PROSTHETIC. V PROSTHETIC.V
|
|
|
- Adrian Thornton
- 5 years ago
- Views:
Transcription
1 PROSTHETIC. V PROSTHETIC.V
2 VALVE TYPE The valve types now implanted include: 1-bileaflet and tilting disc mechanical valves, 2-stented porcine and pericardial xenografts, 3-stentless porcine xenografts, 4-cadaveric homografts, 5-autografts (Ross procedure).

3
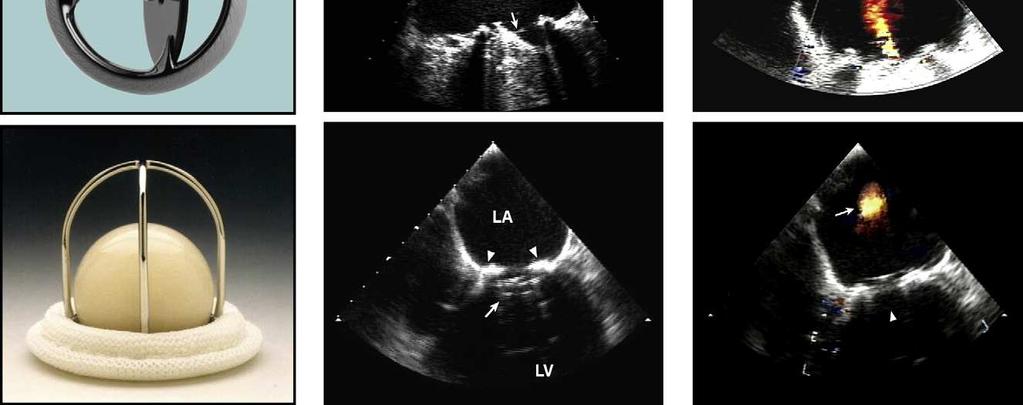
4 TYPES Examples of bileaflet, single-leaflet, and caged-ball mechanical valves and their transesophageal echocardiographic characteristics taken in the mitral position in diastole (middle) and in systole (right). The arrows in diastole point to the occluder mechanism of the valve and in systole to the characteristic physiologic regurgitation observed with each valve


5
6 TYPES Examples of stented, stentless, and percutaneousbiologic valves and their echocardiographicfeatures in diastole (middle) and in systole (right) as seen by TEE. The stentlessvalve is inserted by the root inclusion technique. Mild perivalvularar in the percutaneousvalve is shown by arrow. The percutaneousbiologic valve is currently for investigational use only.
7 NATURE OF TYPES By their design, almost all replacement valves are obstructive compared with normal native valves The degree of obstruction varies with the type and size of the valve. Thus, it may be difficult to differentiate obstructive hemodynamicsdue to valve design from those of mild obstruction observed with pathologic changes and from prosthesis-patient mismatch (PPM)
8 physiologic regurgitation Most mechanical.vand many biologic.vare associated with trivial or mild transprosthetic regurgitation. The pattern of this physiologic regurgitation varies with the design of the replacement valve
9 TYPES There is no ideal valve, and all prosthetic valves are prone to dysfunction
10 Biologic. v -stented porcine and pericardial xenografts, -stentless porcine xenografts, -cadaveric homografts, -autografts (Ross procedure).
11 Biologic. v The most frequently implanted biologic valve is a stented xenograft. The valve may be an entire porcine valve or a composite from 2 or 3 individual pigs The cusps of stented pericardial xenografts are made from pericardium Usually, pericardium is bovine,but pericardiumof other species has also been used
12 Biologic. v Stentlessxenograftgraft valves usually consist of a preparation of porcine aorta Homograft valves consist of cryopreserved human aortic or, less commonly, pulmonary valves. Stentlessvalves were introduced to increase the effective orifice area (EOA). It was also hoped that less stresses on the cusps & better durability and less thrombosis
13 SIZE Usually, the reported size of a prosthesis refers to the outer diameter of the valve ring, in millimeters. In a study comparing valve size as stated by the manufacturer against a modeled patient tissue annulus provided by machined polypropylene blocks, the patient tissue annulus diameter ranged from 3.5 mm smaller to 3.0 mm larger than the labeled size.
14 POSITION The various valve types can differ also by their implantation position relative to the valve annulus. This is mainly in the aortic site. Valve implantation can be intra-annular, partially supra-annular, or wholly supra-annular. The supra-annular position is designed to lift as much of the replacement valve above the annulus to maximize the orifice area available for flow. The maximum label size implantable may then be limited by the diameter of the aortic root or the position of the coronary ostia
15 Percutaneous valves Percutaneousvalves have been implanted in the pulmonary and aortic positions
16 apicoaortic conduit This operation interposes a fabric conduit containing a bioprosthetic or mechanical valve between the LV apex and descending aorta. Postoperative evaluation focuses on evaluation of the apical cannulafor absence of thrombus and adequate flow
17 2D Rocking motion of a replacement valve is almost invariably a sign of a large dehiscence in the aortic position. For valves in the mitral position, however, retention of the posterior or both the anterior and posterior native leaflets can allow increased mobility of a normal prosthesis
18 pressure recovery can occur in two regions: (1) downstream of a valve (2) within some prosthetic valves, typically bileaflet or caged-ball valves In the first scenario, as flow expands into the wider lumen beyond a valve, velocity and kinetic energy will decrease and pressure will be recovered
19 pressure recovery The pressure gradient measured directly by catheter therefore decreases as the catheter port is moved downstream from the prosthetic orifice and will generally be smaller than the gradient estimated from maximal CW Doppler velocity at the vena contracta the smallest area occupied by flow. The magnitude of this phenomenon is generally small, except in which the aorta is <30 mm in diameter, an infrequent finding in adults.
