Embryology The main pattern of the nerve complex course, branching pattern and the relationship is established during the first 3 months of
|
|
|
- Dwayne Hensley
- 5 years ago
- Views:
Transcription

1
2 Embryology The main pattern of the nerve complex course, branching pattern and the relationship is established during the first 3 months of gestation. during this period the muscles of facial expression also differentiated, became functional and actively contracted and the nerve is not full developed till the 4 years of age The facial n. develop with in the 2 nd pharyngeal arch at the same time of the external and middle ear developed ( 1 st arch ) so abnormality of the facial n. should be anticipated whenever there is associated malformation in the external or the middle ear
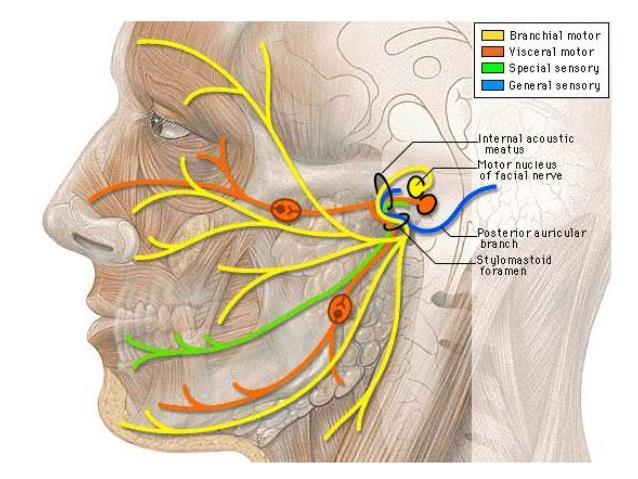
3 Anatomy 1. Nucleus lies deeply within the substance of the pons is that situation it is closely related to the V nucleus 2. Fibers travel a circuitous route at the first backward to encircle the V1 CN nucleus in the floor of the 4th ventricle and then forward through the pons to emerge on its surface then anterolateral to enter the petrous temporal bone 3. With in the cranial cavity it is closely related to the Viii CN 4. In the intrapetrous part, the facial n. and its sensory root accompany the Viii CN in the internal auditory canal her it has anastamotic with the vestibular nerve at the bottom of this canal, it enter the facial canal which at first runs laterally above the vestibule of the labyrinth until it turns backward through a right angle on the medial wall of the promontory and then fenestera vestibuli

4
5 At the medial wall of the aditus it curves downward to emerge on the inferior surface of temporal bone at the stylomastoid foramen to run forward within the parotid gland The N. supplies the following 1.Motor : muscles of facial expression, stapedius muscle, posterior belly of diagastric muscle, and stylohyoid muscle 2.Sensory : to the concha and to the parts behind the auricles 3.Autonmic fibers : for lacrimal, submandibular and sublingual glands together with glands at the nasal and oral cavities ( secretomotor and vasodilator ) 4.Speacial nerve taste via chorda tymapni branch to supply anterior 2/3 of the tongue
6
7
8 Types of nerve injury 1. Neurapraxia is defined as a reversible blockage of the transmission of nerve impulses due to pressure on the nerve fibers. Release of the pressure usually results in rapid and complete recovery of the function with no distal Wallerian degeneration 2. Axonotmesis is a more severe.injury and involves the blockage of axoplasmic flow Although endoneural tubules are preserved, distalwallerian 3. degeneration Neurotmesis occurs total N. transaction

9
10 the history of the onset of palsy, whether complete or incomplete, sudden or progressive progressive facial nerve palsy over a period of more than three weeks, or an incomplete facial nerve palsy that does not start to recover after three to six weeks, should make the clinician suspect an underlying neoplasm as the cause and should dictate the need for further investigations Ipsilateral recurrent facial nerve palsy can happen in idiopathic palsy, Melkersson Rosenthal syndrome and tumours


11 In Bell's palsy recurrence is 13 % and family history is 2.5 times more Melkersson-Rosenthal syndrome, a condition also characterized by alternating recurrent facial nerve palsy associated with facial oedema, fissured tongue and a positive family history
12 is almost always benign bilateral concurrent facial nerve paralysis is most probably associated with a systemic condition, such as Guillain Barre syndrome (most common), leukaemia, sarcoidosis, Lyme disease, rabies, infectious mononucleosis physical examination thorough head, neck, otological and cranial nerve examination is the absolute minimum required when evaluating facial nerve dysfunction complete or incomplete facial nerve palsy localize the lesion intracranial, intratemporal or textratemporal facial nerve palsy may be the first presentation of systemic illness If symptoms or signs of other cranial nerves deficits are present, a central or systemic cause should be suspected. Sparing of forehead movement is considered to be characteristic of a central lesion. However, it should be remembered that normal movement can also be seen in facial nucleus lesions and peripheral lesions of the temporal
13 House Brackmann system. It has become the most widely used scheme and has been endorsed by the American Academy of Otolaryngology Head and Neck Surgery. In the House Brackmann system, grade I is normal function, grade VI is complete absence of facial motor function and grades II V are intermediate

14
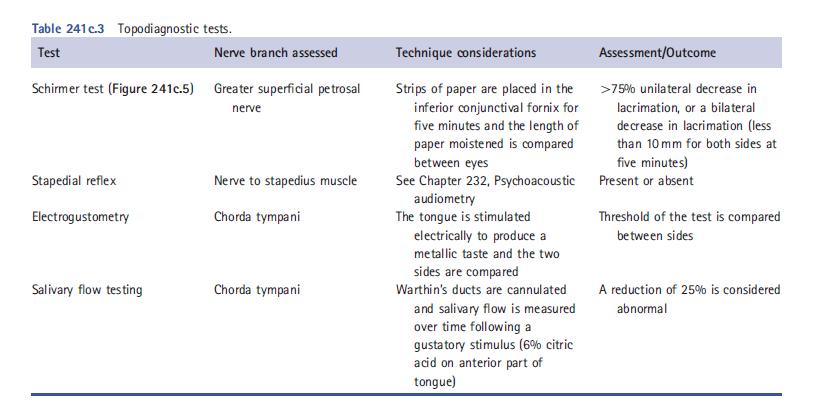
15 Special investigations There are 3 important issue when confronted with facial n palsy The cause The site of lesion The prognosis TOPODIAGNOSTIC TESTING These test aim to localize the site but has no prognostic value
16
17 Used mainly in complete facial n palsy not in incomplete facial n palsy Currently, the two most helpful are the ENoG and EMG Electroneuronography (ENoG) Consider the most valuable prognostic indicators among electrophysiological test and the main indication is acute onset complete facial paralysis Electromyography (EMG ) Electromyography records active motor unit potentials of the orbicularis oculi and orbicularis oris muscles during rest and voluntary contraction. EMG can be used to determine: _ if a nerve in question is in fact in continuity _ if there is evidence of Wallerian degeneration _ if there are early signs of reinnervation Intraoperative nerve monitoring Intraoperative monitoring includes continuous EMG measurement from peripheral facial muscle groups and electrical stimulation of the facial nerve itself or its branches to obtain a CMAP it has a place in cerebellopontine angle (CPA) tumour surgery, in revision mastoid and parotid surgery, and in surgery of congenital ear abnormalities. Other issues to consider are medicolegal issues
