Quantitative Assessment of Pulmonary Regurgitation by Echocardiography in Patients After Repaired TOF
|
|
|
- Luke Robertson
- 6 years ago
- Views:
Transcription
1 Quantitative Assessment of Pulmonary Regurgitation by Echocardiography in Patients After Repaired TOF 서울대학교어린이병원소아청소년과 권보상

2 W. B. TOF (large VSD, infundibular stenosis) 19 mo, 8.5 kg Indication for surgery: cardiac failure, terminal O2 Sat 25 % -> 94% Ann Surg September; 142(3):
3 Survival of the patients with repaired TOF Chiu S et al. Circ Cardiovasc Qual Outcomes 2012;5:
4

5 D. Tang et al. / Progress in Pediatric Cardiology 30 (2010) 51 62
6 Indications for Pulmonary Valve Replacement Moderate or severe pulmonary regurgitation (regurgitation fraction 25%) Asymptomatic patient with two or more of the following criteria RV end-diastolic volume index >150 ml/m2 or Z-score >4. In patients whose body surface area falls outside published normal data: RV/LV EDV ratio >2 RV ESV index >80 ml/m2 RV EF <47% LV EF <55% Large RVOT aneurysm QRS duration >140 ms Sustained tachyarrhythmia related to right heart volume load Other hemodynamically significant abnormalities: RVOTO, severe branch PS, moderate TR, residual L->R shunt (Qp/Qs 1.5),severe AR, Severe aortic dilatation (diameter 5 cm) MRI > Echo Echo = MRI Geva Journal of Cardiovascular Magnetic Resonance 2011, 13:9
7 Indications for Pulmonary Valve Replacement Moderate or severe pulmonary regurgitation (regurgitation fraction 25%) Symptomatic patients Symptoms and signs attributable to severe RV volume load documented by CMR or alternative imaging modality, fulfilling 1 of the quantitative criteria detailed above. Exercise intolerance not explained by extra-cardiac causes with documentation by exercise testing with metabolic cart ( 70% predicted peak VO2 for age and gender not explained by chronotropic incompetence) Signs and symptoms of heart failure (e.g., dyspnea with mild effort or at rest not explained by extracardiac causes, peripheral edema) Syncope attributable to arrhythmia Geva Journal of Cardiovascular Magnetic Resonance 2011, 13:9
8 Echocardiography in adults with TOF 1. Assessment of physiologic and hemodynamic parameters that influence outcome 1. RV and LV size and function 2. Pulmonary regurgitation and / or stenosis 3. Tricuspid regurgitation 4. (QRS duration >180 ms) 2. Assessment of anatomic criteria of unknown significance on outcomes: RVOT aneurysm, DCRV, aortic dilatation and aortic regurgitation 3. Assessment of suitability of RVOT morphology for transcatheter pulmonary valve implantation. RVOT diameter (< 22 mm), prior repair without a transannular patch Wyman W. Lai, et al.(eds) Echocardiography in pediatric and congenital heart disease from fetus to adult. 2009
9 TR grade Mild Moderate Severe TV Usually normal Normal/ abn Abn/ fail leaflet /poor coaptation RV/RA/IVC size Normal Normal or dilated Usually dilated Jet area-central jets (cm2) < >10 VC width (cm) Not defined Not defined, but <0.7 >0.7 PISA radius >0.9 Jet density and contour CW Hepatic vein flow Soft and parabolic Dense, variable contour Systolic dominance Systolic blunting J Am Soc Echocardiogr 2003;16: Dense, triangular with early peaking Systolic reversal >35% RA area IVC retrograde flow
10 PR grade Mild Moderate Severe Pul valve normal Normal/abn abn RV size normal Normal/ dilated Dilated Jet size by CD Thin (usually <10 mm in length) with narrow origin Jet density and deceleration rate -CW Pulmonary systolic flow compared to systemic flow -PW Soft; slow deceleration Intermediate Dense, variable deceleration Usually large, with a wide origin; maybe brief in duration Dense; steep deceleration, early termination of diastolic flow Slightly increased intermediate Greatly increased J Am Soc Echocardiogr 2003;16:
11 Echocardiographic Assessment of Pulmonary Regurgitation (PR) The ratio of jet width / RV outflow diameter: mild 1/3; moderate 1/3-2/3; and severe 2/3 Ratio of duration of PR/ duration of diastole >0.77 correlates with PR regurgitant fraction > 24.5% by CMR Pressure half time <100 ms correlates with hemodynamically significant PR Presence of diastolic flow reversal in branch pulmonary arteries is associated with hemodynamically significant PR Wyman W. Lai, et al.(eds) Echocardiography in pediatric and congenital heart disease from fetus to adult. 2009
12 Grading PR severity color Doppler Mild : small flame below the pulmonary valve Moderate : jet in the right ventricular outflow tract (RVOT) with retrograde diastolic flow in the pulmonary artery Severe: retrograde diastolic flow in both pulmonary artery branches.
13 Grading PR severity color Doppler Regurgitant jet width (measured at valve level during early diastole) RVOT diameter measured at valve level Regurgitant jet width / RVOT diameter (< 0.3, >0.6) Am Heart J 2004;147:

14 Color flow and CW Doppler J Am Soc Echocardiogr 2003;16:

15 Severity of PR assessed by continuous wave Doppler. Bouzas B et al. Eur Heart J 2005;26:
 to the beginning of the next forward pulmonary flow curve The ratio btw duration of PR and total diastolic time = PR index (Pri) Mild : through diastole Moderate: late")
16 PR severity (CW Doppler) PR duration: from the onset in early diastole to the end of the PR Doppler signal Total diastolic time: measured from the end of forward pul flow (coinciding with the onset of the retrograde PR flow) to the beginning of the next forward pulmonary flow curve The ratio btw duration of PR and total diastolic time = PR index (Pri) Mild : through diastole Moderate: late diastole Severe: mid-diastole or earlier >0.77 : significant PR Am Heart J 2004;147:
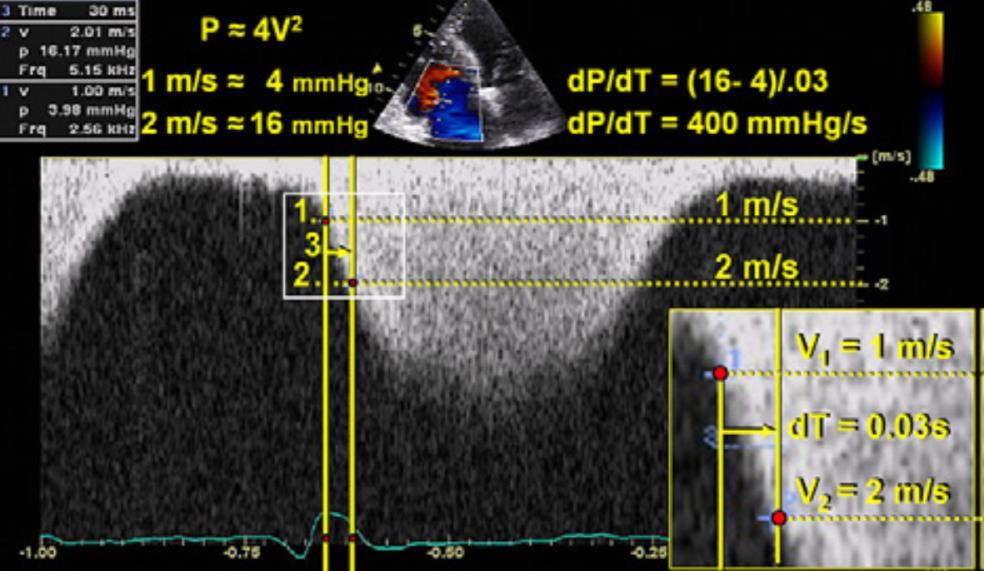
17 PR severity (CW Doppler) PR PRF (MRI) = x PRi (echo) ± 2.55 Am Heart J 2004;147:

18 Pressure half-time / PR Mild PR, PR fraction <20% Significant PR, PR fraction = 40% PHT < 100 ms significant PR J Am Soc Echocardiogr 2003;16:
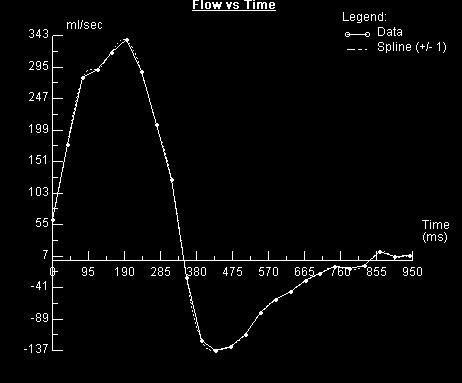
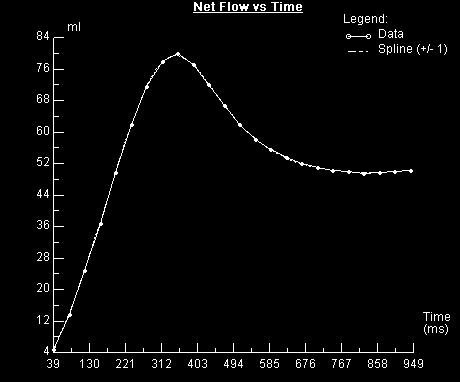
19 Quantifying Pulmonary Regurgitation in repaired TOF DSTVI = x PRF PW in MPA The ratio of diastolic / systolic time velocity integral (DSTVI) Circ Cardiovasc Imaging 2012;5;
20 Determinants of the degree of pulmonary regurgitation (1) Regurgitation orifice area (ROA) (2) RV compliance (3) Diastolic pressure difference between the main pulmonary artery (MPA) and the RV (4) Capacitance of the pulmonary arteries (5) Duration of diastole PR volume = ROA x C x DT x (P2 - P1) 0.5 ROA = regurgitation orifice area; C = constant (empiric number); DT = diastolic time; (P2 - P1) = mean diastolic pressure difference between the MPA and RV AR 가달리 MPA 와 RV 이완기압력차이가작다. (P2-P1) 보다다른인자가중요, 예외적으로 severe PHT 환자에서는 small ROA 에서많은양의 PR 이생김 DT 은 HR 에영향을받음 (other factors: pulmonary vascular resistance, LV function) T. Geva. Journal of Cardiovascular Magnetic Resonance 2011, 13:9


21 1) Regurgitation orifice area (ROA)
22 2) RV compliance Restrictive RV physiology RV size, systolic and diastolic function


23 RV diastolic function VT VT CT ratio =0.49 CT ratio =0.62 Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2006:3-10.

24 Restrictive RV physiology (PR) Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2006:3-10.

25 RV size / volume / function J Am Soc Echocardiogr 2010;23:


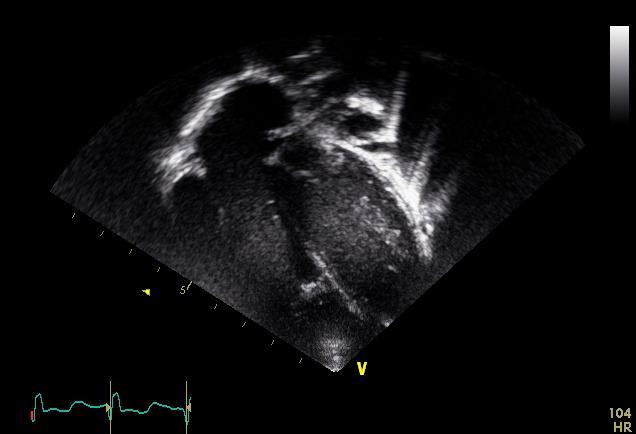
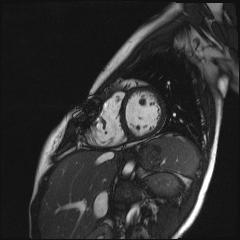
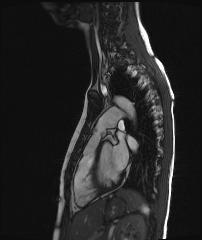
26 Apical 4-chamber view M/ 16 Yr 171 cm, 64 kg RV EDVi 168 ml/m 2 RV EF 44% LV EDVi 76 ml/m 2 F/ 21 yr 168 cm, 47 kg RV EDVi 97 ml/m 2 RV EF 39% LV EDVi 68 ml/m 2
27 RV



28 3D Echo RV volume / EF Statistically significant and clinically meaningful differences in volumetric measurements were observed between the two techniques (MRI vs. Echo). Three dimensional echocardiography does not appear ready for routine clinical use in RV assessment in congenital heart disease patients with more than mild RV dilatation at the current time. Journal of Cardiovascular Magnetic Resonance 2011, 13:78
29 3D Echo in TOF The mean RV ejection fractions were 42 ± 8% on 3D ultrasound and 44 ± 7% on MRI (r = 0.89, P <.0001). The mean end-diastolic volumes were 249 ± 66 and 274 ± 82 ml and the mean end-systolic volumes 147 ± 50 and 159 ± 60 ml on 3D ultrasound and MRI, respectively. JASE 2010 Feb;23(2): Three-dimensional echocardiography underestimated ESV and EDV (P < 0.001) but agreement between 3DE and MRI was excellent (ICC = 0.88 and 0.87, respectively). Ejection fraction was /- 7.8 with 3DE and /- 6.7 with MRI, agreement between both methods was good (ICC = 0.72). Eur J Echocardiogr Aug;10(6): However, the accuracy of 3DE echo diminishes with larger RV volumes, in part due to current difficulty to include the entire RV in the imaged sector.

30 RV volume - indexed RV enddiastolic area (RVEDAi) RVEDAi < 20 cm 2 /m 2 had 100% specificity to predict indexed RV volume 170 ml/m 2 JASE 2012;25:518-23

31 Three-dimensional (3D) knowledge-based reconstruction derived from twodimensional echocardiographic imaging with magnetic tracking J Am Soc Echocardiogr 2011;24:1191-8

32 2D Echo - based 3D reconstruction J Am Soc Echocardiogr 2011;24:1191-8

33 RV function Fractional area change J Am Soc Echocardiogr 2010;23:



34 3) Diastolic pressure difference between the main pulmonary artery (MPA) and the RV
35 4) Capacitance of the pulmonary arteries



36 5) Duration of diastole 3 개월 2 세 27 세
37 MRI - should we be measuring regurgitant fraction or regurgitant volume? Quantification of PR: two distinct method Phase contrast (PC) analysis of flow through the MPA, retrograde flow Indexed PR volume (ml/m 2 ) and PR fraction Ventricular stroke volume (SV) differential measurements derived from steady-state free-precession cine imaging Indexed PR volume (RVSV LVSV) (ml/m 2 ), PR fraction (RVSV LVSV / RVSV x 100 %) European Heart Journal (2009) 30,
38 European Heart Journal (2009) 30, MRI - should we be measuring regurgitant fraction or regurgitant volume? PR volume and PR fraction are not interchangable. PR volume may be a more accurate reflection of RV preload and may better represent physiologically significant PR as compared with PR fraction.


39 Regurgitant volume? LV SV 58 ml RV SV 115 ml Regurgitant volume ml Regurgitant fraction (115-58)/ 115 x 100%
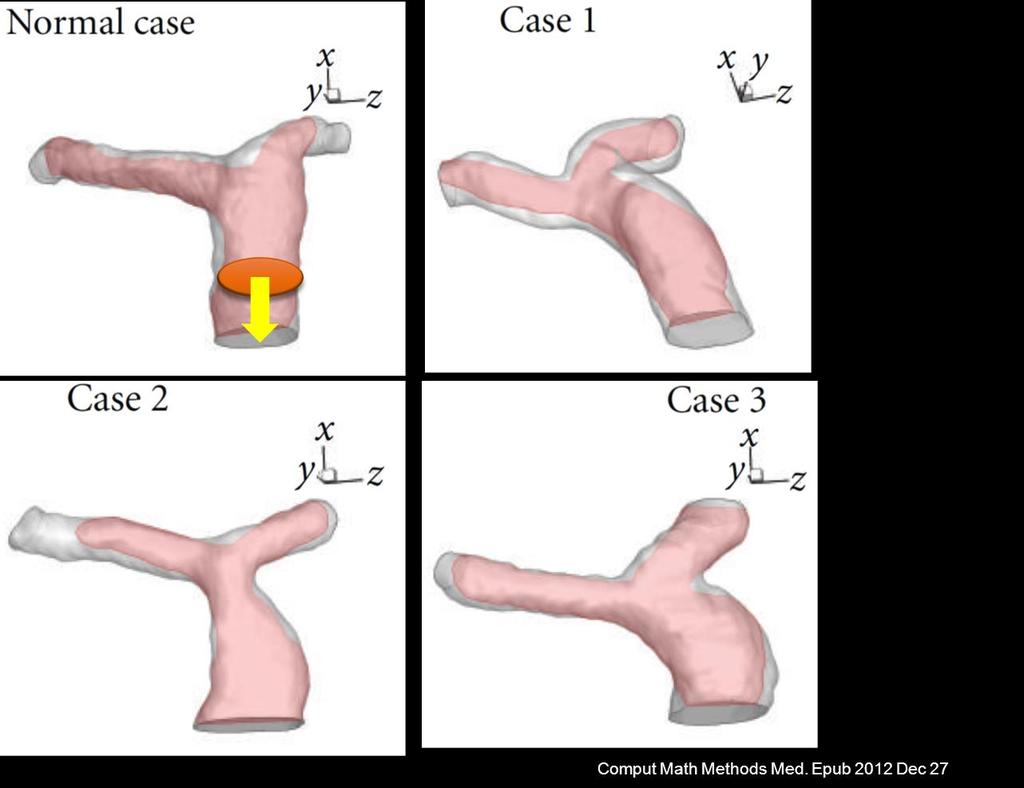
40 Comput Math Methods Med. Epub 2012 Dec 27 Diastolic phase


41 Comput Math Methods Med. Epub 2012 Dec 27 Diastolic phase cross-section




42 PR in RPA and LPA Comput Math Methods Med. Epub 2012 Dec 27


43 Echocardiogram (24 m) Limited by poor acoustic windows; Only qualitative assessment of RV size and function and valve regurgitation
44
45
46 RV FAC (factional area change) Am J Cardiol Mar 15;111(6):


47 Blood flow in pulmonary arteries Comput Math Methods Med. Epub 2012 Dec 27
48 Comput Math Methods Med. Epub 2012 Dec 27 Systolic phase
49 Comput Math Methods Med. Epub 2012 Dec 27 Diastolic phase
50

51 EchoCG RVOT MPA (Late diastolic FF -restrictive ventricular physiology)

52 Pulmonary regurgitation fraction of 34%

53 Doppler examination of pulmonary arterial flow in a patient with restrictive right ventricular physiology. Gatzoulis M A et al. Circulation 1995;91:


54 Transtricuspid Doppler inflow from a restrictive patient demonstrates early passive filling of the right ventricle and apparent filling during atrial systole Transtricuspid Doppler inflow SVC Doppler signal Gatzoulis M A et al. Circulation 1995;91:
55 Immediate postop TOF: hypertrophic RV and low RV compliance, hypoplatic or low-normal PA, low capacitance of RV, relatively high HR (relative short duration of diastole) + relatively large ROA => minimized the impact of PR
56 Geva Journal of Cardiovascular Magnetic Resonance 2011, 13:9 RV remodeling / RV Chamber geometry, myofiber architecture, chamber contraction pattern, coronary artery anatomy and flow dynamic, disposition of the conduction system, and dependency on LV size and function Myocardium: a relatively thin compact layer + a prominent layer of trabeculations interspersed with deep recessess The orientation of the myofibers in the RV is more horizontal and contraction is predominantly from base-to-apex (longitudinal) with a lower degree of angular motion (twist) Supplied by a single coronary artery with nearly 50% of the flow occurring during diastole under normal conditions as oppose to ~90% in the LV. Conduction system in the RV comprises a single fascicle with a long course and a long delay in activation between the base and the distal infundibular free wall, resulting in peristalsis like motion Although RV function impacts LV function, the reverse is much more pronounced with 63% of RV pressure rise accounted for by LV contraction.
57 Indications for Pulmonary Valve Replacement moderate or severe pulmonary regurgitation (regurgitation fraction 25%) Asymptomatic patient with two or more of the following criteria a. RV end-diastolic volume index >150 ml/m2 or Z-score >4. In patients whose body surface area falls outside published normal data: RV/LV EDV ratio >2 b. RV ESV index >80 ml/m2 c. RV EF <47% d. LV EF <55% e. Large RVOT aneurysm f. QRS duration >140 ms g. Sustained tachyarrhythmia related to right heart volume load h. Other hemodynamically significant abnormalities: RVOTO, severe branch PS, moderate TR RVOT obstruction with RV systolic pressure 2/3 systemic Severe branch pulmonary artery stenosis (<30% flow to affected lung) not amenable to transcatheter therapy Moderate tricuspid regurgitation Left-to-right shunt from residual atrial or ventricular septal defects with pulmonary-tosystemic flow ratio 1.5 Severe aortic regurgitation Severe aortic dilatation (diameter 5 cm)
58 Restrictive RV physiology Pulmonary regurgitation: exercise intolerance, RV enlargement, late arrhythmias, and sudden death Restrictive RV physiology: antegrade pulmonary artery flow in late diastole -> seems to protect against RV dilation in pts after repair of TOF Paradoxical effect of restrictive RV physiology in the early postop period and late after repair Circulation. 1996; 94:
59

60 RV pressure-volume relationships IVRT TV opening AV close Isovolemic relaxation MV open AV open Isovolemic contraction MV close


61 The effects of increasing afterload on PR
62 Evaluation of tricuspid regurgitation severity: Utility, advantages, and imitations J Am Soc Echocardiogr 2003;16:
63 Evaluation of PR severity: Utility, advantages, and imitations J Am Soc Echocardiogr 2003;16:
64 Criteria for Pulmonary Valve Replacement Repaired TOF or similar physiology with moderate/severe PR (RF 25% measured by CMR) and two or more of the following criteria: 1. RV EDV index 160 ml/m 2 (Z score>5) 2. RV ESV index 70 ml/m 2 3. LV EDV index 65 ml/m 2 4. RV EF 45% 5. RVOT aneurysm 6. Clinical criteria: exercise intolerance, Sx & signs of HF, cardiac medications, syncope, sustained VT Semin Thorac Cardiovasc Surg Pediatr Card Surg Ann 2006;9:11-22

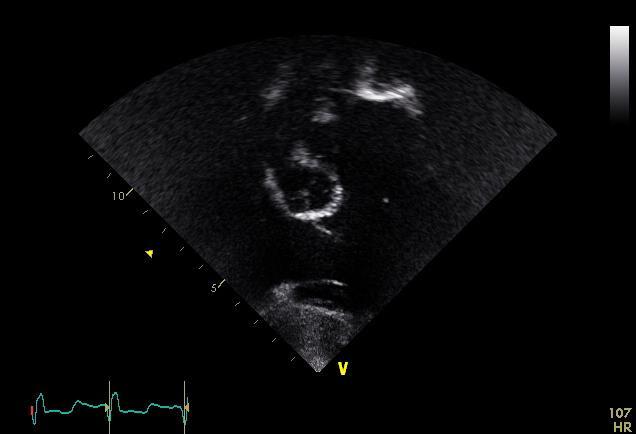
65 Short axis view
66 RVOT view
Cardiac MRI in ACHD What We. ACHD Patients
 Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Cardiac MRI in ACHD What We Have Learned to Apply to ACHD Patients Faris Al Mousily, MBChB, FAAC, FACC Consultant, Pediatric Cardiology, KFSH&RC/Jeddah Adjunct Faculty, Division of Pediatric Cardiology
Pulmonary Regurgitation after TOF Repair. How to Assess and Options of Management? Worakan Promphan, MD.FSCAI.
 Pulmonary Regurgitation after TOF Repair. How to Assess and Options of Management? Worakan Promphan, MD.FSCAI. Queen Sirikit National Institute of Child Health (QSNICH) Bangkok, Thailand How to Assess?
Pulmonary Regurgitation after TOF Repair. How to Assess and Options of Management? Worakan Promphan, MD.FSCAI. Queen Sirikit National Institute of Child Health (QSNICH) Bangkok, Thailand How to Assess?
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT
 FOR REPAIRED TETRALOGY OF FALLOT") MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
MRI (AND CT) FOR REPAIRED TETRALOGY OF FALLOT Linda B Haramati MD, MS Departments of Radiology and Medicine Bronx, New York OUTLINE Pathogenesis Variants Initial surgical treatments Basic MR protocols
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Cardiovascular magnetic resonance for timing pulmonary valve replacement E.Valsangiacomo Buechel University Children s Hospital Zurich Outline Introduction Pulmonary
DECLARATION OF CONFLICT OF INTEREST Cardiovascular magnetic resonance for timing pulmonary valve replacement E.Valsangiacomo Buechel University Children s Hospital Zurich Outline Introduction Pulmonary
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death
 Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Evaluation of the Right Ventricle and Risk Stratification for Sudden Cardiac Death Presenters: Sabrina Phillips, MD FACC FASE Director, Adult Congenital Heart Disease Services The University of Oklahoma
Research Presentation June 23, Nimish Muni Resident Internal Medicine
 Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Research Presentation June 23, 2009 Nimish Muni Resident Internal Medicine Research Question In adult patients with repaired Tetralogy of Fallot, how does Echocardiography compare to MRI in evaluating
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation
 Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children SCAI Fall Fellows Course 2014 Las
Imaging Assessment of the Pulmonary Valve in Stenosis/Atresia and Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children SCAI Fall Fellows Course 2014 Las
CMR for Congenital Heart Disease
 CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
CMR for Congenital Heart Disease * Second-line tool after TTE * Strengths of CMR : tissue characterisation, comprehensive access and coverage, relatively accurate measurements of biventricular function/
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada
 PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
PVR Following Repair of TOF Now? When? Candice Silversides, MD Toronto Congenital Cardiac Centre for Adults University of Toronto Toronto, Canada Late Complications after TOF repair Repair will be necessary
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY
 가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
가천의대길병원소아심장과최덕영 PA C IVS THE EVALUATION AND PRINCIPLES OF TREATMENT STRATEGY PA c IVS (not only pulmonary valve disease) Edwards JE. Pathologic Alteration of the right heart. In: Konstam MA, Isner M, eds.
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
Debate in CHD - When Should We
 Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
Debate in CHD - When Should We Replace Pulmonary Valve? Lee, Jae Young Dept. of Pediatrics, Seoul Saint Mary s Hospital The Catholic University of Korea 14 yr/m, TOF repair (1yr) FC I PR Fraction - 48
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
RIGHT VENTRICULAR SIZE AND FUNCTION
 RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Imaging of Repaired Tetralogy of Fallot in Adults
 SURGICAL MORPHOLOGY and IMAGING of CONGENITAL HEART DISEASE WORKSHOP 22 nd SEPTEMBER, 2016 Imaging of Repaired Tetralogy of Fallot in Adults Tan Ju-Le MBBS, MRCP, FAMS, FACC, FESC Director, Senior Consultant
SURGICAL MORPHOLOGY and IMAGING of CONGENITAL HEART DISEASE WORKSHOP 22 nd SEPTEMBER, 2016 Imaging of Repaired Tetralogy of Fallot in Adults Tan Ju-Le MBBS, MRCP, FAMS, FACC, FESC Director, Senior Consultant
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
Surgical Management of TOF in Adults. Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital
 Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Surgical Management of TOF in Adults Dr Flora Tsang Associate Consultant Department of Cardiothoracic Surgery Queen Mary Hospital Tetralogy of Fallot (TOF) in Adults Most common cyanotic congenital heart
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve
 Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Tetralogy of Fallot Latest data in risk stratification and replacement of pulmonic valve Alexandra A Frogoudaki Adult Congenital Heart Clinic Second Cardiology Department ATTIKON University Hospital No
Quantitation of right ventricular dimensions and function
 SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences
 S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
S. Bruce Greenberg, MD FNASCI and President, NASCI Professor of Radiology and Pediatrics University of Arkansas for Medical Sciences No financial disclosures Aorta Congenital aortic stenosis/insufficiency
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Pulmonary valve: Imaging assessment
 Pulmonary valve: Imaging assessment Fraisse Royal Brompton and Harefield Hospital London, U.K. Consultant and Proctor for medtronic Potential consequences of pulmonary valve Dysfunction RV obstruction
Pulmonary valve: Imaging assessment Fraisse Royal Brompton and Harefield Hospital London, U.K. Consultant and Proctor for medtronic Potential consequences of pulmonary valve Dysfunction RV obstruction
Complex Congenital Heart Disease in Adults
 Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
Complex Congenital Heart Disease in Adults Linda B. Haramati, MD Disclosures Complex Congenital Heart Disease in Adults Linda B. Haramati MD, MS Jeffrey M. Levsky MD, PhD Meir Scheinfeld MD, PhD Department
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
Pulmonary Valve Replacement
 Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
Pulmonary Valve Replacement Christian Kreutzer MD Hospital Nacional Alejandro Posadas Hospital Universitario Austral (No disclosures) Scope of the problem. CHD with PS or PA require a RVOT procedure. Tetralogy
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
COMPLEX CONGENITAL HEART DISEASE: WHEN IS IT TOO LATE TO INTERVENE?
 COMPLEX CONGENITAL HEART DISEASE: WHEN IS IT TOO LATE TO INTERVENE? Aurora S. Gamponia, MD, FPPS, FPCC, FPSE OBJECTIVES Identify complex congenital heart disease at high risk or too late for intervention
COMPLEX CONGENITAL HEART DISEASE: WHEN IS IT TOO LATE TO INTERVENE? Aurora S. Gamponia, MD, FPPS, FPCC, FPSE OBJECTIVES Identify complex congenital heart disease at high risk or too late for intervention
The Fontan circulation. Folkert Meijboom
 The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The Fontan circulation Folkert Meijboom What to expect? Why a Fontan-circulation Indications How does it work Types of Fontan circulation Historical overview Role of echocardiography What to expect? Why
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
New 3D Quantification of Mitral Regurgitation Severity. Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA
 New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη
 Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου 2018 Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη RV shape Triangular shape in frontal plane crescent shape in
Ιπποκράτειες μέρες καρδιολογίας Θεσσαλονίκη, 9-10 Μαρτίου 2018 Φωτεινή Α. Λαζαρίδου Επιμελήτρια Α Γενικό Νοσοκομείο Αγιος Παύλος, Θεσσαλονίκη RV shape Triangular shape in frontal plane crescent shape in
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Echocardiographic assessment of the right ventricle in paediatric pulmonary hypertension.
 Echocardiographic assessment of the right ventricle in paediatric pulmonary hypertension. Mark K. Friedberg, MD No disclosures Outline RV response to increased afterload Echo assessment of RV function
Echocardiographic assessment of the right ventricle in paediatric pulmonary hypertension. Mark K. Friedberg, MD No disclosures Outline RV response to increased afterload Echo assessment of RV function
For Personal Use. Copyright HMP 2013
 12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
12-00415 Case Report J INVASIVE CARDIOL 2013;25(4):E69-E71 A Concert in the Heart. Bilateral Melody Valve Implantation in the Branch Pulmonary Arteries Nicola Maschietto, MD, PhD and Ornella Milanesi,
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation
 First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
First Trimester Fetal Echocardiography: Insight Into the Fetal Circulation Lisa K. Hornberger, MD Fetal & Neonatal Cardiology Program Department of Pediatrics, Division of Cardiology Department of Obstetrics
The need for right ventricular outflow tract reconstruction
 Polytetrafluoroethylene Bicuspid Pulmonary Valve Implantation James A. Quintessenza, MD The need for right ventricular outflow tract reconstruction and pulmonary valve replacement is increasing for many
Polytetrafluoroethylene Bicuspid Pulmonary Valve Implantation James A. Quintessenza, MD The need for right ventricular outflow tract reconstruction and pulmonary valve replacement is increasing for many
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Echocardiographie de la Tétralogie de Fallot opérée
 Echocardiographie de la Tétralogie de Fallot opérée Diala Khraiche M3C-Necker Enfants malades, Université Paris Descartes Paris, France. Disclosure Statement of Financial Interest I currently have, or
Echocardiographie de la Tétralogie de Fallot opérée Diala Khraiche M3C-Necker Enfants malades, Université Paris Descartes Paris, France. Disclosure Statement of Financial Interest I currently have, or
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)
of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on)") Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Evalua&on)of)Le-)Ventricular)Diastolic) Dysfunc&on)by)Echocardiography:) Role)of)Ejec&on)Frac&on) N.Koutsogiannis) Department)of)Cardiology) University)Hospital)of)Patras)! I have no conflicts of interest
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Conflict of Interests
 The Left Ventricle: How Should We Quantify Its Size and Function; Is It Time for 3D in Everyone? Roberto M Lang, MD Conflict of Interests Philips Medical Imaging Research Grants Speakers bureau Advisory
The Left Ventricle: How Should We Quantify Its Size and Function; Is It Time for 3D in Everyone? Roberto M Lang, MD Conflict of Interests Philips Medical Imaging Research Grants Speakers bureau Advisory
What is Ebstein Anomaly?
 Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Echocardiograpnhic Evaluation of : Definition, Detection and Determinants of Outcome P. W. O Leary, M.D. Division of Pediatric Cardiology Mayo Clinic No Conflicts to Disclose What is? Failure of the TV
Cardiovascular MRI of Adult Congenital Heart Disease
 Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Cardiovascular MRI of Adult Congenital Heart Disease Anil K. Attili, MD Cardiovascular Magnetic Resonance imaging of Adult Congenital Heart Disease Anil Attili, M.D. Assistant Professor of Radiology /Cardiology
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών Σ.Ράμμος
 ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
ΔΜΙΝΑΡΙΟ ΔΠΙΣΗΜΟΝΙΚΩΝ ΔΝΩΔΩΝ ΔΛΛΗΝΙΚΟΤ ΚΟΛΛΔΓΙΟΤ ΚΑΡ ΙΟΛΟΓΙΑ 2-4.10.2015 Δπιζηημονική Ένωζη Δπεμβαηικής Καρδιολογίας Βαλβιδοπάθειες, Γιαδερμικές παρεμβάζεις Διαδερμική θεραπεία των παραβαλβιδικών διαφυγών
2/4/2011. Nathan Kerner, M.D.
 Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
Nathan Kerner, M.D. Definition Elevated pressures - cut off usually >40 mmhg pulmonary artery systolic pressure (PASP) Usually associated with elevated pulmonary vascular resistance (PVR) measured in dynessec/cm
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Little is known about the degree and time course of
 Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
Differential Changes in Regional Right Ventricular Function Before and After a Bilateral Lung Transplantation: An Ultrasonic Strain and Strain Rate Study Virginija Dambrauskaite, MD, Lieven Herbots, MD,
A structured report for assessment of Tetralogy of Fallot by Cardiac MRI according to recent guidelines
 A structured report for assessment of Tetralogy of Fallot by Cardiac MRI according to recent guidelines Poster No.: C-0125 Congress: ECR 2016 Type: Educational Exhibit Authors: N. Stagnaro, G. Trocchio,
A structured report for assessment of Tetralogy of Fallot by Cardiac MRI according to recent guidelines Poster No.: C-0125 Congress: ECR 2016 Type: Educational Exhibit Authors: N. Stagnaro, G. Trocchio,
Institute of Cardiology Warsaw, Poland
 Mateusz Śpiewak, Elżbieta K. Biernacka, Łukasz A. Małek, Jolanta Miśko, Joanna Petryka, Mirosław Kowalski, Barbara Miłosz, Magdalena Żabicka, Piotr Hoffman, Witold Rużyłło Institute of Cardiology Warsaw,
Mateusz Śpiewak, Elżbieta K. Biernacka, Łukasz A. Małek, Jolanta Miśko, Joanna Petryka, Mirosław Kowalski, Barbara Miłosz, Magdalena Żabicka, Piotr Hoffman, Witold Rużyłło Institute of Cardiology Warsaw,
Echo assessment of the failing heart
 Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
Echo assessment of the failing heart Mark K. Friedberg, MD The Labatt Family Heart Center The Hospital for Sick Children Toronto, Ontario, Canada Cardiac function- definitions Cardiovascular function:
ADULT CONGENITAL HEART DISEASE. Stuart Lilley
 ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
ADULT CONGENITAL HEART DISEASE Stuart Lilley More adults than children have congenital heart disease Huge variety of congenital lesions from minor to major Heart failure, re-operation and arrhythmia are
Right Heart Evaluation ASE Guidelines Review. Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC
 Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Ref 1. Ref 2. Ref 3. Ref 4. See graph
 Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
Ref 1 Ref 2 Ref 3 1. Ages 6-23 y/o 2. Significant LVM differences by gender 3. For males 95 th percentiles: a. LVM/BSA = 103 b. LVM/height = 100 4. For females 95 th percentiles: a. LVM/BSA = 84 b. LVM/height
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY
 OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
OPTIMIZING ECHO ACQUISTION FOR STRAIN AND DIASTOLOGY October 8, 2017 Deborah Agler, ACS, RDCS, FASE Coordinator of Education and Training Cleveland Clinic General Principles Diastology Clinical Data Heart
A teenager with tetralogy of fallot becomes a soccer player
 ISSN 1507-6164 DOI: 10.12659/AJCR.889440 Received: 2013.06.06 Accepted: 2013.07.10 Published: 2013.09.23 A teenager with tetralogy of fallot becomes a soccer player Authors Contribution: Study Design A
ISSN 1507-6164 DOI: 10.12659/AJCR.889440 Received: 2013.06.06 Accepted: 2013.07.10 Published: 2013.09.23 A teenager with tetralogy of fallot becomes a soccer player Authors Contribution: Study Design A
Tissue Doppler Imaging in Congenital Heart Disease
 Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Pulmonary Valve Regurgitation
 Pulmonary Valve Regurgitation Ziyad M. Hijazi, MD, FSCAI, FACC James A. Hunter,MD, University Chair Professor Of Pediatrics & Internal Medicine Rush Center For Congenital & Structural Heart Disease Rush
Pulmonary Valve Regurgitation Ziyad M. Hijazi, MD, FSCAI, FACC James A. Hunter,MD, University Chair Professor Of Pediatrics & Internal Medicine Rush Center For Congenital & Structural Heart Disease Rush
Right ventricular adaptation in endurance athletes. António Freitas. No conflict of interest
 The role of echocardiography in sports cardiology Right ventricular adaptation in endurance athletes. António Freitas Cardiology Department - Fernando Fonseca Hospital Lisbon Sports Medicine Centre - Lisbon
The role of echocardiography in sports cardiology Right ventricular adaptation in endurance athletes. António Freitas Cardiology Department - Fernando Fonseca Hospital Lisbon Sports Medicine Centre - Lisbon
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
PULMONARY VENOUS OBSTRUCTION
 Korean Cardiology Society Busan / April 19-20, 2019 PULMONARY VENOUS OBSTRUCTION - Integrated Imaging Approach - Shi-Joon Yoo, MD Department of Diagnostic Imaging and Division of Cardiology, Department
Korean Cardiology Society Busan / April 19-20, 2019 PULMONARY VENOUS OBSTRUCTION - Integrated Imaging Approach - Shi-Joon Yoo, MD Department of Diagnostic Imaging and Division of Cardiology, Department
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
LUST trial. Echocardiography USER S MANUAL
 LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
When should we intervene surgically in pediatric patient with MR?
 When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
When should we intervene surgically in pediatric patient with MR? DR.SAUD A. BAHAIDARAH CONSULTANT, PEDIATRIC CARDIOLOGY ASSISTANT PROFESSOR OF PEDIATRICS HEAD OF CARDIOLOGY AND CARDIAC SURGERY UNIT KAUH
Quantification of MR
 Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
Quantifying Aortic Regurgitation
 Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to