20 pressure recovery In the case of mechanical bileafletprostheses the particular design of the valve may cause a separate phenomenon of pressure recovery at the level of the valve. This is may else be observed in caged-ball prostheses.
21 pressure recovery The smaller central orifice in bileafletvalves may give rise to a high-velocity jet that corresponds to a localized pressure drop that is largely recovered once the central flow reunites with flows originating from the two lateral orifices
22 pressure recovery CW Doppler recording often includes this high-velocity jet, which leads to overestimation of gradients and thus underestimation of EOA compared with the invasive hemodynamic standard, particularly in smallprostheses and in high flow states
23 PPM PPM occurs when the EOA of the prosthesis is too small in relation to the patient s body size, resulting in abnormally high postoperative. Gradients increase exponentially when the indexed EOA is < 0.8 to 0.9 cm2/m2 PPM is considered to be hemodynamically: insignificant if the indexed EOA is > 0.85 cm2/m2, moderate if between 0.65 and 0.85 cm2/m2, severe if <0.65 cm2/m2
24 PPM The reported prevalence of moderate PPM varies between 20% and 70%, whereas that of severe PPM is between 2% and 11%. The main adverse clinical outcome ascribed to PPM is reduced short-term and long-term survival, particularly if associated with LV dysfunction
25 PPM There are some reports of lesser regression of LVH, increased incidence of late cardiac events, and less improvement in functional class, although other studies have found little effect. If PPMisanticipated, choosing an alternative prosthesis or considering aortic root enlargement surgery is advised
26 PPM PPM has also been described in the mitral position. It has been suggested that the indexed EOA of mitral prostheses should ideally be no less than 1.2 to 1.3 cm2/m2 to avoid abnormally high postoperative gradients
27 PPM Depending on the study, the reported prevalence for mitral PPM varies between 39% and 71% and was shown to be associated with persisting pulmonary hypertension and decreased long-term survival.
28 PPM Recent data suggest that PPM may not have similar detrimental effects in obese patients (body mass index > 30 kg/m2) compared with nonobese patients For similar body surface areas, obese patients tend to have lower cardiac output requirements.
29 DOPPLER It is not appropriate to use the PHT formula (220/PHT ) to estimate orifice area in prosthetic valves. This is valid only for moderate or severe stenoses with orifice areas < 1.5 cm2. For larger valve areas, the pressure half-time reflects atrial and LV compliance characteristics and loading conditions and has no relation to valve area
30 DOPPLER Doppler recordings should be performed at a sweep speed of 100 mm/s. Measurements should be taken over 1 to 3 cycles in sinus rhythm. In atrialfibrillation, Doppler measurements should be performed when possible during periods of physiologic heart rate (65-85 beats/min).
31 DOPPLER Averaging from 5 to 15 beats in atrial fibrillation has been suggested but is cumbersome and may still give an unrepresentative result, because cycle lengths may vary substantially
32 REGURGITATION Two types of physiologic regurgitation may be seen: a closing volume (a displacement of blood caused by the motion of the occluder) and true trivial or mild regurgitation at the hinges of the occluder
33 REGURGITATION The bileafletvalves typically have multiple jets located just inside the sewing ring, where the closed leaflets meet the housing, and centrally, where the closed bileafletsmeet each other. Regurgitation is increasingly reported in normal biologic valves, mainly because of increased sensitivity of current ultrasound machines. Stentlessvalves, including homograftsand autografts, are more likely than stented valves to have minor regurgitant jets. Percutaneousaortic valves may have small central and/or paravalvular regurgitation
34 Pathologic regurgitation Central or paravalvular Most pathologic central valvularregurgitation is seen with biologic valves, whereas paravalvularregurgitation is seen with either valve type and is frequently the site of regurgitation in mechanical valves
35 SMALL PARA.V.LEAK There is no evidence that they increase the risk for endocarditis, but on occasion, they may cause hemolytic anemia due to red cell destruction

36 PANNUS
37 AV High gradients may be seen with normally functioning valves with a small size, increased stroke volume, PPM, or valve obstruction. Conversely, a mildly elevated gradient in the setting of severe LV dysfunction may indicate significant stenosis
38 AV Recent data have shown that a cutoff of AT of 100 ms differentiates well between normal and stenotic prosthetic valves.