18 Ct scan The tympanic portion is probably easiest to identify on axial computed tomography (CT) scans at the level of the body of incus and its short process. From there on, it can be followed proximally and distally towards the labyrinthine and descending parts, respectively The descending or mastoid segment is best visualized in coronal or saggital views. MRI Owing to the rich perineural arteriovenous plexus which surrounds the facial nerve, enhancement may be observed normally on T1-weighted magnetic resonance imaging (MRI) with the use of contrast agents. It is usually observed in more than one segment, more commonly in the geniculate ganglion and the tympanic segments and it may enhance asymmetrically between
19 Causes of facial palsy Birth Moulding Forceps delivery Dystrophia myotonica Moebius syndrome (facial diplegia associated with other cranial nerve defects) Trauma Basal skull fracture Facial injuries Penetrating injury to middle ear Altitude paralysis (barotauma) Scuba diving (barotauma) Lightning Neurological Opercular syndrome (cortical lesion in facial motor area)
20 Infection Otitis externa Otitis media Mastoiditis Chicken pox Herpes zoster cephalicus (Ramsay Hunt syndrome) Encephalitis Poliomyelitis (type I) Mumps Infectious mononucleosis (glandular fever) Leprosy Coxsackie virus Malaria Syphilis Scleroma Tuberculosis Botulism Acute haemorrhagic conjunctivitis (enterovirus Mucormycosis Lyme disease
21 Metabolic Diabetes mellitus Hyperthyroidism Pregnancy Hypertension Acute porphyria Neoplastic Cholesteatoma VIIth nerve tumour Glomus jugulare tumour Leukaemia Meningioma Haemangioblastoma Sarcoma Carcinoma Anomalous sigmoid sinus Haemangioma of tympanum Facial nerve tumour Schwannoma Teratoma
22 Toxic Tetanus Diptheria Carbon monoxide Iatrogenic Mandibular block anaesthesia Anti-tetanus serum Vaccine treatment for rabies Post-immunization Parotid surgery Mastoid surgery Embolization Dental Idiopathic Bell s, familial Melkersson Rosenthal syndrome (recurrent alternating facial palsy, furrowed tongue, faciolabial oedema) Temporal arteritis Multiple sclerosis Myasthenia gravis
23 Idiopathic (Bell s) palsy Bell's palsy means facial paralysis that has signs and symptoms consistent with the disease and no cause was found It includes paralysis of paresis of all muscle groups on one side of the face; sudden onset; absence of signs of central nervous system disease; and absence of signs of ear or CPA disease Male to female ratio is equal Recurrence rate % 4.1 % has family history The etiology of Bell's palsy remains unclear although microcirculation failure of vasa nervorum, ischemic neuropathy, infection,genetics and immunological causes
24 process include herpes simplex virus type 1 (HSV-1), herpes simplex virus type 2 (HSV-2), human herpesvirus, varicella zoster virus (VZV), influenza B, adenovirus, Coxsackie virus and Epstein Barr virus (EBV ) The majority of patient will recover completely poor prognosis has been related to : complete paralysis at onset or incomplete paralysis with late onset of recovery, old age, a dry eye, abolished taste, absent stapedius reflex and postauricular pain. Normal function is usually regained within three months in about two-thirds of all patients. No further recovery is expected after a period of six months has elapsed
25 Exercises Predinsone 1mg /kg for 5 days then followed by ten days taper Acyclovir mg 5 times daily for 10 days Facial nerve disorder of viral origin VARICELLA ZOSTER VIRUS INFECTION (RAMSAY HUNT SYNDROME Ramsay Hunt syndrome is a peripheral facial nerve palsy accompanied by an erythematous vesicular rash on the ear (zoster oticus) or in the mouth, The mechanism of disease is reactivation of the latent VZV virus in the geniculate ganglion

26
27 The onset of palsy is preceded by pain which may persist and be excruciating. In a small proportion of patients, the facial palsy is accompanied by a sensorineural hearing loss The prognosis for Ramsay Hunt is worse than Bell s palsy. Persistent weakness is observed in percent of patients and only 10 percent recover completely after complete loss of function without treatment Treatment Same as Bell's palsy ( 2-3 weeks ) Predison 1 mg / kg / day for 5 days follwe by 10 days taper IV acyclovir 250 mg 3 times daily or 800 mg orally 5 times daily
28 Facial nerve trauma management of facial nerve paralysis following trauma is generally deferred until the patient is both medically and neurologically stable MAXILLOFACIAL TRAUMA stab wound or mandible fracture Treatment by end to end anastmosis or interposition graft TEMPORAL BONE TRAUMA Longitudinal fracture % facial palsy perigenigulate region Transverse fractures higher incidence of facial nerve paralysis (50 percent) and the labyrinthine and mastoid segments are most commonly involved
29 Middle ear and mastoid surgery The most common site of injury during middle ear or mastoid surgery is the distal tympanic segment including the second genu, followed by the mastoid segment If an injury to the facial nerve is recognized intraoperatively, exploration with decompression of proximal and distal segments of the nerve should be undertaken If more than 50 percent of the circumference has been disrupted it should be repaired with either direct suture or graft Parotid surgery Cerebellopontine angle tumour surgery
30 NEONATAL FACIAL NERVE INJURY Forceps delivery more than 90 % good prognosis Facial nerve paralysis as complications of the ear infection Otits media Facial n paralysis may complicate both acute and csom due to due direct involvement of the nerve by infection through Fallopian canal dehiscence or through Fallopian canal osteitis with bone erosion and nerve involvement MALIGNANT OTITIS EXTERNA Malignant otitis externa is an invasive Pseudomonas or Aspergillus infection of the ear canal which may lead to skull base osteomyelitis Facial palsy indicates advancing infection and invasion through the bony-cartilaginous junction and the fissures of Santorini, under the tympanic ring and posteriorly to the stylomastoid foramen.
