dysfunction Symptomatic chiari is a neurosurgical emergency in this group. Most commonly inspiratory stridor and PEAC (prolonged expiratory apnea and cyanosis) PEAC = apneic spell+opthistonic posturing and cyanosis Laryngoscopy may reveal impaired vocal cord abduction Downbeat nystagmus, fixed retrocollis
52 Other signs and symptoms Impairment of gag Dysphagia, chronic aspiration, nasal regurgitation Quadriparesis, nystagmus, developmental delay Weak cry.
53 Presentation in older age group Less serious and rarely an emergency Hallmark is cervical myelopathy Weakness and spasticity in upper limbs suboccipital headache Ataxia Hand weakness, atrophy Syringomyelia and associated symptoms Opthalmic problems common in adults
54
55 asymptomatic chiari II Exclude hydrocephalus/verify shunt function and cervical stability syrinx No syrinx Verify shunt function observation Small syrinx Large syrinx observation Consider cervical laminectomy and syringo pleural shunt
56 symptomatic chiari II Exclude hydrocephalus/verify shunt function and cervical stability Large syrinx No syrinx/small to moderate syrinx Chiari decompresion plus syringopleural shunt Cervical laminectomy with limited posterior fossa decompression
57 Surgical technique basically similar to that in chiari-i Cervical laminectomy should expose the inferior margin of the herniated cerebellum Limited suboccipital craniectomy Constricting dural bands divided Key objective finding the outlet of fourth ventricle Choroid plexus may serve as a guide
58 Obstructive vermian tissue may be divided /perforated to encourage CSF flow out of the ventricles. Medullary kink not to be confused with vermis. Arachnoid clipped to dura with augmentation duraplasty Complications of this procedure similar to that for Chiari I.
59 Chiari III Very rare Occipital or cervical encephalocele along with chiari II anomalies Chiari IV No hindbrain herniation Cerebellar hypoplasia or aplasia
60 Chiari zero CSF equilibrium changes at cranio-cervical junction No hindbrain herniation Syringohydromyelia Post fossa decompression leads to dramatic improvement Other causes of syrinx must be excluded.
61
Chiari Malformations. Google. Objectives Seventh Annual NKY TBI Conference 3/22/13. Kerry R. Crone, M.D.
 Chiari Malformations Kerry R. Crone, M.D. Professor of Neurosurgery and Pediatrics University of Cincinnati College of Medicine University of Cincinnati Medical Center Cincinnati Children s Hospital Medical
Chiari Malformations Kerry R. Crone, M.D. Professor of Neurosurgery and Pediatrics University of Cincinnati College of Medicine University of Cincinnati Medical Center Cincinnati Children s Hospital Medical
CNS Embryology 5th Menstrual Week (Dorsal View)
") Imaging of the Fetal Brain; Normal & Abnormal Alfred Abuhamad, M.D. Eastern Virginia Medical School CNS Embryology 5th Menstrual Week (Dorsal View) Day 20 from fertilization Neural plate formed in ectoderm
Imaging of the Fetal Brain; Normal & Abnormal Alfred Abuhamad, M.D. Eastern Virginia Medical School CNS Embryology 5th Menstrual Week (Dorsal View) Day 20 from fertilization Neural plate formed in ectoderm
Brain Imaging. Bearbeitet von Klaus Sartor, Stefan Hähnel, Bodo Kress
 Brain Imaging Bearbeitet von Klaus Sartor, Stefan Hähnel, Bodo Kress 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 143961 1 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige
Brain Imaging Bearbeitet von Klaus Sartor, Stefan Hähnel, Bodo Kress 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 143961 1 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige
Abstract !"# $% &%'(% )* ( % +$$ '% % % Presentation Notes
* ( % +$$ '% % % Presentation Notes") Presenter Name: John Oro, MD Topic: Chiari & Syringomyelia 101 A Brief Look at Neuroanatomy The brain is enclosed and protected by a rounded skull made of rigid bone. The bottom of the skull contains multiple
Presenter Name: John Oro, MD Topic: Chiari & Syringomyelia 101 A Brief Look at Neuroanatomy The brain is enclosed and protected by a rounded skull made of rigid bone. The bottom of the skull contains multiple
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Djamila Kafoufi Al Galaa Military Hospital Cairo
 Djamila Kafoufi Al Galaa Military Hospital Cairo Herniation cerebellar tonsils below the foramen magnum, Hans Chiari 4 types Chiari I less than 5mm,HDC rare,syringomyelia often present. Chiari II,protrusion
Djamila Kafoufi Al Galaa Military Hospital Cairo Herniation cerebellar tonsils below the foramen magnum, Hans Chiari 4 types Chiari I less than 5mm,HDC rare,syringomyelia often present. Chiari II,protrusion
Neuroanatomy. Assistant Professor of Anatomy Faculty of Medicine The University of Jordan Dr Maha ELBeltagy
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Development of the Central Nervous System Development of the nervous system Development
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Development of the Central Nervous System Development of the nervous system Development
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
A STUDY OF POSTERIOR FOSSA MALFORMATIONS: MR IMAGING Ravi Ningappa 1, Vaishali D. M 2, Vijayaraghavachari T. V 3, Manjappa B. H 4
 A STUDY OF POSTERIOR FOSSA MALFORMATIONS: MR IMAGING Ravi Ningappa 1, Vaishali D. M 2, Vijayaraghavachari T. V 3, Manjappa B. H 4 HOW TO CITE THIS ARTICLE: Ravi Ningappa, Vaishali D. M, Vijayaraghavachari
A STUDY OF POSTERIOR FOSSA MALFORMATIONS: MR IMAGING Ravi Ningappa 1, Vaishali D. M 2, Vijayaraghavachari T. V 3, Manjappa B. H 4 HOW TO CITE THIS ARTICLE: Ravi Ningappa, Vaishali D. M, Vijayaraghavachari
Moderators: Dr Manmohan Singh Dr Pankaj Singh Presentor : Dr Kanwaljeet Garg
 Moderators: Dr Manmohan Singh Dr Pankaj Singh Presentor : Dr Kanwaljeet Garg History! Hans Chiari (1851 1916) was born in Vienna, Austria! He was Professor of pathology at Prague, Czechoslovakia! His initial
Moderators: Dr Manmohan Singh Dr Pankaj Singh Presentor : Dr Kanwaljeet Garg History! Hans Chiari (1851 1916) was born in Vienna, Austria! He was Professor of pathology at Prague, Czechoslovakia! His initial
intracranial anomalies
 Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Chapter 5: Fetal Central Nervous System 84 intracranial anomalies Hydrocephaly Dilatation of ventricular system secondary to an increase in the amount of CSF. Effects of hydrocephalus include flattening
Chapter 5: Fetal Central Nervous System 71
 71 Chapter 5 Fetal Central Nervous System Embryology NEURULATION begins with the formation of the neural plate, the neural folds and their ultimate fusion and closure as the NEURAL TUBE. NEURAL PLATE -
71 Chapter 5 Fetal Central Nervous System Embryology NEURULATION begins with the formation of the neural plate, the neural folds and their ultimate fusion and closure as the NEURAL TUBE. NEURAL PLATE -
Slide 1. Slide 2. Slide 3. Tomography vs Topography. Computed Tomography (CT): A simplified Topographical review of the Brain. Learning Objective
: A simplified Topographical review of the Brain. Learning Objective") Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Chiari bridges review Chiari Treatments & Potential Pitfalls
 Chiari bridges review Chiari Treatments & Potential Pitfalls Once diagnosed, you will usually be referred to a specialist (not a Chiari Specialist, but an everyday, run-of-the-mill neurologist or neurosurgeon).
Chiari bridges review Chiari Treatments & Potential Pitfalls Once diagnosed, you will usually be referred to a specialist (not a Chiari Specialist, but an everyday, run-of-the-mill neurologist or neurosurgeon).
Multimodal Evaluation Of Cerebrospinal Fluid (csf ) Dynamics Following Extradural Decompression For Chiari I Malformation
 Dynamics Following Extradural Decompression For Chiari I Malformation") Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Multimodal Evaluation Of Cerebrospinal Fluid (csf ) Dynamics
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2015 Multimodal Evaluation Of Cerebrospinal Fluid (csf ) Dynamics
Idiopathic cervical syringomyelia can be associated. Pediatric Chiari malformation Type 0: a 12-year institutional experience.
 J Neurosurg J Neurosurg Pediatrics Pediatrics 8:000 000, 8:1 5, 2011 Pediatric Chiari malformation Type 0: a 12-year institutional experience Clinical article Joshua J. Chern, M.D., Ph.D., Amber J. Gordon,
J Neurosurg J Neurosurg Pediatrics Pediatrics 8:000 000, 8:1 5, 2011 Pediatric Chiari malformation Type 0: a 12-year institutional experience Clinical article Joshua J. Chern, M.D., Ph.D., Amber J. Gordon,
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
Introduction to Neurosurgical Subspecialties: Pediatric Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Pediatric Neurosurgery Pediatric neurosurgeons
Ventricles, CSF & Meninges. Steven McLoon Department of Neuroscience University of Minnesota
 Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Complex Hydrocephalus
 2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
2012 Hydrocephalus Association Conference Washington, DC - June 27-July1, 2012 Complex Hydrocephalus Marion L. Walker, MD Professor of Neurosurgery & Pediatrics Primary Children s Medical Center University
DEVELOPMENT OF BRAIN
 Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2
 Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2 Abstract Cranio-cervical junction abnormalities are a rare combination of congenital or acquired
Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2 Abstract Cranio-cervical junction abnormalities are a rare combination of congenital or acquired
Chapter 3. Structure and Function of the Nervous System. Copyright (c) Allyn and Bacon 2004
 Allyn and Bacon 2004") Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Arnold Chiari Malformation - A hospital based autopsy study
 Rapotra Megha et al / International Journal of Biomedical Research 2017; 8(05): 250-254. 250 International Journal of Biomedical Research ISSN: 0976-9633 (Online); 2455-0566 (Print) Journal DOI: https://dx.doi.org/10.7439/ijbr
Rapotra Megha et al / International Journal of Biomedical Research 2017; 8(05): 250-254. 250 International Journal of Biomedical Research ISSN: 0976-9633 (Online); 2455-0566 (Print) Journal DOI: https://dx.doi.org/10.7439/ijbr
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Department of Cognitive Science UCSD
 Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
HEAD/NECK VESSELS. Objectives
 Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
Objectives Arterial Supply to Head and Neck Arteries to Head Surrounding Brain Common carotid arteries Arteries to Head Surrounding Brain External carotid arteries Arteries to Head Surrounding Brain External
CASE OF THE WEEK PROFESSOR YASSER METWALLY
 CLINICAL PICTURE CLINICAL PICTURE A 13 years old male patient presented clinically with atrophy of the small muscles of the hands, bulbar cranial nerve manifestations and cerebellar manifestations. Physical
CLINICAL PICTURE CLINICAL PICTURE A 13 years old male patient presented clinically with atrophy of the small muscles of the hands, bulbar cranial nerve manifestations and cerebellar manifestations. Physical
M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels
 M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels Anatomical Directions Terms like dorsal, ventral, and posterior provide a means of locating structures
M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels Anatomical Directions Terms like dorsal, ventral, and posterior provide a means of locating structures
Pathological reaction to disease
 Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Role of MRI in Selection of Patients for Surgery and Assessing the Post Operative Outcome in Chiari 1 Malformation
 DOI: 10.7860/IJARS/2017/13599:2222 Radiology Section Original Article Role of MRI in Selection of Patients for Surgery and Assessing the Post Operative Outcome in Chiari 1 Malformation Rajesh Kumar V,
DOI: 10.7860/IJARS/2017/13599:2222 Radiology Section Original Article Role of MRI in Selection of Patients for Surgery and Assessing the Post Operative Outcome in Chiari 1 Malformation Rajesh Kumar V,
Development of Brain Stem, Cerebellum and Cerebrum
 Development of Brain Stem, Cerebellum and Cerebrum The neural tube cranial to the 4th pair of somites develop into the brain. 3 dilatations and 2 flexures form at the cephalic end of the neural tube during
Development of Brain Stem, Cerebellum and Cerebrum The neural tube cranial to the 4th pair of somites develop into the brain. 3 dilatations and 2 flexures form at the cephalic end of the neural tube during
Chiari malformations. A fact sheet for patients and carers
 A fact sheet for patients and carers Chiari malformations This fact sheet provides information on Chiari malformations. It focuses on Chiari malformations in adults. Our fact sheets are designed as general
A fact sheet for patients and carers Chiari malformations This fact sheet provides information on Chiari malformations. It focuses on Chiari malformations in adults. Our fact sheets are designed as general
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Anatomy Lab (1) Theoretical Part. Page (2 A) Page (2B)
 Theoretical Part. Page (2 A) Page (2B)") Anatomy Lab (1) This sheet only includes the extra notes for the lab handout regarding the theoretical part, as for the practical part it includes everything the doctor mentioned. Theoretical Part Page
Anatomy Lab (1) This sheet only includes the extra notes for the lab handout regarding the theoretical part, as for the practical part it includes everything the doctor mentioned. Theoretical Part Page
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Microsurgery of Arnold-Chiari malformation in adults with and without hydromyelia
 Microsurgery of Arnold-Chiari malformation in adults with and without hydromyelia ALBERT L. RHOTON, JR., M.D. Division of Neurological Surgery, University of Florida Health Center, Gainesville, Florida
Microsurgery of Arnold-Chiari malformation in adults with and without hydromyelia ALBERT L. RHOTON, JR., M.D. Division of Neurological Surgery, University of Florida Health Center, Gainesville, Florida
Anatomy Lecture Notes Chapter 13
 I. embryonic development of the CNS A. neurulation is the formation of the CNS in the embryo invagination of dorsal ectoderm (outer layer of embryo cells) this process is induced (caused) by the notochord
I. embryonic development of the CNS A. neurulation is the formation of the CNS in the embryo invagination of dorsal ectoderm (outer layer of embryo cells) this process is induced (caused) by the notochord
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES
 ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
ACTIVITY 7: NERVOUS SYSTEM HISTOLOGY, BRAIN, CRANIAL NERVES LABORATORY OBJECTIVES: 1. Histology: Identify structures indicated on three different slides or images of nervous system tissue. These images
Chapter 14: The Brain and Cranial Nerves. Copyright 2009, John Wiley & Sons, Inc.
 Chapter 14: The Brain and Cranial Nerves Development of the Brain Three to four-week embryo: prosencephalon, mesencephalon and rhombencephalon. Five-week embryo: telencephalon (cerebrum), diencephalon
Chapter 14: The Brain and Cranial Nerves Development of the Brain Three to four-week embryo: prosencephalon, mesencephalon and rhombencephalon. Five-week embryo: telencephalon (cerebrum), diencephalon
Central Nervous System (CNS) -> brain and spinal cord. Major Divisions of the nervous system:
 -> brain and spinal cord. Major Divisions of the nervous system:") Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Cranial Cavity REFERENCES: OBJECTIVES OSTEOLOGY. Stephen A. Gudas, PT, PhD
 Stephen A. Gudas, PT, PhD Cranial Cavity REFERENCES: Moore and Agur, Essential Clinical Anatomy (ECA), 3rd ed., pp. 496 498; 500 507; 512 514 Grant s Atlas 12 th ed., Figs 7.6; 7.19 7.30. Grant s Dissector
Stephen A. Gudas, PT, PhD Cranial Cavity REFERENCES: Moore and Agur, Essential Clinical Anatomy (ECA), 3rd ed., pp. 496 498; 500 507; 512 514 Grant s Atlas 12 th ed., Figs 7.6; 7.19 7.30. Grant s Dissector
BRAIN STEM AND CEREBELLUM..
 Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Pediatric and adult Chiari malformation Type I surgical series : a review of demographics, operative treatment, and outcomes
 PEDIATRICS literature review Pediatric and adult Chiari malformation Type I surgical series 1965 2013: a review of demographics, operative treatment, and outcomes aska arnautovic, bsc, 1 bruno splavski,
PEDIATRICS literature review Pediatric and adult Chiari malformation Type I surgical series 1965 2013: a review of demographics, operative treatment, and outcomes aska arnautovic, bsc, 1 bruno splavski,
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
The MRI in Arnold-Chiari Syndrome I and Idiopathic Syringomyelia
 The MRI in Arnold-Chiari Syndrome I and Idiopathic Syringomyelia Author: Miguel B. Royo Salvador, MD, PhD Introduction Magnetic resonance imaging (MRI) is a crucial diagnostic tool for men, women, and
The MRI in Arnold-Chiari Syndrome I and Idiopathic Syringomyelia Author: Miguel B. Royo Salvador, MD, PhD Introduction Magnetic resonance imaging (MRI) is a crucial diagnostic tool for men, women, and
Preoperative evaluation and surgical management of the Arnold-Chiari II malformation
 J Neurosurg 64:363-370, 1986 Preoperative evaluation and surgical management of the Arnold-Chiari II malformation JOAN L. VENES, M.D., KEITH L. BLACK, M.D., AND JOSEPH T. LATACK, M.D. Section of Neurosurgery,
J Neurosurg 64:363-370, 1986 Preoperative evaluation and surgical management of the Arnold-Chiari II malformation JOAN L. VENES, M.D., KEITH L. BLACK, M.D., AND JOSEPH T. LATACK, M.D. Section of Neurosurgery,
Spinal Imaging. Bearbeitet von Herwig Imhof. 1. Auflage Taschenbuch. 312 S. Paperback ISBN Format (B x L): 12,5 x 19 cm
: 12,5 x 19 cm") Spinal Imaging Bearbeitet von Herwig Imhof 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 144071 6 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige Medizinische Fachgebiete
Spinal Imaging Bearbeitet von Herwig Imhof 1. Auflage 2007. Taschenbuch. 312 S. Paperback ISBN 978 3 13 144071 6 Format (B x L): 12,5 x 19 cm Weitere Fachgebiete > Medizin > Sonstige Medizinische Fachgebiete
Chiari III Joseph Junewick, MD FACR
 Chiari III Joseph Junewick, MD FACR 07/02/2010 History Newborn with suboccipital mass. Diagnosis Chiari III Additional Clinical Surgery-Skin covered suboccipital cystic mass confined by the dura. Pathology-Leptomeningeal
Chiari III Joseph Junewick, MD FACR 07/02/2010 History Newborn with suboccipital mass. Diagnosis Chiari III Additional Clinical Surgery-Skin covered suboccipital cystic mass confined by the dura. Pathology-Leptomeningeal
Fetal Medicine. Case Presentations. Dr Ermos Nicolaou Fetal Medicine Unit Chris Hani Baragwanath Hospital. October 2003
 Case Presentations Dr Ermos Nicolaou Fetal Medicine Unit Chris Hani Baragwanath Hospital October 2003 Case 1 Ms A M 22year old P0 G1 Referred from Sebokeng Hospital at 36w for polyhydramnios On Ultrasound:
Case Presentations Dr Ermos Nicolaou Fetal Medicine Unit Chris Hani Baragwanath Hospital October 2003 Case 1 Ms A M 22year old P0 G1 Referred from Sebokeng Hospital at 36w for polyhydramnios On Ultrasound:
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture. caudal = toward the spinal cord)
 Human Anatomy lecture. caudal = toward the spinal cord)") Insight: Some cranial nerve disorders Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture I. Overview (Directional terms: rostral = toward the forehead caudal = toward the spinal cord) A. 3 Major parts
Insight: Some cranial nerve disorders Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture I. Overview (Directional terms: rostral = toward the forehead caudal = toward the spinal cord) A. 3 Major parts
Introduction and Basic structural organization of the nervous system
 Introduction and Basic structural organization of the nervous system **the slides are in bold and the book is in red Done by : razan krishan & marah marahleh INTRODUCTION The nervous system, along with
Introduction and Basic structural organization of the nervous system **the slides are in bold and the book is in red Done by : razan krishan & marah marahleh INTRODUCTION The nervous system, along with
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM
 Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Pathogenesis of Chiari malformation: a morphometric study of the posterior cranial fossa
 Pathogenesis of Chiari malformation: a morphometric study of the posterior cranial fossa Misao Nishikawa, M.D., Hiroaki Sakamoto, M.D., Akira Hakuba, M.D., Naruhiko Nakanishi, M.D., and Yuichi Inoue, M.D.
Pathogenesis of Chiari malformation: a morphometric study of the posterior cranial fossa Misao Nishikawa, M.D., Hiroaki Sakamoto, M.D., Akira Hakuba, M.D., Naruhiko Nakanishi, M.D., and Yuichi Inoue, M.D.
Unit 18: Cranial Cavity and Contents
 Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Brainstem. By Dr. Bhushan R. Kavimandan
 Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Central nervous system. Obstetrics Content Outline Obstetrics - Fetal Abnormalities
 Obstetrics Content Outline Obstetrics - Fetal Abnormalities Many congenital malformations of the CNS result from incomplete closure of the neural tube Effective February 2007 10 16% the most common neural
Obstetrics Content Outline Obstetrics - Fetal Abnormalities Many congenital malformations of the CNS result from incomplete closure of the neural tube Effective February 2007 10 16% the most common neural
Nsci 2100: Human Neuroanatomy Examination 1
 Name KEY Lab Section Nsci 2100: Human Neuroanatomy Examination 1 On this page, write your name and lab section. On your scantron answer sheet, enter your name (last name, space, first name), internet ID
Name KEY Lab Section Nsci 2100: Human Neuroanatomy Examination 1 On this page, write your name and lab section. On your scantron answer sheet, enter your name (last name, space, first name), internet ID
Significance of Cerebellar Tonsillar Position on MR
 795 Significance of Cerebellar Tonsillar Position on MR A. J. Barkovich 1. 3 F. J. Wippold 2. 3 J. L. Sherman 3. 4 C. M. Citrin 4. 5 It has been noted that a low degree of ectopia of the cerebellar tonsils
795 Significance of Cerebellar Tonsillar Position on MR A. J. Barkovich 1. 3 F. J. Wippold 2. 3 J. L. Sherman 3. 4 C. M. Citrin 4. 5 It has been noted that a low degree of ectopia of the cerebellar tonsils
Introduction to the Central Nervous System: Internal Structure
 Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
Introduction to the Central Nervous System: Internal Structure Objective To understand, in general terms, the internal organization of the brain and spinal cord. To understand the 3-dimensional organization
Sheep Brain Dissection
 Sheep Brain Dissection Mammalian brains have many features in common. Human brains may not be available, so sheep brains often are dissected as an aid to understanding the mammalian brain since he general
Sheep Brain Dissection Mammalian brains have many features in common. Human brains may not be available, so sheep brains often are dissected as an aid to understanding the mammalian brain since he general
Biological Bases of Behavior. 3: Structure of the Nervous System
 Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
J. Neurol. Neurosurg. Psychiat., 1953, 16, 227.
 J. Neurol. Neurosurg. Psychiat., 1953, 16, 227. THE ARNOLD-CHIARI MALFORMATION RADIOLOGICAL EXAMINATION WITH THE " ZIEDSES DES PLANTES " PROCEDURE BY Flom the Neurosurgical Department of the Neurological
J. Neurol. Neurosurg. Psychiat., 1953, 16, 227. THE ARNOLD-CHIARI MALFORMATION RADIOLOGICAL EXAMINATION WITH THE " ZIEDSES DES PLANTES " PROCEDURE BY Flom the Neurosurgical Department of the Neurological
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE
 Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE") Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
MR Imaging of Hindbrain Deformity in Chiari II Patients with and Without Symptoms of Brainstem Compression
 293 MR Imaging of Hindbrain Deformity in Chiari II Patients with and Without Symptoms of Brainstem Compression John T. Curnes 2 W. Jerry Oakes 3 Orest B. Boyko We examined the MR appearance of the hindbrain
293 MR Imaging of Hindbrain Deformity in Chiari II Patients with and Without Symptoms of Brainstem Compression John T. Curnes 2 W. Jerry Oakes 3 Orest B. Boyko We examined the MR appearance of the hindbrain
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Lecture 4 The BRAINSTEM Medulla Oblongata
 Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
Chiari FAQ's. 1. What is a Chiari Malformation?
 Chiari FAQ's These FAQ's are for informational purposes only and in no way represent an attempt to provide medical advice. This information may or may not apply to your case and anyone with a question
Chiari FAQ's These FAQ's are for informational purposes only and in no way represent an attempt to provide medical advice. This information may or may not apply to your case and anyone with a question
Blood supply to the brain Blood brain barrier isolates neural tissue from general circulation
 The Brain and Cranial Nerves Objectives Name the major regions of the brain and describe their functions. Discuss the formation, circulation, and functions of the CSF. List the main components of the medulla
The Brain and Cranial Nerves Objectives Name the major regions of the brain and describe their functions. Discuss the formation, circulation, and functions of the CSF. List the main components of the medulla
Abstract Objective: Multiple surgical strategies exist for the management of the symptomatic Chiari II malformation. To date, no comprehensive
 Childs Nerv Syst (2004) 20:375 381 DOI 10.1007/s00381-004-0969-4 R E V I E W P A P E R R. Shane Tubbs Treatment and management of the Chiari II W. Jerry Oakes malformation: an evidence-based review of
Childs Nerv Syst (2004) 20:375 381 DOI 10.1007/s00381-004-0969-4 R E V I E W P A P E R R. Shane Tubbs Treatment and management of the Chiari II W. Jerry Oakes malformation: an evidence-based review of
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Skull-2. Norma Basalis Interna. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 Skull-2 Norma Basalis Interna Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the skull is divided into
Skull-2 Norma Basalis Interna Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the skull is divided into
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible:
 NERVOUS SYSTEM The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible: the neuron and the supporting cells ("glial cells"). Neuron Neurons
NERVOUS SYSTEM The neurvous system senses, interprets, and responds to changes in the environment. Two types of cells makes this possible: the neuron and the supporting cells ("glial cells"). Neuron Neurons
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD
 Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Enhancement of Cranial US: Utility of Supplementary Acoustic Windows and Doppler Harriet J. Paltiel, MD Boston Children s Hospital Harvard Medical School None Disclosures Conventional US Anterior fontanelle
Disclosures None. Common Neurosurgical Problems Seen in Office Encounters. Macrocephaly Low Back Pain Sacral Dimple Concussion Chiari Malformation
 Common Neurosurgical Problems Seen in Office Encounters When to Manage, When to Refer Andrew Jea MD FAAP Professor and Chief of Pediatric Neurosurgery Riley Hospital for Children Indiana University School
Common Neurosurgical Problems Seen in Office Encounters When to Manage, When to Refer Andrew Jea MD FAAP Professor and Chief of Pediatric Neurosurgery Riley Hospital for Children Indiana University School
Central nervous system (CNS): brain and spinal cord Collections of cell body and dendrites (grey matter) are called nuclei/nucleus Nucleus can also
: brain and spinal cord Collections of cell body and dendrites (grey matter) are called nuclei/nucleus Nucleus can also") Chapter 3 Part 1 Orientation Directions in the nervous system are described relatively to the neuraxis An imaginary line drawn through the center of the length of the central nervous system, from the bottom
Chapter 3 Part 1 Orientation Directions in the nervous system are described relatively to the neuraxis An imaginary line drawn through the center of the length of the central nervous system, from the bottom
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16
 The Brain Chapter 14 and select portions of Chapter 16") Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Unit 12a: The Nervous System The Brain. MDL231 Principle of Anatomy
 Unit 12a: The Nervous System The Brain MDL231 Principle of Anatomy The Brain - Overview Cerebrum T PP H midbrain Cerebellum pons m.o. Brain stem medulla oblongata (M.O.) pons midbrain (mesencephalon) Diencephalon
Unit 12a: The Nervous System The Brain MDL231 Principle of Anatomy The Brain - Overview Cerebrum T PP H midbrain Cerebellum pons m.o. Brain stem medulla oblongata (M.O.) pons midbrain (mesencephalon) Diencephalon
Cerebral hemisphere. Parietal Frontal Occipital Temporal
 Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
CT - Brain Examination
 CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
CT - Brain Examination Submitted by: Felemban 1 CT - Brain Examination The clinical indication of CT brain are: a) Chronic cases (e.g. headache - tumor - abscess) b) ER cases (e.g. trauma - RTA - child
What Every Spine Surgeon Should Know About Neurosurgical Issues
 What Every Spine Surgeon Should Know About Neurosurgical Issues Amer Samdani, MD Chief of Surgery Shriners Hospitals for Children Philadelphia, PA Objectives Main intraspinal lesions Chiari malformation
What Every Spine Surgeon Should Know About Neurosurgical Issues Amer Samdani, MD Chief of Surgery Shriners Hospitals for Children Philadelphia, PA Objectives Main intraspinal lesions Chiari malformation
Chapter 18: The Brain & Cranial Nerves. Origin of the Brain
 Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
stored information, making decisions, and taking action. 1. It is also the center for intellect, emotions, behavior, and memory.
 Chapter 14 - Outline I. INTRODUCTION A. The brain is the center for registering sensations, correlating them with one another and with stored information, making decisions, and taking action. 1. It is
Chapter 14 - Outline I. INTRODUCTION A. The brain is the center for registering sensations, correlating them with one another and with stored information, making decisions, and taking action. 1. It is
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Skull-2. Norma Basalis Interna Norma Basalis Externa. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
Chapter 14. The Brain Meninges and Cerebral Spinal Fluid
 Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms.
 RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
Human Anatomy. Brain and Cranial Nerves
 Human Anatomy Brain and Cranial Nerves 1 Brain and Cranial Nerves An adult brain weighs between 1.35 and 1.4 kilograms (kg) (around 3 pounds) and has a volume of about 1200 cubic centimeters (cc). Brain
Human Anatomy Brain and Cranial Nerves 1 Brain and Cranial Nerves An adult brain weighs between 1.35 and 1.4 kilograms (kg) (around 3 pounds) and has a volume of about 1200 cubic centimeters (cc). Brain
Anatomy, Terminology and Treatment in Pediatric Neurosurgery Part I
 Anatomy, Terminology and Treatment in Pediatric Neurosurgery Part I John Ragheb, MD, FACS, FAAP Professor of Neurosurgery and Pediatrics, Affiliated Faculty of University of Miami, Miller School of Medicine
Anatomy, Terminology and Treatment in Pediatric Neurosurgery Part I John Ragheb, MD, FACS, FAAP Professor of Neurosurgery and Pediatrics, Affiliated Faculty of University of Miami, Miller School of Medicine
Cranial Vertebral Junction Anatomy and Pathology
 Cranial Vertebral Junction Anatomy and Pathology October 2016 Mary Scanlon MD FACR Goals and Objective Goal-Understand CVJ anatomy & pathology Objective-After attending this lecture you will be able to
Cranial Vertebral Junction Anatomy and Pathology October 2016 Mary Scanlon MD FACR Goals and Objective Goal-Understand CVJ anatomy & pathology Objective-After attending this lecture you will be able to
Dandy-Walker syndrome: different modalities of treatment and outcome in 42 cases
 Child s Nerv Syst (2001) 17:348 352 DOI 10.1007/s003810000425 ORIGINAL PAPER Raj Kumar Manoj Kumar Jain Devendra Kumar Chhabra Dandy-Walker syndrome: different modalities of treatment and outcome in 42
Child s Nerv Syst (2001) 17:348 352 DOI 10.1007/s003810000425 ORIGINAL PAPER Raj Kumar Manoj Kumar Jain Devendra Kumar Chhabra Dandy-Walker syndrome: different modalities of treatment and outcome in 42
Decompression of the spinal subarachnoid space as a solution for syringomyelia without Chiari malformation
 (2002) 40, 501 ± 506 ã 2002 International Society All rights reserved 1362 ± 4393/02 $25.00 www.nature.com/sc Original Article Decompression of the spinal subarachnoid space as a solution for syringomyelia
(2002) 40, 501 ± 506 ã 2002 International Society All rights reserved 1362 ± 4393/02 $25.00 www.nature.com/sc Original Article Decompression of the spinal subarachnoid space as a solution for syringomyelia
Gross Morphology of Spinal Cord
 Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
Gross Morphology of Spinal Cord Lecture Objectives Describe the gross anatomical features of the spinal cord. Describe the level of the different spinal segments compared to the level of their respective
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
4The head basic anatomy and physiology
 Hene_Ch04.qxd 8/30/04 2:47 AM Page 108 108 THE HEAD BASIC ANATOMY AND PHYSIOLOGY 4The head basic anatomy and physiology The scalp Anatomists describe the SCALP as having five layers: Skin, Subcutaneous
Hene_Ch04.qxd 8/30/04 2:47 AM Page 108 108 THE HEAD BASIC ANATOMY AND PHYSIOLOGY 4The head basic anatomy and physiology The scalp Anatomists describe the SCALP as having five layers: Skin, Subcutaneous
Adult - Cerebrovascular. Adult - Cranio-Cervical Junction. Adult - Epilepsy. Adult - Hydrocephalus
 list for SET and IMG Neurosurgery Adult - Cerebrovascular Aneurysm - Clipping: Anterior circulation Aneurysm - Clipping: Posterior circulation AVM excision Carotid endarterectomy Carotid trapping Cavernoma
list for SET and IMG Neurosurgery Adult - Cerebrovascular Aneurysm - Clipping: Anterior circulation Aneurysm - Clipping: Posterior circulation AVM excision Carotid endarterectomy Carotid trapping Cavernoma