39 AV.DVI DVI is a dimensionless ratio of the proximal velocity in the LVOT to that of flow velocity through the prosthesis: DVI = V.LVOT / V.AV ( VTI ) DVI can therefore be helpful to screenfor valve dysfunction, particularly when the crosssectional area of the LVO tract cannot be obtained or valve size is not known. A DVI < 0.25 is highly suggestive of significant valve obstruction
40 DVI One must bear in mind that high velocity alone is not proof of intrinsic prosthetic obstruction and may be secondary to high flow or PPM. If the DVI is >0.25 and the jet shows early peaking of the velocity (AT < 100 ms),most likely, the valve is normal, particularly if the other quantitative parameters fall in the normal or intermediate Range. In this case, the high velocity is most likely because of high flow, PPM, or pressure recovery from a bileaflet or cagedball valve
41 AV Obstruction of the valve starts to be suspected when the DVI is <0.30 and is highly suggested if the DVI is <0.25 and the jet has a rounded contour, with late peaking of the velocity (AT > 100 ms). In a normal DVI of >0.30 but a rounded contour and an AT > 100 ms, prosthetic stenosisshould be considered, the reason for the elevated LVO velocity being either improper position of PW Doppler sample volume (too close to the valve, causing high velocity recording in the LVO) or subvalvular narrowing.
42 AV In the converse situation of a low DVI (<0.25) and a Nl contour of the jet & an AT < 100 ms, an improper LVO velocity recording is most likely the situation (sample volume position too far apical from the prosthesis).
43 AV Starr Edwards Caged ball BILEAFLET Carbomedics Bileaflet ATS Edwards Duromedics Bileaflet Edwards Mira Bileaflet St Jude Medical Regent Bileaflet TILTING Bjork-Shiley(Single tilting disc) Monostrut Bjork-Shiley Single tilting disc Omniscience Single tilting disc
44 AV BIOLOGIC : Baxter Perimount (Stented bovine) Biocor( Stentedporcine ) Extended Biocor( Stentless) Bioflo(Stented bovine pericardial) Carpentier Edwards Pericardial Stented bovine pericardial Carpentier Edwards Standard Stented porcine Cryolife(Stentless) Hancock (Stented porcine ) Ionescu-Shiley Stented bovine pericardial Medtronic Mosaic Stented porcine Prima Stentless
45 MV As a general rule, however, a peak E velocity < 1.9 m/s is likely to be normal in most patients with mechanical valves unless there is markedly depressed LV function. If the peak velocity is >1.9 m/s in a mechanical valve, one should consider a normally functioning valve with a high velocity versus prosthetic valve dysfunction (stenosisor regurgitation). This cutoff may be slightly higher in some bioprostheticvalves.
46 MV Because MR also increases transmitralflow velocity, patients with elevated peak E velocity may require TEE to exclude significant MR.
47 MV.MG Mean gradient is also useful in assessing prosthetic mitral valve function and is normally < 5 to 6 mm Hg. However, values up to 10 and 12 mm Hg have been reported in normally functioning Starr- Edwards and St Jude bileafletprostheses, respectively, highlighting the need to compare serial values in the same patient over time
48 MV.MG High mean gradients may be due to hyperdynamicstates, tachycardia or PPM, regurgitation, or stenosis. The mean gradient is significantly affected by heart rate, so the HR at which the MG is measured should always be reported
49 MV.PHT A large rise in PHT on serial studies or a markedly prolonged single measurement (>200ms) may be a clue to the presence of prosthetic valve obstruction, because the pressure half-time seldom exceeds130 ms across a normally functioning mitral valve prosthesis
50 DVI The VTI.MV/VTI.LVOT ratio would be elevated either in stenosis(increased velocity across the valve) or regurgitation (increased velocity across the valve and decreased velocity in the LVOT). In mechanical valves, a VTI.MV/VTILVOT < 2.2 is most often normal
51 MV BILEAFLETS CarbomedicsBileaflet St Jude Medical Bileaflet On-X Bileaflet DuromedicsBileaflet
52 MV TILTING Bjork-Shiley Tilting disc Bjork-Shiley monostrut Tilting disc Medtronic- Hall Tilting disc Omnicarbon Tilting disc
53 MV BIO Biocor Stentless bioprosthesis Bioflo pericardial Stented bioprosthesis Carpentier- Edwards Stented bioprosthesis Hancock I & 2 Stented bioprosthesis Ionescu-Shiley Stented bioprosthesis Mitroflow Stented bioprosthesis
54 Findings suspicious for prosthetic pulmonary valve stenosis Cusp or leaflet thickening or immobility Narrowing of forward color map Peak velocity through the prosthesis > 3 m/s or >2 m/s through a homograft* Increase in peak velocity on serial studies Impaired RV function or elevated RV systolic pressure
55 PV normal homograftshave a peak velocity < 2.5 m/s (mean gradient < 15 mm Hg), and normal xenograftshave a peak velocity < 3.2 m/s (mean gradient < 20 mm)
56 TV Obstruction is also suggested on CW Doppler by an E velocity > 1.7m/s, mean gradient > 6 mm Hg, or pressure half-time > 230 ms
57 PROSTHETIC.VHD CLASS I A bioprosthesisis recommended in patients of any age for whom 1-anticoagulant therapy is contraindicated 2-cannot be managed appropriately 3-is not desired
58 PROSTHETIC.VHD Class IIa 1. A mechanicalprosthesis is reasonable for AVR or MVR in patients less than 60 years of age who do not have a contraindication to anticoagulation 2. A BIOprosthesisis reasonable in patients more than 70 years of age 3. Either a bioprostheticor mechanical valve is reasonable in patients between years of age