31 Primary or secondary Primary facial nerve tumours are rare. Schwannomas and haemangiomas are the most frequent Any part of the nerve may be involved and multiple segments can be affected simultaneously Clinical features slowly progressive for n function, recurrent palsy and pain Treatment Poor facial n function resection and graft Good facial n function conservative treatment with regular imagining and clinical evaluation Secondary facial nerve tumors Squamous cells carcinoma or adenoid cycstic carcinoma of the parotid gland if the facial nerve is functioning preoperatively, the nerve can be preserved in most patients The facial nerve should be sacrificed if there is direct invasion of the tumour into the nerve where the tumour cannot be separated
32 Neurophysiology of pain pain as an unpleasant sensory or emotional experience associated with actual or potential tissue damage Most otalgia is mediated via unmyelinated pain fibres, which characteristically cause a diffuse dull ache. Myelinated fibres, such as supply skin or dental enamel, are associated with much better localization and easier diagnosis. Pain may be nociceptive or neuropathic
33 or central nervous systems or from an abnormality in the pain processing system. The resulting sharp, sudden, stabbing, lightning type of pain is typical of neuralgias Nerve supply of the ear 1.The auriculotemporal branch of V innervates the anterosuperior external canal and pinna, but also the temporomandibular joint. 2. The facial nerve makes a smaller contribution, providing some sensory input from the posterior tympanic membrane and external canal and the bowl of the concha. 3. Cranial nerve IX innervates the posterior external canal, meatus and tympanic membrane, but also the ipsilateral oropharynx. Its tympanic branch (Jacobson s nerve) forms the tympanic plexus, innervating the middle ear cleft. 4. The auricular branch of the vagus (Arnold s nerve) has a similar otologic distribution, but cranial nerve X has a vast dispersion to the viscera of the neck and even mediastinum 5. The upper cervical nerves C2 and C3, via the great auricular nerve and lesser occipital nerve, supply the cranial surface of the pinna, but also the skin and muscles of the neck and cervical spine. This rich innervation of the ear allows central misinterpretation of the origin of
34 Causes 1.from the ear 2. Refereed From the ear From the pinna Trauma : tear, laceration, bite Heamtaoma Infected eczema Perichondritis Infected basal or squamous cell carcinoma
35 b) from the meatus 1.impacted wax 2. impacted foreign body 3. otitis externa 4.Herps zoster oticus 5.keratosis obturance 6. furnculosis 7. malignant otitis externa 8. carcinoma
36 C) middle ear 1.bullous myringitis 2. traumatic perforation 3. OME 4.carcinoma 5. acute om 6. otitis baro trauma 7. hemotympanum
37 D)mastoid 1.acute mastoiditis 2. zygomatic mastoiditis 3. Bezold's abscess 4. complications of cholesteatoma 5. cholesterol granuloma E) inner ear 1.noise 2. menieres disease 3. tinnitus 4. vestibular shwannoma
38 Causes of referred otalgia Via the V cranial N Lesion of the teeth and jaw Impaction of molar tooth, apical abscess, dental caries, malocclusion, TMJ arthritis Lesion of salivary gland and duct ( acute infection or calculus ) Sphenopalatine neurolagia Lesion of the tongue, ulceration, carcinoma
39 B)via the X and IX CN 1. lesion of the oro and hypophayrnx. acute phayrngitis and tonsillitis.parapharyngeal and retropharyngeal abscess, quinsy. tonsillectomy, TB, neoplasm 2.Lesion of the tongue Ulceration, neoplasm, infection 3.elngated styloid process causing stretching of the glosspharyngeal CN 4. Glossphayrngeal neuralgia
40 C)via the 2 nd and 3 rd cervical spinal nerve Cervical disc lesions Arthritis of the cervical spine Fibrositis of the upper part of steronmastoid m The most common cause of refereed otalgia are impaction of lower molar tooth, infection or removal of tonsil, and dental malocclusion
41 How to arrive at diagnosis _ History Features suggestive of primary otalgia (due to ear disease): _ hearing loss; _ aural discharge; _ vertigo; _ unilateral rather than bilateral symptoms. Symptoms suggesting referred otalgia: _ pain on chewing/trismus; _ dysphagia/odynophagia; _ hoarseness; _ risk factors (smoking/alcohol history); _ neck swelling/goitre; _ cervical musculoskeletal symptoms; _ dental history/recent treatment. Features of neuropathic pain: _ radiation, e.g. to throat; _ typical time course/duration; _ quality of pain; _ trigger zone/precipitating factors, e.g. swallowing.
42 _ Examination Primary otalgia: _ inspection of ear and otoscopy; _ palpation for tenderness; _ aural examination with teleotoscope and microscope; _ tympanometry. Referred otalgia: _ cranial nerve (CN) examination, especially CN V, VII, IX and X; _ palpation of cervical lymphatic chain; _ assessment of cervical spine mobility/ tenderness; _ palpation of TMJ and pterygoid muscles; _ exclude trismus; _ dental inspection for caries, absent dentition and malocclusion; _ direct and fibreoptic examination of oropharynx and laryngopharynx; _ palpation of oropharynx to seek induration, trigger zone or styloid bone
43 Where diagnosis eludes the examiner, CT will detect skull base erosion, petrous apex disease and otherwise asymptomatic malignancies and demonstrate the styloid process. Enhanced MRI is superior in evaluating soft tissue disease, e.g. cranial nerve lesions, such as vestibular schwannoma or adenoid cystic carcinoma of the infratemporal fossa
Functional components
 Facial Nerve VII cranial nerve Emerges from Pons Two roots Functional components: 1. GSA (general somatic afferent) 2. SA (Somatic afferent) 3. GVE (general visceral efferent) 4. BE (Special visceral/branchial
Facial Nerve VII cranial nerve Emerges from Pons Two roots Functional components: 1. GSA (general somatic afferent) 2. SA (Somatic afferent) 3. GVE (general visceral efferent) 4. BE (Special visceral/branchial
Dr. Sami Zaqout Faculty of Medicine IUG
 Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
Auricle External Ear External auditory meatus The Ear Middle Ear (Tympanic Cavity) Auditory ossicles Internal Ear (Labyrinth) Bony labyrinth Membranous labyrinth External Ear Auricle External auditory
Facial Paralysis: Objectives: Discuss the anatomy of the facial nerve. Look at common patterns of facial nerve palsy
 Facial Paralysis: Objectives: Discuss the anatomy of the facial nerve Look at common patterns of facial nerve palsy Discuss imaging appearance of lesions that lead to facial paralysis. Lindell R. Gentry,
Facial Paralysis: Objectives: Discuss the anatomy of the facial nerve Look at common patterns of facial nerve palsy Discuss imaging appearance of lesions that lead to facial paralysis. Lindell R. Gentry,
4/30/2009 FN PARALYSIS HEMIFACIAL SPASM
 FN PARALYSIS HEMIFACIAL SPASM 1 Hemifacial spasm (Involuntary twitches) Etiology: Vascular loop compressing the FN at the root exit zone in the CPA = Neuro-vascular conflict Diagnosis: CT & MRI, Electrophysiology
FN PARALYSIS HEMIFACIAL SPASM 1 Hemifacial spasm (Involuntary twitches) Etiology: Vascular loop compressing the FN at the root exit zone in the CPA = Neuro-vascular conflict Diagnosis: CT & MRI, Electrophysiology
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR.
 The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
The Ear The ear consists of : 1-THE EXTERNAL EAR 2-THE MIDDLE EAR, OR TYMPANIC CAVITY 3-THE INTERNAL EAR, OR LABYRINTH 1-THE EXTERNAL EAR Made of A-AURICLE B-EXTERNAL AUDITORY MEATUS A-AURICLE It consists
Cranial Nerve VII - Facial Nerve. The facial nerve has 3 main components with distinct functions
 Cranial Nerve VII - Facial Nerve The facial nerve has 3 main components with distinct functions Somatic motor efferent Supplies the muscles of facial expression; posterior belly of digastric muscle; stylohyoid,
Cranial Nerve VII - Facial Nerve The facial nerve has 3 main components with distinct functions Somatic motor efferent Supplies the muscles of facial expression; posterior belly of digastric muscle; stylohyoid,
By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi
 By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi OBJECTIVES By the end of the lecture, students shouldbe able to: List the nuclei of the deep origin of the trigeminal and facial nerves in the brain
By : Prof Saeed Abuel Makarem & Dr.Sanaa Alshaarawi OBJECTIVES By the end of the lecture, students shouldbe able to: List the nuclei of the deep origin of the trigeminal and facial nerves in the brain
CHAPTER 3. OTALGIA 1. HISTORY. Professor Bruce Black MD Dr Jane Black PhD
 CHAPTER 3. OTALGIA Pain felt in the ear is a common problem, but not all earache originates in the ear. Pain can arise from structures near the ear, or alternatively from sites more distant in the head
