LUST trial. Echocardiography USER S MANUAL
|
|
|
- Abner Nash
- 5 years ago
- Views:
Transcription
1 LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy
2 Parameters required (1)



3 Aortic root Measurement of aortic root diameter at sinuses of Valsava from 2-dimensional parasternal long-axis image. Inner edge-to-inner edge measurement in end-systole is advisable.
4 Left ventricular dimensions Left ventricular M-mode dimensions. M-mode delivers sup It is recommended that LV internal dimensions (LVIDd and LVIDs, respectively) and wall thicknesses be measured at the level of the LV minor axis, approximately at the mitral valve leaflet tips. These linear measurements can be made directly from 2D images or using 2D-targeted M-mode echocardiography.

5 Left ventricular outflow tract Left ventricular outflow tract diameter is measured in the parasternal long-axis view in mid-systole from the white black interface of the septal endocardium to the anterior mitral leaflet, parallel to the aortic valve plane and within cm of the valve orifice.
 in apical 4-chamber")
.")
6 Left ventricular volumes Two-dimensional measurements for volume calculations using biplane method of disks (modified Simpson s rule) in apical 4-chamber (A4C) and apical 2-chamber (A2C) views at end diastole (LV EDD) and at end systole (LV ESD). Papillary muscles should be excluded from the cavity in the tracing.
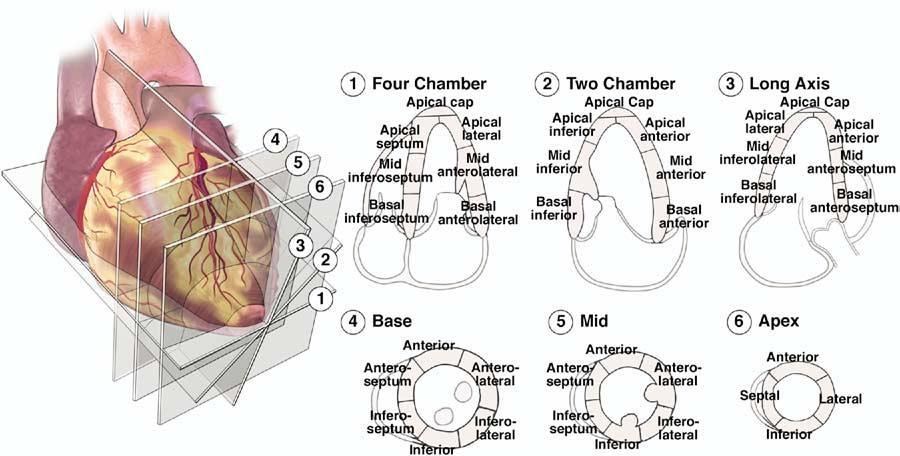
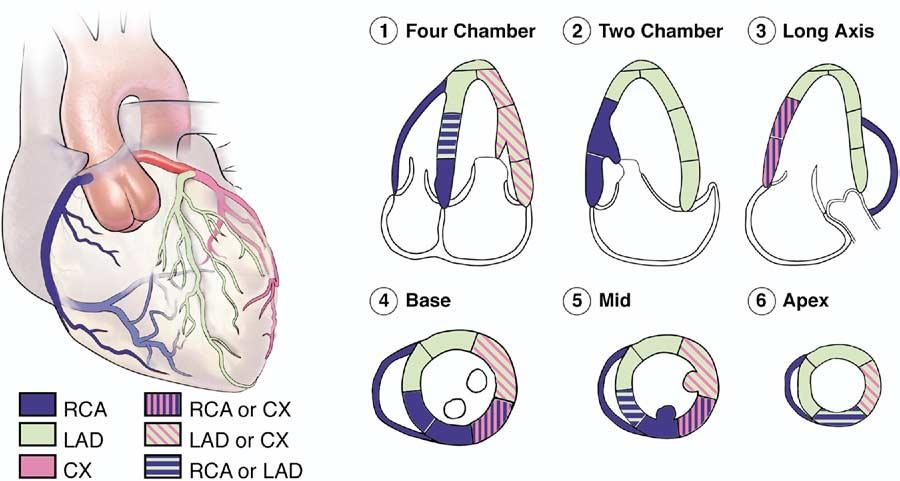
7 LV segmentation for WMSI
 using apical 4-chamber (A4C) and apical 2-chamber (A2C) views at ventricular endsystole (maximum LA")
8 Left atrial volumes Measurement of left atrial (LA) volume from biplane method of disks (modified Simpson s rule) using apical 4-chamber (A4C) and apical 2-chamber (A2C) views at ventricular endsystole (maximum LA size).