59 PROSTHETIC.VHD Class IIb 1. AVR by a pulmonary autograft(the Ross procedure), when performed by an experienced surgeon, may be considered in young patients when VKA anticoagulation is contraindicated or undesirable
60 MECHANICAL PROSTHETIC.VHD WARFARIN + ASA( LIFE LONG)>>INR=2.5 INR = 3 IN: 1-MVR 2-AVR + AF/LOW LVEF/HxOF TE 3- OLD VALVE,,CAGE BALL
61 BIO.PROSTHESIS CLASS IIa BIO.PROSTHESIS OR REPAIR ASA LIFE LONG WRAFARIN IN BIO.MVR or REPAIR FOR 3MO//INR= CLASS IIb WARFARIN FOR BIO.AVR ADITION OF PLAVIX TO ASA FOR 6 mo IN TAVI
62 Bridging Therapy for Prosthetic Valves CLASS I 1-MINOR procedures (such as dental extractions or cataract removal) with LOW bleeding risk: Continuation of WARFARIN. 2-major surgery without bridging Tx in : AVR WITH NO RF & BILEAFLET.V 3-bridging Tx IN MVR/AVR+RF/OLDER VALVE
63 Bridging Therapy for Prosthetic Valves CLASS IIa 1-FFP or PCC is reasonable with mechanical valves receiving WARFARIN IN emergency noncardiacinvasive surgery 2-FFP or PCC in patients with mechanical valves and uncontrollable bleeding who require reversal of anticoagulation
64 Prosthetic Valve Thrombosis TTE & TEE CLASS I FLOUROSCOPY CLASS IIa Class IIa 1.Fibrinolytic Tx for thrombosed L-sided prosthetic.v IF: recent onset (<14 days) recent onset (<14 days) FC I to II symptoms small thrombus (<0.8 cm2) otherwise SURGERY 2. Fibrinolytic therapy is reasonable for thrombosed rightsided prosthetic heart valves (FIRST OR AFTER HEPARIN Tx)
65 Prosthetic Valve Stenosis 1. Repeat valve replacement is indicated for severe & symptomaticprosthetic valve stenosis.
66 Prosthetic Valve Regurgitation Class I severe( trans or para) valvularregurgitation with intractable hemolysis or HF:Surgery ClassIIa Percutaneousrepair of paravalvularregurgitation is reasonable in patients with prosthetic heart valves and intractable hemolysisor NYHA class III/IV HF who are at high risk for surgery and have anatomic features suitable for catheter-based therapy when performed in centers with expertise in the procedure
67 Prosthetic Valve Regurgitation Class IIa 1. Surgery for operable patients with severesym or asymptomatic bioprosthetic regurgitation
68 IE A-2 TIMES B/C IN AT RISK PATIENTS WITH unexplained fever for more than 48 hours or newly diagnosed left-sided valve regurgitation B-TEE is recommended in all patients with known or suspected IE when TTE is nondiagnostic, when complications have developed or are clinically suspected, or when intracardiac device leads are present
69 IE.Tx Class IIa 1. It is reasonable to temporarily discontinue anticoagulation in patients with IE who develop CNS symptoms compatible with embolism orstroke regardless of the other indications for anticoagulation (AT THE TIME OF DIAGNOSIS OF IE IS CLASS IIb)
70 SURGERY FOR IE CLASS I Early in patients with IE who present with: 1-valve dysfunction resulting in HF 2-left-sided IE caused by Staph aureus, fungal, or other highly resistant organisms 3-IE complicated by heart block, annular or aortic abscess, or destructive penetrating lesions 4-persistent bacteremia or fevers more than 5 to 7 days after onset of appropriate Tx 6-Complete removal of PPM/ICD( leads and the generator) as part of the early management plan in documented DEVICE IE (WITHOUT DEVICE.INV/under V. surgery ) IS CLASS IIa
71 RECURENT IE prosthetic V.IE >>>Tx>>>Relapsing without other identifiable source for portal of infection>>>early SURGERY is class I Early surgery in patients with IE with recurrent emboli and persistent vegetations despite appropriate antibiotic herapy>>>class IIa
72 IE Class IIb 1. Early surgery in patients with native V.IE WITH mobile vegetations greater than 10 mm in length (with or without clinical evidence of embolic phenomenon)
73 PREGNANCY II a 1-SEVERE MS+SYMPTOMATIC FC 3-4>>>PTMC & FC 4 NOT SUITABLE FOR PTMC>>SURGERY 2-AVR IN SYMPTOMATIC FC 3-4&SEVERE AS
74 Prosthetic Valves in Pregnancy 1-WARFARIN in 1 st trimester(dose<5mg) >>>IIa 2-Dose-adjusted continuous intravenous UFH & ENOXA in replace of W (if dose>5mg) in 1 st trimester >>>IIa otherwise: If W dose<5mg >>>>IIb 3-LMWH to pregnant patients with mechanical prostheses WITHOUT anti-xalevels monitoring 4 to 6 hours after administration>>>iii
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Echo Evaluation of a Mitral Valve Prostheses Sunday, February 14, :50 2:10 PM 20 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ Echo Evaluation of a Mitral Valve Prostheses Sunday, February 14, 2016 1:50 2:10 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t
2016 ASE State of the Art Echocardiography Course Tucson, AZ Echo Evaluation of a Mitral Valve Prostheses Sunday, February 14, 2016 1:50 2:10 PM 20 min 1 M U H A M E D S A R I Ć, M D, P H D D i r e c t
A Practical Approach to Prosthetic Valves
 A Practical Approach to Prosthetic Valves Bonita Anderson DMU (Cardiac), MApplSc (Med Ultrasound), ACS, AMS, FASE https://doi.org/10.1161/circulationaha.108.778886 Disclosures None 1 Know the Product Know
A Practical Approach to Prosthetic Valves Bonita Anderson DMU (Cardiac), MApplSc (Med Ultrasound), ACS, AMS, FASE https://doi.org/10.1161/circulationaha.108.778886 Disclosures None 1 Know the Product Know
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves
 Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Hemodynamics Benefit of Supra-Annular Design in Failed Bio-Prosthetic Valves Speaker's name: I have the following potential conflicts of interest to report: Proctorship for Medtronic Agenda Failure modes