CHAPTER 3. OTALGIA Pain felt in the ear is a common problem, but not all earache originates in the ear. Pain can arise from structures near the ear, or alternatively from sites more distant in the head
Unit VIII Problem 9 Anatomy of The Ear
 Unit VIII Problem 9 Anatomy of The Ear - The ear is an organ with 2 functions: Hearing. Maintenance of equilibrium/balance. - The ear is divided into 3 parts: External ear. Middle ear (which is also known
Unit VIII Problem 9 Anatomy of The Ear - The ear is an organ with 2 functions: Hearing. Maintenance of equilibrium/balance. - The ear is divided into 3 parts: External ear. Middle ear (which is also known
CHAPTER 13. FACIAL NERVE PARALYSIS
 CHAPTER 13. FACIAL NERVE PARALYSIS Introduction Facial nerve paralysis, whilst not a disease of the ear itself, commonly arises within the ear due to its anatomical course, and often as a result of ear
CHAPTER 13. FACIAL NERVE PARALYSIS Introduction Facial nerve paralysis, whilst not a disease of the ear itself, commonly arises within the ear due to its anatomical course, and often as a result of ear
Laith Sorour. Facial nerve (vii):
:") Laith Sorour Cranial nerves 7 & 8 Hello, there are edited slides please go back to them to see pictures, they are not that much important in this lecture but still, and yes slides are included :p Let s
Laith Sorour Cranial nerves 7 & 8 Hello, there are edited slides please go back to them to see pictures, they are not that much important in this lecture but still, and yes slides are included :p Let s
Parotid Gland, Temporomandibular Joint and Infratemporal Fossa
 M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
M1 - Anatomy Parotid Gland, Temporomandibular Joint and Infratemporal Fossa Jeff Dupree Sanger 9-057 jldupree@vcu.edu Parotid gland: wraps around the mandible positioned between the mandible and the sphenoid
Gross Anatomy of the. TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR
 Gross Anatomy of the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Professor of Anatomy and Neurobiology Assignment: Head
Gross Anatomy of the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Professor of Anatomy and Neurobiology Assignment: Head
Dr.Ban I.S. head & neck anatomy 2 nd y. جامعة تكريت كلية طب االسنان املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102
 جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102 Parotid region The part of the face in front of the ear and below the zygomatic arch is the parotid region. The
جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102/6102 Parotid region The part of the face in front of the ear and below the zygomatic arch is the parotid region. The
For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER
 GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
GROSS ANATOMY EXAMINATION May 15, 2000 For the following questions, indicate the letter that corresponds to the SINGLE MOST APPROPRIATE ANSWER 1. Pain associated with an infection limited to the middle
ASSESSMENT AND TREATMENT OF FACIAL PALSY. Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan
 ASSESSMENT AND TREATMENT OF FACIAL PALSY Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan FACIAL PARALYSIS - ETIOLOGY Bells Palsy Ramsay Hunt Syndrome Infection (Acute/Chronic)
ASSESSMENT AND TREATMENT OF FACIAL PALSY Michael J. LaRouere, M.D. Michigan Ear Institute Farmington Hills, Michigan FACIAL PARALYSIS - ETIOLOGY Bells Palsy Ramsay Hunt Syndrome Infection (Acute/Chronic)
Lec [8]: Mandibular nerve:
![Lec [8]: Mandibular nerve:](/thumbs/94/121295776.jpg "Lec [8]: Mandibular nerve:") Lec [8]: Mandibular nerve: The mandibular branch from the trigeminal ganglion lies in the middle cranial fossa lateral to the cavernous sinus. With the motor root of the trigeminal nerve [motor roots lies
Lec [8]: Mandibular nerve: The mandibular branch from the trigeminal ganglion lies in the middle cranial fossa lateral to the cavernous sinus. With the motor root of the trigeminal nerve [motor roots lies
Neoplasms that present as a swelling in the neck may be either
 Problems in otolaryngology Inflammatory swellings Viral and bacterial infection are frequent causes of swellings in the neck. Enlargement of the cervical lymph nodes is most likely but a dormant branchial
Problems in otolaryngology Inflammatory swellings Viral and bacterial infection are frequent causes of swellings in the neck. Enlargement of the cervical lymph nodes is most likely but a dormant branchial
Gross Anatomy of the. TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR. Assignment: Head to Toe Temporomandibular Joint (TMJ)
") Gross Anatomy the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Pressor Anatomy and Neurobiology Assignment: Head to Toe
Gross Anatomy the TEMPORAL BONE, EXTERNAL EAR, and MIDDLE EAR M1 Gross and Developmental Anatomy 9:00 AM, December 11, 2008 Dr. Milton M. Sholley Pressor Anatomy and Neurobiology Assignment: Head to Toe
3-Deep fascia: is absent (except over the parotid gland & buccopharngeal fascia covering the buccinator muscle)
") The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
The Face 1-Skin of the Face The skin of the face is: Elastic Vascular (bleed profusely however heal rapidly) Rich in sweat and sebaceous glands (can cause acne in adults) It is connected to the underlying
Imaging of facial paralysis
 Imaging of facial paralysis Poster No.: C-2151 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Martinez Molina, L. Aleman Romero, L. A. Sanchez Alonso, A. Puerta Sales, V. Garcia Medina; Murcia/ES
Imaging of facial paralysis Poster No.: C-2151 Congress: ECR 2013 Type: Educational Exhibit Authors: N. Martinez Molina, L. Aleman Romero, L. A. Sanchez Alonso, A. Puerta Sales, V. Garcia Medina; Murcia/ES
Cranial Nerve VII & VIII
 Cranial Nerve VII & VIII Lecture Objectives Follow up the course of facial nerve from its point of central connections, exit and down to its target areas. Follow up the central connections of the facial
Cranial Nerve VII & VIII Lecture Objectives Follow up the course of facial nerve from its point of central connections, exit and down to its target areas. Follow up the central connections of the facial
The Seventh Cranial Nerve The Facial By Prof. Dr. Muhammad Imran Qureshi
 The Seventh Cranial Nerve The Facial By Prof. Dr. Muhammad Imran Qureshi Functional Components: SVE: Fibers originate from nucleus of facial nerve, and supply facial muscles GVE: Fibers derived from superior
The Seventh Cranial Nerve The Facial By Prof. Dr. Muhammad Imran Qureshi Functional Components: SVE: Fibers originate from nucleus of facial nerve, and supply facial muscles GVE: Fibers derived from superior
Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus
 Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
Outline of content Temporal fossa Infratemporal fossa Pterygopalatine fossa Terminal branches of external carotid artery Pterygoid venous plexus Boundary Content Communication Mandibular division of trigeminal
The Ear. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
The Ear Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology The Ear The ear consists of the external ear; the middle ear (tympanic cavity); and the internal ear (labyrinth), which contains
Major Anatomic Components of the Orbit
 Major Anatomic Components of the Orbit 1. Osseous Framework 2. Globe 3. Optic nerve and sheath 4. Extraocular muscles Bony Orbit Seven Bones Frontal bone Zygomatic bone Maxillary bone Ethmoid bone Sphenoid
Major Anatomic Components of the Orbit 1. Osseous Framework 2. Globe 3. Optic nerve and sheath 4. Extraocular muscles Bony Orbit Seven Bones Frontal bone Zygomatic bone Maxillary bone Ethmoid bone Sphenoid
K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 10: Facial Nerve Paralysis. Evaluation
 Chapter 10: Facial Nerve Paralysis. Evaluation") K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 10: Facial Nerve Paralysis Evaluation Evaluation of patients with facial nerve paralysis must be a careful process including
K. J. Lee: Essential Otolaryngology and Head and Neck Surgery (IIIrd Ed) Chapter 10: Facial Nerve Paralysis Evaluation Evaluation of patients with facial nerve paralysis must be a careful process including
Infratemporal fossa: Tikrit University college of Dentistry Dr.Ban I.S. head & neck Anatomy 2 nd y.
 Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
Infratemporal fossa: This is a space lying beneath the base of the skull between the lateral wall of the pharynx and the ramus of the mandible. It is also referred to as the parapharyngeal or lateral pharyngeal
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES
 INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
INTRODUCTION: ANATOMY UNDERLYING CLINICAL TESTS OF CRANIAL NERVES CRANIAL NERVE I - OLFACTORY I - OLFACTORY NERVE - SMELL TEST: SMELL ODORS (note: not ammonia; pain in nasal cavity CN5 DAMAGE: LOSS OF
Cranial nerves.