9 Aortic peak velocity Aor1c ou<low can be displayed in the apical five- chamber view. The V- shaped flow profile
, with a length (or gate) of 3 5 mm, is positioned on the LV side of the")

10 TVI LVOT Left ventricular outflow tract (LVOT) time-velocity integral is measured from the apical approach (5-chamber). Using pulsed-doppler, the sample volume (SV), with a length (or gate) of 3 5 mm, is positioned on the LV side of the aortic valve, just proximal to the region of flow acceleration into the jet. An optimal signal shows a smooth velocity curve with a narrow velocity range at each time point. The VTI is measured by tracing the modal velocity (middle of the dense signal).

11 Mitral valve inflow Pulsed- wave (PW) Doppler is performed in the apical 4- chamber view to obtain mitral inflow veloci1es to assess LV filling. A 1- mm to 3- mm sample volume is then placed between the mitral leaflet 1ps during diastole to record a crisp velocity profile.


.")
12 Tissue Doppler Imaging of the LV Myocardial velocity recording obtained from apical window with 1ssue Doppler using PW mode. Diagram illustrates Doppler cursor with sample volume posi1oned at base of lateral wall. Recording shows systolic posi1ve wave (S), early diastolic wave (E ), and atrial wave (a ). E should be assessed at both lateral and septal wall. S should also be the mean value of lateral and septal wall measurements.


13 RV basal diameter RV basal diameter corresponds to RVD1
14 Right atrial area Tracing of the right atrium (RA) is performed from the plane of the tricuspid annulus (TA), along the interatrial septum (IAS), superior and anterolateral walls of the RA. The right atrial major dimension is represented by the green line from the TA center to the superior right atrial wall, and the right atrial minor dimension is represented by the blue line from the anterolateral wall to the IAS.

15 TVI RVOT The TVI at RVOT is obtained by placing a 1- to 2-mm pulsed wave Doppler sample volume in the proximal RVOT.
16 TAPSE Measurement of tricuspid annular plane systolic excursion (TAPSE): the monodi- mensional cursor should be oriented to the junc1on of the tricuspid valve plane with the right ventricle free wall, using the 2- dimensional apical 4- chamber view. The tricuspid annular plane systolic excursion is measured as the total excursion of the tricuspid annulus from end- diastole to end- systole.
17 Tissue Doppler Imaging of the RV Tissue Doppler of the tricuspid annulus: a sample is placed on the tricuspid annulus at the place of attachment of the anterior leaflet of the tricuspid valve. Peak systolic (S ), peak early (E ) and late (A ) diastolic annular velocities are recorded.
.")
18 Vena cava diameter The diameter (solid line) is measured perpendicular to the long axis of the IVC at endexpiration, just proximal to the junction of the hepatic veins that lie approximately 0.5 to 3.0 cm proximal to the ostium of the right atrium (RA). M-mode can be used to assess the percentage of diameter variation during inspiration.

19 Tricuspidal peak velocity Spectral continuous-wave Doppler signal of tricuspid regurgitation corresponding to the right ventricular (RV) right atrial (RA) pressure gradient. It is recommended to gather TR signals from several windows and to use the signal with the highest velocity. Technically adequate signals with well-defined borders can be obtained in the majority of patients.
20 Parameters required (2)
 2 x VTI LVOT VTI AV Calcula1on of con1nuity- equa1on valve area requires three measurements: 1) aor1c valve TVI by CW Doppler in 5- chamber apical view; 2) LVOT TVI by PW")
21 Aortic stenosis: continuity equation Aor1c valve area is calculated based on the con1nuity- equa1on, according to the following formula: AVA = Area LVOT x VTI LVOT VTI AV which results in: AVA = x (diameter LVOT ) 2 x VTI LVOT VTI AV Calcula1on of con1nuity- equa1on valve area requires three measurements: 1) aor1c valve TVI by CW Doppler in 5- chamber apical view; 2) LVOT TVI by PW Doppler in 5- chamber apical view; 3) LVOT diameter from parasternal long axis view (zoomed image).
22 Aortic stenosis: grading severity Table 3 Recommendations for classification of AS severity Aortic sclerosis Mild Moderate Severe Aortic jet velocity (m/s) 2.5 m/s Mean gradient (mmhg),20 (,30 a ) b (30 50 a ).40 b (.50 a ) AVA (cm 2 ) ,1.0 Indexed AVA (cm 2 /m 2 ) ,0.6 Velocity ratio ,0.25 a ESC Guidelines. b AHA/ACC Guidelines.
.")
23 Aortic regurgitation: vena contracta a b a b Regurgitant jet. Parasternal long- axis view. The posi1on for measuring the height of the colour flow map as a percentage of the ou<low tract height is at (a). The vena contracta or neck is at (b).


24 Aortic regurgitation: PHT CW Doppler tracing of aor1c regurgita1on velocity illustra1ng method for determining pressure half 1me.
25 Aortic regurgitation: grading severity Table 2 Grading the severity of AR Parameters Mild Moderate Severe... Qualitative Aortic valve morphology Normal/Abnormal Normal/Abnormal Abnormal/flail/large coaptation defect Colour flow AR jet width a Small in central jets Intermediate Large in central jet, variable in eccentric jets CW signal of AR jet Incomplete/faint Dense Dense Diastolic flow reversal in descending aorta Semi-quantitative Brief, protodiastolic flow reversal Intermediate Holodiastolic flow reversal (end-diastolic velocity.20 cm/s) VC width (mm),3 Intermediate.6 Pressure half-time (ms) b.500 Intermediate,200 Quantitative EROA (mm 2 ), ; c 30 R Vol (ml), ; c 60 +LV size d AR, aortic regurgitation; CW, continuous-wave; LA, left atrium; EROA, effective regurgitant orifice area; LV, left ventricle; R Vol, regurgitant volume; VC, vena contracta. a At a Nyquist limit of cm/s. b PHT is shortened with increasing LV diastolic pressure, vasodilator therapy, and in patients with a dilated compliant aorta or lengthened in chronic AR. c Grading of the severity of AR classifies regurgitation as mild, moderate or severe and subclassifies the moderate regurgitation group into mild-to-moderate (EROA of mm or an R Vol of ml) and moderate-to-severe (EROA of mm 2 or an R Vol of ml). d Unless for other reasons, the LV size is usually normal in patients with mild AR. In acute severe AR, the LV size is often normal. In chronic severe AR, the LV is classically dilated. Accepted cut-off values for non-significant LV enlargement: LV end-diastolic diameter,56 mm, LV end-diastolic volume,82 ml/m 2, LV end-systolic diameter,40 mm, LV end-systolic volume,30 ml/m 2.


26 Mitral stenosis: PHT CW Doppler tracing taken from a pa1ent with mitral stenosis, illustra1ng measurement of pressure half 1me. Figure 14 CW Doppler tracing taken from a patient with Determination of Doppler pressure half-time (T1/2) with a bimodal, non-linear decreasing slope of the E-wave. The deceleration slope should not be traced from the early part (left), but using the extrapolation of the linear midportion of the mitral velocity profile (right).
27 Mitral stenosis: mean gradient Doppler gradient is assessed using the apical window in most cases, as it allows for parallel alignment of the ultrasound beam and mitral inflow. The ultrasound Doppler beam should be oriented to minimize the intercept angle with mitral flow to avoid underestimation of velocities. In the figure: determination of mean mitral gradient from Doppler diastolic mitral flow in a patient with severe mitral stenosis in atrial fibrillation. Mean gradient varies according to the length of diastole: it is 8 mmhg during a short diastole (A) and 6 mmhg during a longer diastole (B).
28 Mitral stenosis: valve area Planimetry measurement is obtained by direct tracing of the mitral orifice, including opened commissures, if applicable, on a parasternal short-axis view.
 a,5 5 10.10 Pulmonary artery pressure (mmhg),30 30 50.")
29 Mitral stenosis: grading severity Table 9 severity Recommendations for classification of mitral stenosis Mild Moderate Severe Specific findings Valve area (cm 2 ) ,1.0 Supportive findings Mean gradient (mmhg) a, Pulmonary artery pressure (mmhg), a At heart rates between 60 and 80 bpm and in sinus rhythm.

30 Mitral regurgitation: vena contracta The vena contracta is the area of the jet as it leaves the regurgitant orifice. The vena contracta is typically imaged in a view perpendicular to the commissural line (e.g. the parasternal long-axis or the apical four- chamber view) using a careful probe angulation to optimize the flow image, an adapted Nyquist limit (colour Doppler scale) (40 70 cm/s) to perfectly identify the neck or narrowest portion of the jet and the narrowest Doppler colour sector scan coupled with the zoom mode to improve resolution and measurement accuracy.


31 Mitral regurgitation: PISA method Fig. 24. Proximal isovelocity surface area (PISA).
32 Mitral regurgitation: grading severity Table 3 Grading the severity of organic mitral regurgitation Parameters Mild Moderate Severe... Qualitative MV morphology Normal/Abnormal Normal/Abnormal Flail lefleat/ruptured PMs Colour flow MR jet Small, central Intermediate Very large central jet or eccentric jet adhering, swirling and reaching the posterior wall of the LA Flow convergence zone a No or small Intermediate Large CW signal of MR jet Faint/Parabolic Dense/Parabolic Dense/Triangular Semi-quantitative VC width (mm),3 Intermediate 7 (.8 for biplane) b Pulmonary vein flow Systolic dominance Systolic blunting Systolic flow reversal c Mitral inflow A wave dominant d Variable E wave dominant (.1.5 cm/s) e TVI mit /TVI Ao,1 Intermediate.1.4 Quantitative EROA (mm 2 ), ; f 40 R Vol (ml), ; f 60 + LV and LA size and the systolic pulmonary pressure g CW, continuous-wave; LA, left atrium; EROA, effective regurgitant orifice area; LV, left ventricle; MR, mitral regurgitation; R Vol, regurgitant volume; VC, vena contracta. a At a Nyquist limit of cm/s b For average between apical four- and two-chamber views. c Unless other reasons of systolic blunting (atrial fibrillation, elevated LA pressure). d Usually after 50 years of age; e in the absence of other causes of elevated LA pressure and of mitral stenosis. f Grading of severity of organic MR classifies regurgitation as mild, moderate or severe, and sub-classifies the moderate regurgitation group into mild-to-moderate (EROA of mm or a R Vol of ml) and moderate-to-severe (EROA of mm 2 or a R Vol of ml). g Unless for other reasons, the LA and LV size and the pulmonary pressure are usually normal in patients with mild MR. In acute severe MR, the pulmonary pressures are usually elevated while the LV size is still often normal. In chronic severe MR, the LV is classically dilated. Accepted cut-off values for non significant left-sided chambers enlargement: LA volume,36 ml/m 2, LV end-diastolic diameter,56 mm, LV end-diastolic volume,82 ml/m 2, LV end-systolic diameter,40 mm, LV end-systolic volume,30 ml/m 2, LA diameter,39 mm, LA volume,29 ml/m 2.

33 Tricuspidal stenosis The evaluation of stenosis severity is primarily done using the haemodynamic information provided by CWD. The tricuspid inflow velocity is best recorded from either a low parasternal right ventricular inflow view or from the apical four-chamber view.
34 Tricuspidal regurgitation Figure 29 Semi-quantitative assessment of tricuspid regurgitation severity using the vena contracta width (VC). The three components of the regurgitant jet (flow convergence zone, vena contracta, jet turbulence) are obtained. CV, chamber view.
35 Tricuspidal regurgitation: grading severity Table 5 Grading the severity of TR Parameters Mild Moderate Severe... Qualitative Tricuspid valve morphology Normal/abnormal Normal/abnormal Abnormal/flail/large coaptation defect Colour flow TR jet a Small, central Intermediate Very large central jet or eccentric wall impinging jet CW signal of TR jet Faint/Parabolic Dense/Parabolic Dense/Triangular with early peaking (peak,2 m/s in massive TR) Semi-quantitative VC width (mm) a Not defined,7 7 PISA radius (mm) b Hepatic vein flow c Systolic dominance Systolic blunting Systolic flow reversal Tricuspid inflow Normal Normal E wave dominant ( 1 cm/s) d Quantitative EROA (mm 2 ) Not defined Not defined 40 R Vol (ml) Not defined Not defined 45 + RA/RV/IVC dimension e CW, continuous-wave; EROA, effective regurgitant orifice area; RA, right atrium; RV, right ventricle; R Vol, regurgitant volume; TR, tricuspid regurgitation; VC, vena contracta. a At a Nyquist limit of cm/s. b Baseline Nyquist limit shift of 28 cm/s. c Unless other reasons of systolic blunting (atrial fibrillation, elevated RA pressure). d In the absence of other causes of elevated RA pressure. e Unless for other reasons, the RA and RV size and IVC are usually normal in patients with mild TR. An end-systolic RV eccentricity index.2 is in favour of severe TR. In acute severe TR, the RV size is often normal. In chronic severe TR, the RV is classically dilated. Accepted cut-off values for non significant right-sided chambers enlargement (measurements obtained from the apical four-chamber view): Mid RV dimension 33 mm, RV end-diastolic area 28 cm 2, RV end-systolic area 16 cm 2, RV fractional area change.32%, maximal RA volume 33 ml/m 2. An IVC diameter,1.5 cm is considered normal.
36 Pulmonary stenosis Table 11 Grading of pulmonary stenosis Mild Moderate Severe Peak velocity (m/s), Peak gradient (mmhg), Continuous-wave Doppler is used to assess the severity when even mild stenosis is present. It is important to line up the Doppler sample volume parallel to the flow with the aid of colour flow mapping where appropriate. In adults, this is usually most readily performed from a parasternal short-axis view.
 severity by using colour flow imaging.")
.")
37 Pulmonary regurgitation Figure 15 Assessment of pulmonary regurgitation (PR) severity by using colour flow imaging. (Top) Measurement of the vena contracta width in two patients with PR (left: moderate, right: severe). (Bottom) Continuous-wave Doppler recordings.
38 List of abbrevia-ons LV = lea ventricle WMSI = wall mo1on score index LVOT = lea ventricular ou<low tract TVI = 1me- velocity integral LA = lea atrium E = early mitral diastolic velocity A = late mitral diastolic velocity DT = decelera1on 1me IVRT =isovolumetric relaxa1on 1me TDI = 1ssue Doppler imaging S = myocardial systolic lea ventricular velocity E = early myocardial diastolic velocity A = late myocardial diastolic velocity RV = right ventricle RA = right atrium RVOT = right ventricular ou<low tract TAPSE = tricuspid annular plane systolic excursion IVC = inferior vena cava PHT = pressure half 1me
39 References: - Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardio- graphic assessment of the right heart in adults. J Am Soc Echocardiogr 2010;23: Lang RM, Bierig M, Devereux RB, et al, American Society of 487 Echocardiography's Nomenclature and Standards Committee, Task Force on Chamber Quantification; American College of Cardiology 489 Echocardiography Committee, American Heart Association; 490 European Association of Echocardiography, European Society of 491 Cardiology. Recommendations for chamber quantification. Eur J 492 Echocardiogr 2006;7: Lancellotti P, Moura L, Pierard LA, Agricola E, Popescu BA, Tribouilloy C, Hagendorff A, Monin JL, Badano L, Zamorano JL; European Association of Echocardiography. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease). Eur J Echocardiogr May;11(4): Lancellotti P, Tribouilloy C, Hagendorff A, Moura L, Popescu BA, Agricola E, Monin JL, Pierard LA, Badano L, Zamorano JL; European Association of Echocardiography. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease). Eur J Echocardiogr Apr;11(3): Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quiñones M; EAE/ASE. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echocardiogr Jan;10(1):1-25.
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
How to assess ischaemic MR?
 ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
ESC 2012 How to assess ischaemic MR? Luc A. Pierard, MD, PhD, FESC, FACC Professor of Medicine Head, Department of Cardiology University Hospital Sart Tilman, Liège ESC 2012 No conflict of interest Luc
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Disclosures Rebecca T. Hahn, MD, FASE
 The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The New ASE Guidelines for Native Valvular Regurgitation Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR (With caveats and comments from R. Hahn) William A. Zoghbi MD, FASE, MACC Professor
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
New 3D Quantification of Mitral Regurgitation Severity. Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA
 New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
New 3D Quantification of Mitral Regurgitation Severity Judy Hung, MD Cardiac Ultrasound Laboratory Massachusetts General Hospital Boston, MA No Financial Disclosures No off label discussion of devices
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas
 Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
Marti McCulloch, BS, MBA, RDCS, FASE Houston, Texas Mitral Regurgitation What to Expect Review Specific Signs of Severity Supportive Signs of Severity Qualitative Parameters Structural Doppler Quantitative
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
Adopted by Council March 2006, Revised March 2012, September 2015
 Guidelines, Policies and Statements E4 Education Protocol: Competences Required Of Cardiac Sonographers Who Practice Adult Transthoracic Cardiac Ultrasound Examinations Adopted by Council March 2006, Revised
Guidelines, Policies and Statements E4 Education Protocol: Competences Required Of Cardiac Sonographers Who Practice Adult Transthoracic Cardiac Ultrasound Examinations Adopted by Council March 2006, Revised
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Primary Mitral Regurgitation
 EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
EURO VALVE Madrid News from Valves Guidelines 2012: What s new and Why? Primary Mitral Regurgitation Luc A. Pierard, MD, PhD Professor of Medicine Head of the Department of Cardiology Heart Valve Clinic,
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Prof. JL Zamorano Hospital Universitario Ramón y Cajal
 Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Prof. JL Zamorano Hospital Universitario Ramón y Cajal Should we forget TR? Nath J et al. Impact of tricuspid regurgitation on long-term survival. J Am Coll Cardiol. 2004; 43:405-409 Why is it difficult
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
5 Working With Measurements
 5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
PISA Evaluation of Mitral Regurgitation. Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011
 PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
PISA Evaluation of Mitral Regurgitation Raymond Graber, MD Cardiac Anesthesia Group University Hospitals Case Medical Center 4/07/2011 Introduction Evaluation of MR. What is PISA? Physiologic basis Issues
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
RIGHT VENTRICULAR SIZE AND FUNCTION
 RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Quantifying Aortic Regurgitation
 Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
Quantifying Aortic Regurgitation Linda D. Gillam, MD, MPH Morristown Medical Center Dorothy and Lloyd Huck Chair Cardiovascular Medicine Atlantic Health System No Disclosures 1 Valve Dysfunction Functional
The difficult patient with mitral regurgitation
 Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
Clinical pathways The difficult patient with mitral regurgitation Stress echo can be the best tool Challenging cases Maria João Andrade, Lisbon PT Management of Severe Chronic Organic MR Echo Exercise
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY. MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C.
 AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
AIMI-HF PROCEDURE MANUAL TECHNICAL GUIDE FOR ECHOCARDIOGRAPHY MHI Core Laboratory E. O Meara - J.C. Tardif J. Vincent, G. Grenier, C. Roy February 2016 Montreal Heart Institute HF Research Aude Turgeon,
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
What is a standard transthoracic echocardiogram performed by a cardiologist?
 OFFICIAL COMMUNICATIONS 146 By the Working Group Echocardiography and Cardiac Imaging of the Swiss Society of Cardiology What is a standard transthoracic echocardiogram performed by a cardiologist? Xavier
OFFICIAL COMMUNICATIONS 146 By the Working Group Echocardiography and Cardiac Imaging of the Swiss Society of Cardiology What is a standard transthoracic echocardiogram performed by a cardiologist? Xavier
Diastolic Function: What the Sonographer Needs to Know. Echocardiographic Assessment of Diastolic Function: Basic Concepts 2/8/2012
 Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Diastolic Function: What the Sonographer Needs to Know Pat Bailey, RDCS, FASE Technical Director Beaumont Health System Echocardiographic Assessment of Diastolic Function: Basic Concepts Practical Hints
Introduction RECOMMENDATIONS
 European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
European Journal of Echocardiography (2010) 11, 223 244 doi:10.1093/ejechocard/jeq030 RECOMMENDATIONS European Association of Echocardiography recommendations for the assessment of valvular regurgitation.
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis
 JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
JOINT MEETING 2 Tricuspid club Chairpersons: G. Athanassopoulos, A. Avgeropoulou, M. Khoury, G. Stavridis Similarities and differences in Tricuspid vs. Mitral Valve Anatomy and Imaging. Echo evaluation
Right Heart Evaluation ASE Guidelines Review. Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC
 Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Right Sided Failure Edema Gut congestion
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Back to Basics: Common Errors In Quantitation In Everyday Practice
 Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
Back to Basics: Common Errors In Quantitation In Everyday Practice Deborah Agler, ACS, RDCS, FASE October 9, 2017 ASE: Echo Florida Rebecca T. Hahn, MD Director of Interventional Echocardiography Professor
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Cardiac ultrasound protocols
 Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Revealing new insights. irotate electronic rotation and xplane adjustable biplane imaging. Ultrasound cardiology. irotate and xplane
 Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
Ultrasound cardiology irotate and xplane Revealing new insights irotate electronic rotation and xplane adjustable biplane imaging Annemien van den Bosch and Jackie McGhie Department of Cardiology, Erasmus
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension
 ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
ESC Congress 2011.No 85975 Evaluation of Left Ventricular Diastolic Dysfunction by Doppler and 2D Speckle-tracking Imaging in Patients with Primary Pulmonary Hypertension Second Department of Internal
Recommendations of the European Association of Echocardiography
 European Journal of Echocardiography (2011) 12, 339 353 doi:10.1093/ejechocard/jer051 RECOMMENDATIONS Recommendations of the European Association of Echocardiography How to use echo-doppler in clinical
European Journal of Echocardiography (2011) 12, 339 353 doi:10.1093/ejechocard/jer051 RECOMMENDATIONS Recommendations of the European Association of Echocardiography How to use echo-doppler in clinical
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo
 Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Professors Carpentier and McGoon Mechanism, resulting from the disease Severity of regurgitation, resulting from the mechanism Echo define the mechanism, quantify the regurgitation severity CP1293058-3
Clinical Outcome of Tricuspid Regurgitation. David Messika-Zeitoun
 Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Clinical Outcome of Tricuspid Regurgitation David Messika-Zeitoun I have financial relationships to disclose Consultant for: Edwards, Symetis and Valtech Tricuspid Regurgitation is a Common Finding Tricuspid
Diagnostic approach to heart disease
 Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
Diagnostic approach to heart disease Initial work up History Physical exam Chest radiographs ECG Special studies Echocardiography Cardiac catheterization Echocardiography principles Technique of producing
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD
 CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
CHAPTER 4 AN EFFICACIOUS APPROACH FOR THE QUANTIFICATION OF MITRAL REGURGITATION USING IMAGE PROCESSING AND PROXIMAL FLOW CONVERGENCE METHOD 4.1. Introduction Mitral Regurgitation also called Mitral Insufficiency
B-Mode measurements protocols:
 Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus. Rapid Cardiac Echo (RCE)
 Syllabus. Rapid Cardiac Echo (RCE)") Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
TAVR TTE INTERROGATION BY ALAN MATTHEWS
 TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
TAVR TTE INTERROGATION BY ALAN MATTHEWS KEYS TO ACCURATE ASSESSMENT EDWARDS SAPIEN VALVE 3 PHASES OF TAVR TTE Evaluation (Qualifying) Placement (Intraoperative) Follow-up (Post-Op) GOALS High quality TTE
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
When Does 3D Echo Make A Difference?