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Patient/prosthesis mismatch: how to evaluate and when to act?
 Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Patient/prosthesis mismatch: how to evaluate and when to act? Svend Aakhus, MD, PhD Oslo University Hospital, Norway Disclosures: No conflict of interest Types of aortic valve prostheses (AVR) Mechanical
Heart Valves: Before and after surgery
 Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Heart Valves: Before and after surgery Tim Sutton, Consultant Cardiologist Middlemore Hospital, Auckland Auckland Heart Group Indications for intervention in Valvular disease To prevent sudden death and
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Spotlight on valvular heart disease guidelines. Prosthetic heart valves. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
CoreValve in a Degenerative Surgical Valve
 CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
CoreValve in a Degenerative Surgical Valve Ran Kornowski, MD, FESC, FACC Chairman Department of Cardiology Rabin Medical Center, Petach Tikva, Israel Disclosure Statement of Financial Interest I, Ran Kornowski,
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
PRINCIPLES OF ENDOCARDITIS
 015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
Management of Difficult Aortic Root, Old and New solutions
 Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Management of Difficult Aortic Root, Old and New solutions Hani K. Najm MD, Msc, FRCSC,, FACC, FESC Chairman, Pediatric and Congenital Heart Surgery Cleveland Clinic Conflict of Interest None Difficult
Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
 Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
Hans R. Figulla, M.D., PhD ; Ali Hamadanchi, M.D. Medicine, Pneumology Universitity Hospital, Jena, Germany Successful Percutaneous Closure of Mitral Bioprosthetic Paravalvular Leak Using Figulla ASD Occluder
How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, :00 11:25 PM 25 min
 2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
2016 ASE State of the Art Echocardiography Course Tucson, AZ How Do I Evaluate a Patient Being Considered for TAVR? Sunday, February 14, 2016 11:00 11:25 PM 25 min 1 M U H A M E D S A R I Ć, M D, P H D
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Experience with 500 Stentless Aortic Valve Replacements
 Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
Experience with 500 Stentless Aortic Valve Replacements Dimitrios C. Iliopoulos, MD Cardiac Surgeon Ass. Professor of Surgery University of Athens, School of Medicine I declare no conflict of interest
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim
 or AoV plasty- Kyung-Hwan Kim") 42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
42yr Old Male with Severe AR Mild LV dysfunction s/p TOF -AV Replacement(tissue valve) or AoV plasty- Kyung-Hwan Kim Current Guideline for AR s/p TOF Surgery is reasonable in adults with prior repair of
Update on Oral Anticoagulation for Mechanical Heart Valves
 Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Update on Oral Anticoagulation for Mechanical Heart Valves Douglas C. Anderson, Pharm.D., D.Ph. Professor and Chair Dept. of Pharmacy Practice Cedarville University School of Pharmacy OHIO SOCIETY OF HEALTH-SYSTEM
Valvular heart disease (VHD) is present in 2.5% of the
 is present in 2.5% of the") 2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
2017 Focused Update for Management of Patients With Valvular Heart Disease: Summary of New Recommendations Richard Matiasz, MD; Vera H. Rigolin, MD Valvular heart disease (VHD) is present in 2.5% of the
Case. 15-year-old boy with bicuspid AV Severe AR with moderate AS. Ross vs. AVR (or AVP)
") Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
Case 15-year-old boy with bicuspid AV Severe AR with moderate AS Ross vs. AVR (or AVP) AMC case 14-year-old boy with bicuspid AV Severe AS with mild AR Body size Bwt: 55 kg, Ht: 154 cm, BSA: 1.53 m 2 Echocardiography
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD
 2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
2017 Cardiovascular Symposium CARDIAC SURGERY UPDATE: SMALLER INCISIONS AND LESS COUMADIN DAVID L. SAINT, MD David L Saint M.D. Tallahassee Memorial Hospital Southern Medical Group Division of Cardiothoracic
PPM: How to fit a big valve in a small heart
 PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
PPM: How to fit a big valve in a small heart Hani K. Najm MD, Msc, FRCSC, FRCS (Glasgow), FACC, FESC King Abdulaziz Cardiac Centre National Guard Health Affairs Riyadh, Saudi Arabia GHA meeting Muscat
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute
 Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Mechanical vs. Bioprosthetic Aortic Valve Replacement: Time to Reconsider? Christian Shults, MD Cardiac Surgeon, Medstar Heart and Vascular Institute Assistant Professor, Georgetown School of Medicine
Management of Patients With Valvular Heart Disease. ACC/AHA Pocket Guidelines
 ACC/AHA Pocket Guidelines Management of Patients With Valvular Heart Disease A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines July 2000 ACC/AHA
ACC/AHA Pocket Guidelines Management of Patients With Valvular Heart Disease A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines July 2000 ACC/AHA
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
Mechanical heart valves and Anticoagulation. Dr. Alkesh ZALA Basic Physician trainee, Dept. of Cardiology, John Hunter hospital.