 Cranial nerves eaglezhyxzy@163.com Key Points of Learning Name Components Passing through Peripheral distribution Central connection Function Cranial nerves Ⅰ olfactory Ⅱ optic Ⅲ occulomotor Ⅳ trochlear
Cranial nerves eaglezhyxzy@163.com Key Points of Learning Name Components Passing through Peripheral distribution Central connection Function Cranial nerves Ⅰ olfactory Ⅱ optic Ⅲ occulomotor Ⅳ trochlear
REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM
 REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM - 2017 PALPATE CAROTID ARTERY: AT LEVEL OF CAROTID BIFURCATION VERTEBRAL LEVEL C4 Sternocleidomastoid Muscle INTERNAL CAROTID EXTERNAL CAROTID COMMON
REVIEW/PREVIEW OF HEAD AND NECK ANATOMY FOR ENT EXAM - 2017 PALPATE CAROTID ARTERY: AT LEVEL OF CAROTID BIFURCATION VERTEBRAL LEVEL C4 Sternocleidomastoid Muscle INTERNAL CAROTID EXTERNAL CAROTID COMMON
The Temporal Bone Anatomy & Pathology
 Department of Radiology University of California San Diego The Temporal Bone Anatomy & Pathology John R. Hesselink, M.D. Temporal Bone Axial View Temporal Bone Coronal View Longitudinal Fracture The Temporal
Department of Radiology University of California San Diego The Temporal Bone Anatomy & Pathology John R. Hesselink, M.D. Temporal Bone Axial View Temporal Bone Coronal View Longitudinal Fracture The Temporal
Veins of the Face and the Neck
 Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
Veins of the Face and the Neck Facial Vein The facial vein is formed at the medial angle of the eye by the union of the supraorbital and supratrochlear veins. connected through the ophthalmic veins with
BLOCK 12 Viruses of the ENT
 BLOCK 12 Viruses of the ENT Acute infections Introduction Pharyngitis, Common cold, Sinusitis, Otitis media Recurrent infections Herpes zoster oticus Chronic infections HIV and ENT manifestations Neoplasms
BLOCK 12 Viruses of the ENT Acute infections Introduction Pharyngitis, Common cold, Sinusitis, Otitis media Recurrent infections Herpes zoster oticus Chronic infections HIV and ENT manifestations Neoplasms
Case Report Bilateral Facial Paralysis Caused by Bilateral Temporal Bone Fracture: A Case Report and a Literature Review
 Case Reports in Otolaryngology Volume 2015, Article ID 306950, 4 pages http://dx.doi.org/10.1155/2015/306950 Case Report Bilateral Facial Paralysis Caused by Bilateral Temporal Bone Fracture: A Case Report
Case Reports in Otolaryngology Volume 2015, Article ID 306950, 4 pages http://dx.doi.org/10.1155/2015/306950 Case Report Bilateral Facial Paralysis Caused by Bilateral Temporal Bone Fracture: A Case Report
PTERYGOPALATINE FOSSA
 PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
PTERYGOPALATINE FOSSA Outline Anatomical Structure and Boundaries Foramina and Communications with other spaces and cavities Contents Pterygopalatine Ganglion Especial emphasis on certain arteries and
Via Transmastoid Approach. Mitul Chaitan Bhatt. Maharashtra University Miraj India
 ISSN: 2250-0359 Volume 6 Issue 1 2016 Evaluation Of Patients Of Traumatic Facial Palsy Treated By Facial Nerve Decompression Via Transmastoid Approach Mitul Chaitan Bhatt Maharashtra University Miraj India
ISSN: 2250-0359 Volume 6 Issue 1 2016 Evaluation Of Patients Of Traumatic Facial Palsy Treated By Facial Nerve Decompression Via Transmastoid Approach Mitul Chaitan Bhatt Maharashtra University Miraj India
Anatomy and Physiology. Bones, Sutures, Teeth, Processes and Foramina of the Human Skull
 Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
Anatomy and Physiology Chapter 6 DRO Bones, Sutures, Teeth, Processes and Foramina of the Human Skull Name: Period: Bones of the Human Skull Bones of the Cranium: Frontal bone: forms the forehead and the
7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome.
 7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome. 8. Fundamental examination tools of otoneurology. 20. Ménière s syndrome and Ménière s disease. Therapeutic
7. Anatomy and physiology of the vestibular system. Harmonic and disharmonic vestibular syndrome. 8. Fundamental examination tools of otoneurology. 20. Ménière s syndrome and Ménière s disease. Therapeutic
Structure Location Function
 Frontal Bone Cranium forms the forehead and roof of the orbits Occipital Bone Cranium forms posterior and inferior portions of the cranium Temporal Bone Cranium inferior to the parietal bone forms the
Frontal Bone Cranium forms the forehead and roof of the orbits Occipital Bone Cranium forms posterior and inferior portions of the cranium Temporal Bone Cranium inferior to the parietal bone forms the
Ramsay Hunt syndrome a case report and review of literature
 From the SelectedWorks of Balasubramanian Thiagarajan January 1, 2013 Ramsay Hunt syndrome a case report and review of literature Balasubramanian Thiagarajan Available at: https://works.bepress.com/drtbalu/27/
From the SelectedWorks of Balasubramanian Thiagarajan January 1, 2013 Ramsay Hunt syndrome a case report and review of literature Balasubramanian Thiagarajan Available at: https://works.bepress.com/drtbalu/27/
14, 2007 RESIDENT PHYSICIAN:
 TITLE: Bell s Palsy SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: February 14, 2007 RESIDENT PHYSICIAN: Ki-Hong Kevin Ho, MD FACULTY PHYSICIAN: Shawn D. Newlands, MD, PhD, MBA
TITLE: Bell s Palsy SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: February 14, 2007 RESIDENT PHYSICIAN: Ki-Hong Kevin Ho, MD FACULTY PHYSICIAN: Shawn D. Newlands, MD, PhD, MBA
INFECTION OF EXTERNAL EAR. Miguel G. Wagner R1 HUSE 2017
 INFECTION OF EXTERNAL EAR Miguel G. Wagner R1 HUSE 2017 ANATOMY AURICLE + EXTERNAL AUDITORY CANAL (EAC) + EPITELIAL SURFACE TYMPANIC MB Auricle Fibroelastic cartilage (except lobule) + perichondrium +
INFECTION OF EXTERNAL EAR Miguel G. Wagner R1 HUSE 2017 ANATOMY AURICLE + EXTERNAL AUDITORY CANAL (EAC) + EPITELIAL SURFACE TYMPANIC MB Auricle Fibroelastic cartilage (except lobule) + perichondrium +
AUDITORY APPARATUS. Mr. P Mazengenya. Tel 72204
 AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
AUDITORY APPARATUS Mr. P Mazengenya Tel 72204 Describe the anatomical features of the external ear Describe the tympanic membrane (ear drum) Describe the walls of the middle ear Outline the structures
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Anatomy of the ear: Lymphatics
 Anatomy of the ear: 1. External ear which consist of auricle and external auditory canal. The auricle has a framework of cartilage except the lobule, the skin is closely adherent to perichonderium at the
Anatomy of the ear: 1. External ear which consist of auricle and external auditory canal. The auricle has a framework of cartilage except the lobule, the skin is closely adherent to perichonderium at the
Temporal region. temporal & infratemporal fossae. Zhou Hong Ying Dept. of Anatomy
 Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
Temporal region temporal & infratemporal fossae Zhou Hong Ying Dept. of Anatomy Temporal region is divided by zygomatic arch into temporal & infratemporal fossae. Temporal Fossa Infratemporal fossa Temporal
Parotid Gland. Parotid Gland. Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible. Medial pterygoid.