 When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
When Does 3D Echo Make A Difference? Wendy Tsang, MD, SM Assistant Professor, University of Toronto Toronto General Hospital, University Health Network 1 Practical Applications of 3D Echocardiography Recommended
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Imaging Guide Echocardiography
 Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Fig.1 Normal appearance of RV in SAX:
 Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Right Heart Hemodynamics: Echo-Cath Discrepancies
 Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Department of cardiac, thoracic and vascular sciences University of Padua, School of Medicine Padua, Italy Right Heart Hemodynamics: Echo-Cath Discrepancies Luigi P. Badano, MD, PhD, FESC, FACC **Dr. Badano
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
NEW GUIDELINES MAJOR ECHOCARDIOGRAPHIC CRITERIA FOR ARVC MINOR ECHOCARDIOGRAPHIC CRITERIA FOR ARVC
 NEW GUIDELINES The Echocardiographic Assessment of the Right Ventricle with particular reference to Arrhythmogenic Right Ventricular Cardiomyopathy A Protocol of the British Society of Echocardiography
NEW GUIDELINES The Echocardiographic Assessment of the Right Ventricle with particular reference to Arrhythmogenic Right Ventricular Cardiomyopathy A Protocol of the British Society of Echocardiography
Quantitation of right ventricular dimensions and function
 SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
SCCS Basics of cardiac assessment Quantitation of right ventricular dimensions and function Tomasz Kukulski, MD PhD Dept of Cardiology, Congenital Heart Disease and Electrotherapy Silesian Medical University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
CASE REPORT: DOUBLE ORIFICE MITRAL VALVE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VALVE IN AN AFRO-CARIBBEAN
 CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
Incorporating the New Echo Guidelines Into Everyday Practice
 Incorporating the New Echo Guidelines Into Everyday Practice Clinical Case RIGHT VENTRICULAR FAILURE Gustavo Restrepo MD President Elect Interamerican Society of Cardiology Director Fellowship Training
Incorporating the New Echo Guidelines Into Everyday Practice Clinical Case RIGHT VENTRICULAR FAILURE Gustavo Restrepo MD President Elect Interamerican Society of Cardiology Director Fellowship Training
Quantification of MR
 Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Valvular Regurgitation: Putting the New Guidelines into Practice James D. Thomas, MD, FACC, FASE, FESC Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
TRANSTHORACIC ECHOCARDIOGRAPHY (TTE) An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015
 An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015") TRANSTHORACIC ECHOCARDIOGRAPHY (TTE) An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015 This piece of work is not meant to teach students echo interpretation, but instead offers
TRANSTHORACIC ECHOCARDIOGRAPHY (TTE) An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015 This piece of work is not meant to teach students echo interpretation, but instead offers
Imaging MV. Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015
 Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Imaging MV Jeroen J. Bax Leiden University Medical Center The Netherlands Davos, feb 2015 MV/MR: information needed on.. 1. MV anatomy 2. MR etiology - primary vs secondary 3. MR severity quantification
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation
 Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
Titel Kardiologie-SG.ch hot topics in heart failure and mitral regurgitation where and how to quantify mitral regurgitation: Echolab, Cathlab or MRI? Philipp K. Haager, St. Gallen Measuring mitral regurgitation?
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Quantification of Cardiac Chamber Size
 2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
2017 KSE 2017-11-25 Quantification of Cardiac Chamber Size Division of Cardiology Keimyung University Dongsan Medical Center In-Cheol Kim M.D., Ph.D. LV size and function Internal linear dimensions PLX
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
What echo measurements are key prior to MitraClip?
 APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
APHP CHU Bichat - Claude Bernard What echo measurements are key prior to MitraClip? Eric Brochet,MD Cardiology Department Hopital Bichat Paris France No disclosure Conflict of interest Case 69 y.o man
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Tissue Doppler Imaging in Congenital Heart Disease
 Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Tissue Doppler Imaging in Congenital Heart Disease L. Youngmin Eun, M.D. Department of Pediatrics, Division of Pediatric Cardiology, Kwandong University College of Medicine The potential advantage of ultrasound
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Swan Song: Echocardiography as a Pulmonary Artery Catheter? Interdepartmental Division of Critical Care Medicine
 Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Swan Song: Echocardiography as a Pulmonary Artery Catheter? The swan is without spot, and it sings sweetly as it dies, that song ending its life Leonardo Da Vinci Curr Opin Anesthesiol 2016, 29:36 45 Circulation.
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
RVOTO adult and post-op
 Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
Right ventricular outflow tract obstruction in the adult: native and post-op Helmut Baumgartner Westfälische Wilhelms-Universität Münster Adult Congenital and Valvular Heart Disease Center University of
ESC/EACTS Guidelines for the Management of Valvular Heart Disease
 ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been
ES/EATS Guidelines for the Management of Valvular Heart Disease European Journal of ardio-thoracic Surgery 2012 - Why do we need new guidelines on the management of valvular disease? New evidence has been