 Mechanical heart valves and Anticoagulation Dr. Alkesh ZALA Basic Physician trainee, Dept. of Cardiology, John Hunter hospital. Today s discussion: Case review The currently Available and most commonly
Mechanical heart valves and Anticoagulation Dr. Alkesh ZALA Basic Physician trainee, Dept. of Cardiology, John Hunter hospital. Today s discussion: Case review The currently Available and most commonly
RESEARCH AND REVIEWS: JOURNAL OF PHARMACOLOGY AND TOXICOLOGICAL STUDIES
 e-issn:2322-0139 RESEARCH AND REVIEWS: JOURNAL OF PHARMACOLOGY AND TOXICOLOGICAL STUDIES Comparative Evaluation of Safety Outcomes of Different Prosthetic Valves in Indian Subjects. Kama Raval 1 *, Reena
e-issn:2322-0139 RESEARCH AND REVIEWS: JOURNAL OF PHARMACOLOGY AND TOXICOLOGICAL STUDIES Comparative Evaluation of Safety Outcomes of Different Prosthetic Valves in Indian Subjects. Kama Raval 1 *, Reena
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Transcatheter Mitral Valve Replacement How Close Are We?
 Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Transcatheter Mitral Valve Replacement How Close Are We? Gregory Pavlides, MD, PhD, FACC, FESC Professor of Medicine Miscia Chair of Interventional Cardiology Director, Cardiac Catheterization Laboratories,
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques
 Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques Pablo Codner, Abid Assali, Hanna Vaknin-Assa, Katia Orvin, Ram Sharony, Leor Perl, Gabriel Greenberg, Marina Kupershmidt,
Treatment of Bio-Prosthetic Valve Deterioration Using Transcatheter Techniques Pablo Codner, Abid Assali, Hanna Vaknin-Assa, Katia Orvin, Ram Sharony, Leor Perl, Gabriel Greenberg, Marina Kupershmidt,
CARDIOLOGY GRAND ROUNDS
 CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
CARDIOLOGY GRAND ROUNDS Presentation: Speakers: Percutaneous Repair of Paravalvular Prosthetic Regurgitation Paul Sorajja, MD Director of the Center for Valve and Structural Heart Disease Minneapolis Heart
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Surgical Indications of Infective Endocarditis in Children
 2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain
 DOI: 10.1111/echo.13357 CASE REPORT Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain Sathish Chikkabyrappa
DOI: 10.1111/echo.13357 CASE REPORT Subacute left ventricular outflow tract obstruction after transapical closure of a mitral paravalvular leak in the region of the aortomitral curtain Sathish Chikkabyrappa
The introduction of valve replacement surgery in the early
 Valvular Heart Disease: Changing Concepts in Disease Management Prosthetic Heart Valves Selection of the Optimal Prosthesis and Long-Term Management Philippe Pibarot, DVM, PhD; Jean G. Dumesnil, MD, FRCP(C)
Valvular Heart Disease: Changing Concepts in Disease Management Prosthetic Heart Valves Selection of the Optimal Prosthesis and Long-Term Management Philippe Pibarot, DVM, PhD; Jean G. Dumesnil, MD, FRCP(C)
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis
 Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Prosthesis-Patient Mismatch in High Risk Patients with Severe Aortic Stenosis in a Randomized Trial of a Self-Expanding Prosthesis George L. Zorn, III On Behalf of the CoreValve US Clinical Investigators
Para-valvular Leak Closure
 Para-valvular Leak Closure Antonios Halapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens, Greece Disclosures I and the HYGEIA Hospital «Heart Team» have received research and travel grants from
Para-valvular Leak Closure Antonios Halapas, MD, PhD, FESC THV & Hygeia Hospital Heart Team Athens, Greece Disclosures I and the HYGEIA Hospital «Heart Team» have received research and travel grants from
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns
 Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Questions of the webinar "Imaging in TAVI procedures" Answered by Andreas Hagendorff, Victoria Delgado and Bernard Cosyns 1. The incidence in AR I think that this question focuses on the incidence in AR
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz
 Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
Hani K. Najm MD, Msc, FRCSC FACC, FESC President Saudi Society for Cardiac Surgeons Associate Professor of Cardiothoracic Surgery King Abdulaziz Cardiac Centre Riyadh, Saudi Arabia Decision process for
How to Avoid Prosthesis-Patient Mismatch
 How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
How to Avoid Prosthesis-Patient Mismatch Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE, FESC Canada Research Chair in Valvular Heart Diseases INSTITUT UNIVERSITAIRE DE CARDIOLOGIE ET DE PNEUMOLOGIE DE QUÉBEC
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Iatrogenic pathology of the heart:
 Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
Iatrogenic pathology of the heart: Complications of mitral valve plasty and replacement Patrick Bruneval D pt of Pathology Hôpital Européen Georges Pompidou Enterprise Interest None Mitral valve surgery
Endocarditis and Its Complications: The Role of Echocardiography
 Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Cardiac catheterisation in AS
 AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
AORTIC STENOSIS MANAGEMENT OF VALVULAR AORTIC STENOSIS Dr Badri Paudel Third most common cardiovascular disease Most prevalent valvular heart disease in the world Commonest acquired valvular lesion with
Anticoagulation Therapy and Valve Surgery. Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon
 Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
Anticoagulation Therapy and Valve Surgery Dr Pau Kiew Kong Consultant Cardiothoracic Surgeon Outline of lecture 1. Type of Valve Surgery 2. Anticoagulation requirements 3. Mechanical (Metallic) prosthetic
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor. Cardiothoracic Radiology
 New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
New Cardiovascular Devices and Interventions: Non-Contrast MRI for TAVR Abhishek Chaturvedi Assistant Professor Cardiothoracic Radiology Disclosure I have no disclosure pertinent to this presentation.
Echo Emergencies. Outline. Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures
 Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair?
 TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
TAVI- Is Stroke Risk the Achilles Heel of Percutaneous Aortic Valve Repair? Elaine E. Tseng, MD and Marlene Grenon, MD Department of Surgery Divisions of Adult Cardiothoracic and Vascular and Endovascular
The St. Jude Medical Biocor Bioprosthesis
 The St. Jude Medical Biocor Bioprosthesis Clinical Evidence of Long-term Durability Long-term Biocor Experience A Review and Comparative Assessment Long-term Biocor Stented Tissue Valve Studies Twenty-year
The St. Jude Medical Biocor Bioprosthesis Clinical Evidence of Long-term Durability Long-term Biocor Experience A Review and Comparative Assessment Long-term Biocor Stented Tissue Valve Studies Twenty-year
Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis
 Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Page 1 of 5 Title of image and video article Sub-Acute Leaflet Thrombosis: A Reversible Cause of Aortic Stenosis Authors Athina Chasapi, Adam Hobbs, Theodore Velissaris & Benoy N Shah. Wessex Cardiac &
Management of Valvular Heart Disease. Management of Valvular Heart Disease
 Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
Management of Valvular Heart Disease The Task Force on the Management of Valvular Heart Disease (Eur Heart J 2007;28:230-68) Chairperson Task Force Members Alec Vahanian, Paris (France) Task Force Members
Surgical Treatment for Valvular Heart Disease
 Chapter 34 Surgical Treatment for Valvular Heart Disease Peter J. K. Starek Competency of the atrioventricular valves allows blood to enter the ventricles, where pressure is generated. When adequate systolic
Chapter 34 Surgical Treatment for Valvular Heart Disease Peter J. K. Starek Competency of the atrioventricular valves allows blood to enter the ventricles, where pressure is generated. When adequate systolic
PARAVALVULAR LEAK POST TAVR. Elements of Follow-up Post TAVR
 PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
PARAVALVULAR LEAK POST TAVR David S Rubenson MD FACC FASE Founding Director, Cardiac Non-Invasive Laboratory Scripps Clinic Medical Group number 1 Elements of Follow-up Post TAVR JACC CV Imag 2016;9:193
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Disclosures. ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech
 Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Disclosures ESC Munich 2012 Bernard Iung, MD Consultancy: Abbott Boehringer Ingelheim Bayer Servier Valtech Speaker s fee Edwards Lifesciences Sanofi-Aventis Decision Making in Patients with Multivalvular
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
TAVR for Valve-In-Valve. Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology
 TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
TAVR for Valve-In-Valve Brian O Neill Assistant Professor of Medicine Department of Medicine, Section of Cardiology Temple Hearth and Vascular Institute Disclosures: Consultant: Cardiac Assist TAVR for
Βαλβιδοπάθειες. Από ηις τειροσργικές ζηις διαδερμικές θεραπείες
 Βαλβιδοπάθειες. Από ηις τειροσργικές ζηις διαδερμικές θεραπείες Ιωάννης Δ. Κανονίδης Καθηγηηής Καρδιολογίας Α.Π.Θ. Γιεσθσνηης Β Καρδιολογικής Κλινικής Α.Π.Θ. Γενικό Νοζοκομείο Θεζζαλονίκης «Ιπποκράηειο»
Βαλβιδοπάθειες. Από ηις τειροσργικές ζηις διαδερμικές θεραπείες Ιωάννης Δ. Κανονίδης Καθηγηηής Καρδιολογίας Α.Π.Θ. Γιεσθσνηης Β Καρδιολογικής Κλινικής Α.Π.Θ. Γενικό Νοζοκομείο Θεζζαλονίκης «Ιπποκράηειο»
TAVI and Valve Replacement Thromboprophylaxis. Warren Prokopiw Pharmacy Resident
 TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
TAVI and Valve Replacement Thromboprophylaxis Warren Prokopiw Pharmacy Resident 2011-2012 Case Mr MW 76 yo Admitted 14 May for worsening CHF PMH: Aortic Stenosis, CVD (CABG x4 1980, PCI x3 stent 2008)
UNDERSTANDING YOUR HEART VALVE. Mosaic Tissue Valve
 UNDERSTANDING YOUR HEART VALVE Mosaic Tissue Valve A Message to You from the Employees at Medtronic, Inc. We understand that having heart valve replacement surgery is an important change in your life.