 Ramus of Mandible. Medial pterygoid.") Parotid region Parotid Gland Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible Medial pterygoid Cross section of mandible Masseter D S SCM Parotid Gland Mastoid Process
Parotid region Parotid Gland Largest of 3 paired salivary glands (submandibular; sublingual) Ramus of Mandible Medial pterygoid Cross section of mandible Masseter D S SCM Parotid Gland Mastoid Process
MRI ANATOMY OF THE CRANIAL NERVES. Alexandra Borges Radiology Dpt. Instituto Português de Oncologia de Lisboa
 MRI ANATOMY OF THE CRANIAL NERVES Alexandra Borges Radiology Dpt. Instituto Português de Oncologia de Lisboa SENR 2014 CRANIAL NERVES Olfactory: I Optic: II Oculomotor nerves: III, IV, VI Trigeminal nerve:
MRI ANATOMY OF THE CRANIAL NERVES Alexandra Borges Radiology Dpt. Instituto Português de Oncologia de Lisboa SENR 2014 CRANIAL NERVES Olfactory: I Optic: II Oculomotor nerves: III, IV, VI Trigeminal nerve:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr.
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr. Jalal Almarzooq) - Anatomy of the ear: The ear is divided into 3 parts: External ear.
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Year 6 ENT SMC Otitis Media (Dr. Jalal Almarzooq) - Anatomy of the ear: The ear is divided into 3 parts: External ear.
The Neck the lower margin of the mandible above the suprasternal notch and the upper border of the clavicle
 The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
The Neck is the region of the body that lies between the lower margin of the mandible above and the suprasternal notch and the upper border of the clavicle below Nerves of the neck Cervical Plexus Is formed
Anatomy of External and Middle ear. Dr Sai Manohar
 Anatomy of External and Middle ear. Dr Sai Manohar 1 Human Ear For Anatomical description, Ear is divided into Auricle (or pinna) The external auditory canal The Middle Ear and its derivatives The Inner
Anatomy of External and Middle ear. Dr Sai Manohar 1 Human Ear For Anatomical description, Ear is divided into Auricle (or pinna) The external auditory canal The Middle Ear and its derivatives The Inner
Dr. Sami Zaqout, IUG Medical School
 The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
The skull The skull is composed of several separate bones united at immobile joints called sutures. Exceptions? Frontal bone Occipital bone Vault Cranium Sphenoid bone Zygomatic bones Base Ethmoid bone
1. GOAL 2. OBJECTIVES a) KNOWLEDGE b) SKILLS c) INTEGRATION
 KNOWLEDGE b) SKILLS c) INTEGRATION") 1. GOAL The broad goal of the teaching of undergraduate students in Otorhinolaryngology is that the undergraduate student have acquired adequate knowledge and skills for optimally dealing with common disorders
1. GOAL The broad goal of the teaching of undergraduate students in Otorhinolaryngology is that the undergraduate student have acquired adequate knowledge and skills for optimally dealing with common disorders
VII NERVE PALSY EVALUATION AND MANAGEMENT
 VII NERVE PALSY EVALUATION AND MANAGEMENT The eye cannot close and constantly weeps. The mouth dribbles, the speech is interfered with and mastication impaired. The delicate shades of continence are lost.
VII NERVE PALSY EVALUATION AND MANAGEMENT The eye cannot close and constantly weeps. The mouth dribbles, the speech is interfered with and mastication impaired. The delicate shades of continence are lost.
Bones of the skull & face
 Bones of the skull & face Cranium= brain case or helmet Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction or display. The cranium is composed of eight bones : frontal Occipital
Bones of the skull & face Cranium= brain case or helmet Copyright The McGraw-Hill Companies, Inc. Permission required for reproduction or display. The cranium is composed of eight bones : frontal Occipital
Brainstem and Cranial Nerves II. Nerves covered in other lectures. A reminder about embryology. Prof. Stuart Bunt
 Brainstem and Cranial Nerves II Prof. Stuart Bunt Nerves covered in other lectures 1 Olfactory 2 Optic 3,4,6 Extraocular eye muscles 8 Vestibulo-cochlear 5 Motor and Sensory to the face and muscles of
Brainstem and Cranial Nerves II Prof. Stuart Bunt Nerves covered in other lectures 1 Olfactory 2 Optic 3,4,6 Extraocular eye muscles 8 Vestibulo-cochlear 5 Motor and Sensory to the face and muscles of
HBA THE BODY Head & Neck Written Examination October 23, 2014
 HBA 531 - THE BODY Head & Neck Written Examination October 23, 2014 Name: NOTE 2: When asked to trace nerve, artery, or vein pathways, do so by using arrows, e.g., structure a structure b structure c...
HBA 531 - THE BODY Head & Neck Written Examination October 23, 2014 Name: NOTE 2: When asked to trace nerve, artery, or vein pathways, do so by using arrows, e.g., structure a structure b structure c...
Anatomy of the Ear Region. External ear Middle ear Internal ear
 Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Ear Lecture Objectives Make a list of structures making the external, middle, and internal ear. Discuss the features of the external auditory meatus and tympanic membrane. Describe the shape, position,
Facial nerve, more than any other cranial nerves, Intratemporal Facial Nerve Paralysis- A Three Year Study. Case Series
 Case Series Intratemporal Facial Nerve Paralysis- A Three Year Study Anirban Ghosh, 1 Sankar Prasad Bera, 2 Somnath Saha 3 ABSTRACT Introduction This study on intratemporal facial paralysis is an attempt
Case Series Intratemporal Facial Nerve Paralysis- A Three Year Study Anirban Ghosh, 1 Sankar Prasad Bera, 2 Somnath Saha 3 ABSTRACT Introduction This study on intratemporal facial paralysis is an attempt
Basic Anatomy and Physiology of the Lips and Oral Cavity. Dr. Faghih
 Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
Basic Anatomy and Physiology of the Lips and Oral Cavity Dr. Faghih It is divided into seven specific subsites : 1. Lips 2. dentoalveolar ridges 3. oral tongue 4. retromolar trigone 5. floor of mouth 6.
Mohammad Hisham Al-Mohtaseb. Lina Mansour. Reyad Jabiri. 0 P a g e
 2 Mohammad Hisham Al-Mohtaseb Lina Mansour Reyad Jabiri 0 P a g e This is only correction for the last year sheet according to our record. If you already studied this sheet just read the yellow notes which
2 Mohammad Hisham Al-Mohtaseb Lina Mansour Reyad Jabiri 0 P a g e This is only correction for the last year sheet according to our record. If you already studied this sheet just read the yellow notes which
Face. Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face
 Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Face Definition: The area between the two ears and from the chin to the eye brows. The muscles of the face The muscle of facial expression (include the muscle of the face and the scalp). All are derived
Omran Saeed. Luma Taweel. Mohammad Almohtaseb. 1 P a g e
 2 Omran Saeed Luma Taweel Mohammad Almohtaseb 1 P a g e I didn t include all the photos in this sheet in order to keep it as small as possible so if you need more clarification please refer to slides In
2 Omran Saeed Luma Taweel Mohammad Almohtaseb 1 P a g e I didn t include all the photos in this sheet in order to keep it as small as possible so if you need more clarification please refer to slides In
University of Palestine. Midterm Exam 2013/2014 Total Grade:
 [ Course No: DNTS2208 Course Title: Head and Neck Anatomy Date: 17/11/1024 No. of Questions: (52) Time: 2hours Using Calculator (No) University of Palestine Midterm Exam 2013/2014 Total Grade: Instructor
[ Course No: DNTS2208 Course Title: Head and Neck Anatomy Date: 17/11/1024 No. of Questions: (52) Time: 2hours Using Calculator (No) University of Palestine Midterm Exam 2013/2014 Total Grade: Instructor
Dr.Noor Hashem Mohammad Lecture (5)
") Dr.Noor Hashem Mohammad Lecture (5) 2016-2017 If the mandible is discarded, the anterior part of this aspect of the skull is seen to be formed by the hard palate. The palatal processes of the maxillae
Dr.Noor Hashem Mohammad Lecture (5) 2016-2017 If the mandible is discarded, the anterior part of this aspect of the skull is seen to be formed by the hard palate. The palatal processes of the maxillae
STUDY OF VARIOUS CAUSES OF FACIAL PALSY AND ITS MANAGEMENT PROTOCOL
 STUDY OF VARIOUS CAUSES OF FACIAL PALSY AND ITS MANAGEMENT PROTOCOL S. Venkataramana Rao 1, V. S. Sharma 2, M. V. Subba Rao 3, B. J. Prasad 4, Kalyan 5, Pravin Tez 6, Vijay Kumar 7, G. S. Keerthi 8 1Professor,
STUDY OF VARIOUS CAUSES OF FACIAL PALSY AND ITS MANAGEMENT PROTOCOL S. Venkataramana Rao 1, V. S. Sharma 2, M. V. Subba Rao 3, B. J. Prasad 4, Kalyan 5, Pravin Tez 6, Vijay Kumar 7, G. S. Keerthi 8 1Professor,
C h a p t e r PowerPoint Lecture Slides prepared by Jason LaPres North Harris College Houston, Texas
 C h a p t e r 15 The Nervous System: The Brain and Cranial Nerves PowerPoint Lecture Slides prepared by Jason LaPres North Harris College Houston, Texas Copyright 2009 Pearson Education, Inc., publishing
C h a p t e r 15 The Nervous System: The Brain and Cranial Nerves PowerPoint Lecture Slides prepared by Jason LaPres North Harris College Houston, Texas Copyright 2009 Pearson Education, Inc., publishing
Dr.Ban I.S. head & neck anatomy 2 nd y. جامعة تكريت كلية طب االسنان املرحلة الثانية
 جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102-6102 1 The Palate The palate forms the roof of the mouth and the floor of the nasal cavity. It is divided into two
جامعة تكريت كلية طب االسنان التشريح مادة املرحلة الثانية أ.م.د. بان امساعيل صديق 6102-6102 1 The Palate The palate forms the roof of the mouth and the floor of the nasal cavity. It is divided into two
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Brain and spinal nerve. By: shirin Kashfi
 Brain and spinal nerve By: shirin Kashfi Nervous system: central nervous system (CNS) peripheral nervous system (PNS) Brain (cranial) nerves Spinal nerves Ganglions (dorsal root ganglions, sympathetic
Brain and spinal nerve By: shirin Kashfi Nervous system: central nervous system (CNS) peripheral nervous system (PNS) Brain (cranial) nerves Spinal nerves Ganglions (dorsal root ganglions, sympathetic
General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways
 General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways Lecture Objectives Describe pathways for general sensations (pain, temperature, touch and proprioception) from the face area.
General Sensory Pathways of the Face Area, Taste Pathways and Hearing Pathways Lecture Objectives Describe pathways for general sensations (pain, temperature, touch and proprioception) from the face area.
AXIAL SKELETON SKULL
 AXIAL SKELETON SKULL CRANIAL BONES (8 total flat bones w/ 2 paired) 1. Frontal forms forehead & upper portion of eyesocket (orbital) 2. Parietal paired bones; form superior & lateral walls of cranium 3.
AXIAL SKELETON SKULL CRANIAL BONES (8 total flat bones w/ 2 paired) 1. Frontal forms forehead & upper portion of eyesocket (orbital) 2. Parietal paired bones; form superior & lateral walls of cranium 3.
Cholesteatoma and Non-cholesteatomatous Inflammatory Disease. Cholesteatoma. Disclosures. Overview EAC. Cholesteatoma. None
 Disclosures Cholesteatoma and Non-cholesteatomatous Inflammatory Disease None Amy F Juliano, MD Staff Radiologist, Massachusetts Eye and Ear Infirmary Assistant Professor of Radiology, Harvard Medical
Disclosures Cholesteatoma and Non-cholesteatomatous Inflammatory Disease None Amy F Juliano, MD Staff Radiologist, Massachusetts Eye and Ear Infirmary Assistant Professor of Radiology, Harvard Medical
Trigeminal Nerve Anatomy. Dr. Mohamed Rahil Ali
 Trigeminal Nerve Anatomy Dr. Mohamed Rahil Ali Trigeminal nerve Largest cranial nerve Mixed nerve Small motor root and large sensory root Motor root Nucleus of motor root present in the pons and medulla
Trigeminal Nerve Anatomy Dr. Mohamed Rahil Ali Trigeminal nerve Largest cranial nerve Mixed nerve Small motor root and large sensory root Motor root Nucleus of motor root present in the pons and medulla
Skull-2. Norma Basalis Interna Norma Basalis Externa. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
Skull-2 Norma Basalis Interna Norma Basalis Externa Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Norma basalis interna Base of the skull- superior view The interior of the base of the
Learning Outcomes. The Carotid 20/02/2013. Scalp, Face, Parotid. Layers of the Scalp. The Parotid Gland. The Scalp. The Carotid The Facial Artery
 Learning Outcomes The Scalp Layers of the Scalp Bleeding from the Scalp The Carotid The Facial Artery Major Muscles of the Face and Jaw(s) Muscles of Mastication Muscles of Facial Expression The Parotid
Learning Outcomes The Scalp Layers of the Scalp Bleeding from the Scalp The Carotid The Facial Artery Major Muscles of the Face and Jaw(s) Muscles of Mastication Muscles of Facial Expression The Parotid
Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :
![Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :](/thumbs/88/115294566.jpg "Tikrit University collage of dentistry Dr.Ban I.S. head & neck anatomy 2 nd y. Lec [5] / Temporal fossa :") Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
Lec [5] / Temporal fossa : Borders of the Temporal Fossa: Superior: Superior temporal line. Inferior: gap between zygomatic arch and infratemporal crest of sphenoid bone. Anterior: Frontal process of the
Examination and Diseases of Cranial Nerves
 Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
Cranial nerve evaluation is an important part of a neurologic exam. There are some differences in the assessment of cranial nerves with different species but the general principles are the same. Going
Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery
 Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery Editor: Peter S Roland MD Contributors: Peter S Roland MD, Larry Lundy MD, Jacques Herzog MD, Fred
Facial Paralysis Facial Nerve Subcommittee of the American Academy of Otolaryngology-Head & Neck Surgery Editor: Peter S Roland MD Contributors: Peter S Roland MD, Larry Lundy MD, Jacques Herzog MD, Fred
A Study of Etiopathology and Management of Facial Palsy at a Tertiary Care Institute
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 7 Ver.VII (July 2016), PP 71-75 www.iosrjournals.org A Study of Etiopathology and Management
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 7 Ver.VII (July 2016), PP 71-75 www.iosrjournals.org A Study of Etiopathology and Management
Cranial Nerves VII to XII
 Cranial Nerves VII to XII MSTN121 - Neurophysiology Session 13 Department of Myotherapy Cranial Nerve VIII: Vestibulocochlear Sensory nerve with two distinct branches. Vestibular branch transmits information
Cranial Nerves VII to XII MSTN121 - Neurophysiology Session 13 Department of Myotherapy Cranial Nerve VIII: Vestibulocochlear Sensory nerve with two distinct branches. Vestibular branch transmits information
Introduction to Head and Neck Anatomy
 Introduction to Head and Neck Anatomy Nervous Tissue Controls and integrates all body activities within limits that maintain life Three basic functions 1. sensing changes with sensory receptors 2. interpreting
Introduction to Head and Neck Anatomy Nervous Tissue Controls and integrates all body activities within limits that maintain life Three basic functions 1. sensing changes with sensory receptors 2. interpreting
The Pharynx. Dr. Nabil Khouri MD. MSc, Ph.D
 The Pharynx Dr. Nabil Khouri MD. MSc, Ph.D Introduction The pharynx is the Musculo-fascial halfcylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck Common
The Pharynx Dr. Nabil Khouri MD. MSc, Ph.D Introduction The pharynx is the Musculo-fascial halfcylinder that links the oral and nasal cavities in the head to the larynx and esophagus in the neck Common
Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper. Oral vestibule : is slit like space between.
 Oral cavity Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper Oral vestibule : is slit like space between the teeth, buccal gingiva, lips, and cheeks 1 Oral cavity Oral
Oral cavity Oral cavity : consist of two parts: the oral vestibule and the oral cavity proper Oral vestibule : is slit like space between the teeth, buccal gingiva, lips, and cheeks 1 Oral cavity Oral
Anatomic Relations Summary. Done by: Sohayyla Yasin Dababseh
 Anatomic Relations Summary Done by: Sohayyla Yasin Dababseh Anatomic Relations Lecture 1 Part-1 - The medial wall of the nose is the septum. - The vestibule lies directly inside the nostrils (Nares). -
Anatomic Relations Summary Done by: Sohayyla Yasin Dababseh Anatomic Relations Lecture 1 Part-1 - The medial wall of the nose is the septum. - The vestibule lies directly inside the nostrils (Nares). -
ACUTE PAEDIATRIC EAR PRESENTATIONS PROF IAIN BRUCE PAEDIATRIC OTOLARYNGOLOGIST & ADULT OTOLOGIST
 www.manchesterchildrensent.com ACUTE PAEDIATRIC EAR PRESENTATIONS PROF IAIN BRUCE PAEDIATRIC OTOLARYNGOLOGIST & ADULT OTOLOGIST A CHILD WITH EARACHE UNCOMPLICATED AOM ACUTE OTITIS MEDIA Acute otitis media
www.manchesterchildrensent.com ACUTE PAEDIATRIC EAR PRESENTATIONS PROF IAIN BRUCE PAEDIATRIC OTOLARYNGOLOGIST & ADULT OTOLOGIST A CHILD WITH EARACHE UNCOMPLICATED AOM ACUTE OTITIS MEDIA Acute otitis media
APRIL
 APRIL - 2003 OCTOBER - 2003 February 2009 [KU 652] Sub. Code : 4131 FIRST B.D.S DEGREE EXAMINATION (Modified Regulations III) Paper I HUMAN ANATOMY, HISTOLOGY AND EMBRYOLOGY Time : Three hours
APRIL - 2003 OCTOBER - 2003 February 2009 [KU 652] Sub. Code : 4131 FIRST B.D.S DEGREE EXAMINATION (Modified Regulations III) Paper I HUMAN ANATOMY, HISTOLOGY AND EMBRYOLOGY Time : Three hours
-Ibrahim Al-Naser. -Dr Al- Muhtaseb. 1 P a g e
 -1 -Ibrahim Al-Naser - -Dr Al- Muhtaseb 1 P a g e The Digestive System The doctor started the lecture by talking about the class rules. The GI system is an organ system, it is divided into: The Alimentary
-1 -Ibrahim Al-Naser - -Dr Al- Muhtaseb 1 P a g e The Digestive System The doctor started the lecture by talking about the class rules. The GI system is an organ system, it is divided into: The Alimentary
PERIPHERAL NERVOUS SYSTEM
 CHAPTER 13 PERIPHERAL NERVOUS SYSTEM Functional division of nervous system = afferent info to the CNS ascending spinal cord = efferent info from CNS descending spinal cord somatic skin, muscles visceral
CHAPTER 13 PERIPHERAL NERVOUS SYSTEM Functional division of nervous system = afferent info to the CNS ascending spinal cord = efferent info from CNS descending spinal cord somatic skin, muscles visceral
POST TRAUMATIC FACIAL PARALYSIS - A REVIEW
 POST TRAUMATIC FACIAL PARALYSIS - A REVIEW Pages with reference to book, From 105 To 107 Naresh K. Panda, Y. N. Mehra, S.B.S. Mann, Satish K. Mehta ( Deptt. of Otolaryngology, Postgraduate Institute of
POST TRAUMATIC FACIAL PARALYSIS - A REVIEW Pages with reference to book, From 105 To 107 Naresh K. Panda, Y. N. Mehra, S.B.S. Mann, Satish K. Mehta ( Deptt. of Otolaryngology, Postgraduate Institute of
The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi. E. mail:
 The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Temporal fossa The temporal fossa is a depression on the temporal
The Skull and Temporomandibular joint II Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E. mail: abdulameerh@yahoo.com Temporal fossa The temporal fossa is a depression on the temporal
Nose & Mouth OUTLINE. Nose. - Nasal Cavity & Its Walls. - Paranasal Sinuses. - Neurovascular Structures. Mouth. - Oral Cavity & Its Contents
 Dept. of Human Anatomy, Si Chuan University Zhou hongying eaglezhyxzy@163.com Nose & Mouth OUTLINE Nose - Nasal Cavity & Its Walls - Paranasal Sinuses - Neurovascular Structures Mouth - Oral Cavity & Its
Dept. of Human Anatomy, Si Chuan University Zhou hongying eaglezhyxzy@163.com Nose & Mouth OUTLINE Nose - Nasal Cavity & Its Walls - Paranasal Sinuses - Neurovascular Structures Mouth - Oral Cavity & Its
*in general the blood supply of the nose comes from branches of the internal and external carotid arteries.
 In the previous lecture we talked about the anatomy of the nasal cavity, today we will talk about its blood supply, venous drainage, innervations, and finally about the paranasal sinuses. When we describe
In the previous lecture we talked about the anatomy of the nasal cavity, today we will talk about its blood supply, venous drainage, innervations, and finally about the paranasal sinuses. When we describe
Tracing the Cranial Nerves Osteologically
 CN I II III IV V 1 Supra-orbital ethmoidal nn. Ext. nasal V 2 Tracing the Cranial Nerves Osteologically Nucleus of Origin Olfactory tracts of frontal lobe of cerebrum Optic tracts from optic chiasma and
CN I II III IV V 1 Supra-orbital ethmoidal nn. Ext. nasal V 2 Tracing the Cranial Nerves Osteologically Nucleus of Origin Olfactory tracts of frontal lobe of cerebrum Optic tracts from optic chiasma and
Primary Headache Prevalence % (95% CI) Migraine without aura 9 (7-9) Migraine with aura 6 (5-8)
 Migraine without aura 9 (7-9) Migraine with aura 6 (5-8)") Primary Headache Prevalence % (95% CI) Migraine without aura 9 (7-9) Migraine with aura 6 (5-8) Episodic tension-type headache 66 (62-69) Chronic tension-type headache 3 (2-5) Cluster headache 0.1 (0 1)
Primary Headache Prevalence % (95% CI) Migraine without aura 9 (7-9) Migraine with aura 6 (5-8) Episodic tension-type headache 66 (62-69) Chronic tension-type headache 3 (2-5) Cluster headache 0.1 (0 1)
Evaluation and Management of Bell's Palsy January 2002
 TITLE: Evaluation and Management of Bell s Palsy SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 29, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, MD FACULTY PHYSICIAN: Byron
TITLE: Evaluation and Management of Bell s Palsy SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: January 29, 2002 RESIDENT PHYSICIAN: Russell D. Briggs, MD FACULTY PHYSICIAN: Byron