UNDERSTANDING YOUR HEART VALVE Mosaic Tissue Valve A Message to You from the Employees at Medtronic, Inc. We understand that having heart valve replacement surgery is an important change in your life.
Aortic valve replacement: is porcine or bovine valve better?
 Interactive CardioVascular and Thoracic Surgery Advance Access published December 4, 2012 Interactive CardioVascular and Thoracic Surgery (2012) 1 13 doi:10.1093/icvts/ivs447 BEST EVIDENCE TOPIC Aortic
Interactive CardioVascular and Thoracic Surgery Advance Access published December 4, 2012 Interactive CardioVascular and Thoracic Surgery (2012) 1 13 doi:10.1093/icvts/ivs447 BEST EVIDENCE TOPIC Aortic
Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC
 TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
TAVR: When Things go Wrong Federico M Asch MD, FASE MedStar Heart and Vascular Institute Georgetown University Washington, DC Disclosures Academic Echo Core Lab Abbott / St Jude Medical Edwards Medtronic
Transapical Transcatheter Aortic Valve Implantation in the Presence of a Mitral Prosthesis
 Journal of the American College of Cardiology Vol. 58, No. 7, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.04.023
Journal of the American College of Cardiology Vol. 58, No. 7, 2011 2011 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.04.023
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Learn and LiveSM. ACC/AHA Pocket Guideline. Based on the ACC/AHA 2006 Guideline Revision. Management of Patients With. Valvular Heart Disease
 Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2006 Guideline Revision Management of Patients With Valvular Heart Disease June 2006 Special thanks to Distributed through support from Medtronic
Late failure of transcatheter heart valves: An open question
 Late failure of transcatheter heart valves: An open question A comparison with surgically implanted bioprosthetic heart valves. A. Rashid The Cardiothoracic Centre Liverpool, UK. Conflict of Interest Statement
Late failure of transcatheter heart valves: An open question A comparison with surgically implanted bioprosthetic heart valves. A. Rashid The Cardiothoracic Centre Liverpool, UK. Conflict of Interest Statement
Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504
 Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Transcatheter valve-in-valve e implantation for aortic bioprosthetic valve dysfunction Interventional procedures guidance Published: 26 September 2014 nice.org.uk/guidance/ipg504 Your responsibility This
Hardware in the Chest - From VADs to Valves
 Hardware in the Chest - From VADs to Valves Cristina Fuss, MD Purpose Recognize the device Indication and function Cristina Fuss, MD Department of Diagnostic Radiology FROM VADS TO VALVES Implanting technique
Hardware in the Chest - From VADs to Valves Cristina Fuss, MD Purpose Recognize the device Indication and function Cristina Fuss, MD Department of Diagnostic Radiology FROM VADS TO VALVES Implanting technique
DISCLOSURE. Mitral ViV: why? Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? UW Medicine NONE.
 Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
Mitral Valve- in- Valve: Procedural Image Guidance with TEE, a Must Have or Nice to Have? G. Burkhard Mackensen, MD, PhD, FASE Professor & Chief, Division of Cardiothoracic Anesthesia, Department of Anesthesiology
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Choice of Prosthetic Heart Valve in Adults
 Journal of the American College of Cardiology Vol. 55, No. 22, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.10.085
Journal of the American College of Cardiology Vol. 55, No. 22, 2010 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2009.10.085
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated?
 Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Expanding Relevance of Aortic Valve Repair Is Earlier Operation Indicated? RM Suri, V Sharma, JA Dearani, HM Burkhart, RC Daly, LD Joyce, HV Schaff Division of Cardiovascular Surgery, Mayo Clinic, Rochester,
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative