Participate in Board Questions
|
|
|
- Melvin Stewart
- 5 years ago
- Views:
Transcription




1 ASCeXAM / ReASCE Practice Board Exam Questions Sunday Afternoon Mitral Valve Prostheses Aortic Stenosis, Spectrum of Disease, Low Flow, Low Gradient, and Different Variants Aortic Stenosis, Bicuspid Valve, and Aortic Root Dialation Hypertrophic Cardiomyopathy or Phenocopy Systemic Disease Participate in Board Questions Select Afternoon Select SUNDAY SESSION 2 4. VOTE 1. Select Agenda 3a. Ask Questions 3b. Select Practice Board 1
2 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, MD, FASE Case 1 2


3 History A 54 year old woman with hypothyroidism presents to her PCP with worsening of shortness of breath. Systolic and diastolic murmurs are auscultated. Transthoracic echocardiography is requested for further evaluation. 3

4 Q1. Echocardiography confirms the presence of aortic stenosis (orifice area 0.6 cm 2 ) and identifies the presence of moderate aortic regurgitation. Mitral valve thickening is also observed. Which of the following constitutes the most likely etiology for the valvular abnormalities: A. Age related degenerative valve disease B. Rheumatic heart disease C. Annular calcific disease D. Carcinoid heart disease E. Radiation associated valve disease 4
5 Q1. Echocardiography confirms the presence of aortic stenosis (orifice area 0.6 cm 2 ) and identifies the presence of moderate aortic regurgitation. Mitral valve thickening is also observed. Which of the following constitutes the most likely etiology for the valvular abnormalities: A. Age related degenerative valve disease B. Rheumatic heart disease C. Annular calcific disease D. Carcinoid heart disease E. Radiation associated valve disease** Q2. Which of the following conditions would be an expected complication resulting from the disease process causing these left sided valvular abnormalities? A. Flushing B. Constrictive pericarditis C. Coronary artery spasm D. Hypertrophic cardiomyopthy E. Cardioembolic stroke 5
6 Q2. Which of the following conditions would be an expected complication resulting from the disease process causing these left sided valvular abnormalities? A. Flushing B. Constrictive pericarditis** C. Coronary artery spasm D. Hypertrophic cardiomyopthy E. Cardioembolic stroke Radiation Associated Valve Disease Frequent complication Regurgitant lesions > Stenotic lesions Left sided > right sided Risk greater with >30 Gy Women > men Suggestive echocardiographic appearance Calcification and thickening of aortic mitral curtain Anterior changes more profound than posterior (vs MAC) No leaflet doming/commissural involvement (vs RHD) Aortic root calcification increases the likelihood Progressive Periodic screening required 6

7 Radiation Therapy Cardiovascular complications Coronary artery disease Cardiomyopathy Restrictive or dilated Pericardial effusion Constrictive pericarditis Conduction system/arrhythmias Valvular heart disease Carotid artery disease Lancellotti P et al. J Am Soc Echocardiogr 2013;26:
8 Case 2 8
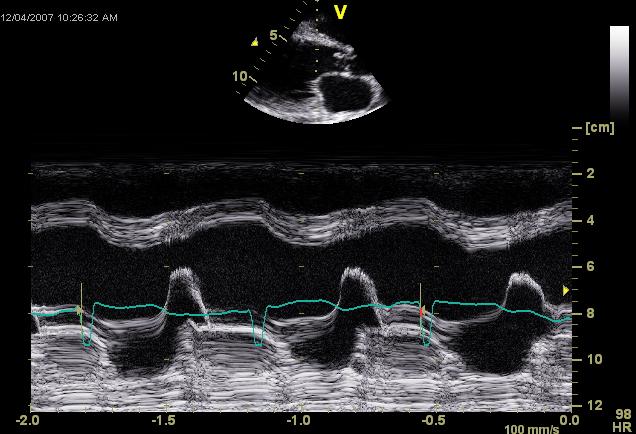
9 Based on this M mode tracing, which of the following findings is unlikely to be present? A. Restrictive mitral inflow pattern B. Soft S1 C. Diastolic mitral regurgitation D. Premature closure of the aortic valve E. Brief diastolic murmur Based on this M mode tracing, which of the following findings is unlikely to be present? A. Restrictive mitral inflow pattern B. Soft S1 C. Diastolic mitral regurgitation D. Premature closure of the aortic valve** E. Brief diastolic murmur 9
10 Choice Explanations D. Premature closure of the aortic valve. This is the correct answer. This M mode tracing displays premature closure of the mitral valve along with high frequency diastolic fluttering of the anterior mitral leaflet (and the interventricular septum). This constellation of findings occurs when acute, severe aortic regurgitation is present. This answer is false because the aortic valve is incompetent. With the rapid rise in LV diastolic pressure characteristic of this lesion, premature opening of the aortic valve may be observed. A. Restrictive mitral inflow pattern. This answer is true due to the rapid increase in LV diastolic pressure characteristic of acute severe AR. B. Soft S1. This answer is true because the rapidly rising LV diastolic pressure leads to premature closure of the mitral valve. C. Diastolic mitral regurgitation. This answer is true. Rapid increases in LV diastolic pressure can lead to transient reversal of the LA LV pressure gradient in diastole and the occurrence of (low velocity) diastolic mitral regurgitation. E. Brief diastolic murmur. This answer is true. The regurgitant murmur is brief in duration because the aortic diastolic pressure rapidly equilibrates with that of the LV. Case 3 10


11 History A 56 year old woman with shortness of breath and the finding of right heart volume overload on outside echocardiography due an ostium secundum ASD is referred for percutaneous closure. RHC revealed PASP 29 mm Hg and PVR <2 WU. Nonobstructive CAD was found. TEE performed at the time of the procedure confirms the presence of the ASD and documents adequate surrounding rims and appropriate PV drainage. However an incidental finding is made. 11
12 Q1. Based on this finding which of the following courses of action should you recommend? A. Inform your interventional colleague to cease the procedure immediately and discuss the finding with the patient and her family. B. Obtain an urgent CT surgery consult. C. Provide additional antibiotic coverage for oral cavity organisms given a high risk of infective endocarditis. D. Continue with the planned procedure and discuss the incidental finding and its implications with the referring cardiologist. Q1. Based on this finding which of the following courses of action should you recommend? A. Inform your interventional colleague to cease the procedure immediately and discuss the finding with the patient and her family. B. Obtain an urgent CT surgery consult. C. Provide additional antibiotic coverage for oral cavity organisms given a high risk of infective endocarditis. D. Continue with the planned procedure and discuss the incidental finding and its implications with the referring cardiologist.** 12
13 Q2. Which of the following statements concerning this valvular abnormality is correct? A. Aortic stenosis is the predominant hemodynamic abnormality. B. Aortic regurgitation is the predominant hemodynamic abnormality. C. Long term survival with this condition is poor. D. Aortic dilatation is not commonly found in association with this lesion. E. Aortic dissection is strongly associated with this valvular abnormality. Q2. Which of the following statements concerning this valvular abnormality is correct? A. Aortic stenosis is the predominant hemodynamic abnormality. B. Aortic regurgitation is the predominant hemodynamic abnormality.** C. Long term survival with this condition is poor. D. Aortic dilatation is not commonly found in association with this lesion. E. Aortic dissection is strongly associated with this valvular abnormality. 13

14 Quadricuspid Aortic Valve Rare congenital abnormality (<0.05% frequency) Recent single center review showed frequency of 0.006% of all echocardiograms Hurwitz and Roberts classification Types A and B most frequent Tsang MYC et al. Circulation 2016;133: Aortic Valve Findings Aortic regurgitation is the predominant hemodynamic abnormality Aortic stenosis present in only 8% 14
15 Associated Findings Aorta Dilatation 29% Usually mild Other cardiac lesions MVP/bowing TVP Pulmonary valve stenosis ASD VSD Coronary anomaly Survival 16% required surgery 15
16 Case 4 History Echo number 25 of a long day. A 22 year old man previously cared for in pediatric cardiology clinics is referred by his new cardiologist for echocardiography to evaluate mitral regurgitation and LV function. He has seen multiple subspecialists over the years. The patient has ESRD and was recently initiated on HD. He has poorly controlled HTN and his CBC/diff is distinctly abnormal. 16



17 17






18 18





19 RV RA grad Pulm vein GLS = 12% LAVI = 39 ml/m2 4 years prior 19
20 Q1. Based on the available data, how would you best characterize his left heart function? A. Normal LVEF, elevated mean LAP, elevated LVeDP B. Normal LVEF, elevated mean LAP, normal LVeDP C. Normal systolic function with normal filling pressures. D. Normal systolic function with elevated filling pressures. Q1. Based on the available data, how would you best characterize his left heart function? A. Normal LVEF, elevated mean LAP, elevated LVeDP** B. Normal LVEF, elevated mean LAP, normal LVeDP C. Normal systolic function with normal filling pressures. D. Normal systolic function with elevated filling pressures. 20
21 Q2. Which of the following conditions is the most likely etiology for the observed echo findings? A. Amyloidosis B. Apical hypertrophic cardiomyopathy C. Hypertensive heart disease D. Hypereosinophilic syndrome E. Rheumatic heart disease Q2. Which of the following conditions is the most likely etiology for the observed echo findings? A. Amyloidosis B. Apical hypertrophic cardiomyopathy C. Hypertensive heart disease D. Hypereosinophilic syndrome** E. Rheumatic heart disease 21

22 BMP Lab Studies Na 139; K 3.7; Cl 100; Co2 29; BUN 15; Cr 6.4; egfr 11. CBC/diff WBC 12.7; Hgb 8.5; Hct PMN 18%; Lymph 13%; Eos 64%; Baso 2%. Hypereosinophilic Syndome Mankad R et al. Heart 2016;102:

23 Gottdiener JS et al. Circulation 1983;67: As recommended by the 2014 AHA/ACC Valvular Heart Disease Guideline, which of the following statements regarding follow up of prosthetic heart valves by echocardiography is true? A. Annual TTE is reasonable staring at 5 years following mechanical valve replacement. B. An initial TEE should be performed routinely to assess valve hemodynamics within 2 months of implantation. C. Change in clinical status should prompt early echocardiography. D. Annual TTE is reasonable staring at 5 years following bioprosthetic valve replacement. 23
24 As recommended by the 2014 AHA/ACC Valvular Heart Disease Guideline, which of the following statements regarding follow up of prosthetic heart valves by echocardiography is true? A. Annual TTE is reasonable staring at 5 years following mechanical valve replacement. B. An initial TEE should be performed routinely to assess valve hemodynamics within 2 months of implantation. C. Change in clinical status should prompt early echocardiography.** D. Annual TTE is reasonable staring at 5 years following bioprosthetic valve replacement. Which of the following statements regarding the obstructed/thrombosed prosthetic heart valve is correct? 1. A PHT > 130 msec is the single best indicator of prosthetic mitral obstruction. 2. Taking into account heart rate is not necessary when assessing trans mitral gradients. 3. Pannus in growth is more common in the aortic position than with mitral PHVs. 4. A peak velocity 2.5 m/sec suggests significant aortic PHV stenosis. 5. Randomized, controlled trials have demonstrated that bolus infusion of rt PA is the fibrinolytic regimen of choice. 24
25 Which of the following statements regarding the obstructed/thrombosed prosthetic heart valve is correct? 1. A PHT > 130 msec is the single best indicator of prosthetic mitral obstruction. 2. Taking into account heart rate is not necessary when assessing trans mitral gradients. 3. Pannus in growth is more common in the aortic position than with mitral PHVs.** 4. A peak velocity 2.5 m/sec suggests significant aortic PHV stenosis. 5. Randomized, controlled trials have demonstrated that bolus infusion of rt PA is the fibrinolytic regimen of choice. Which of the following statements concerning prosthetic heart valve regurgitation is correct? A. Pseudo regurgitation is an issue most often encountered during performance of TEE. B. Any degree of regurgitation indicates dysfunction of a mechanical valve. C. Structural valve deterioration is an uncommon cause of pathological regurgitation. D. Mitral bioprostheses are less prone to suffer structural valve deterioration than are aortic bioprostheses. E. Annular dehiscence most often is a consequence of infective endocarditis. 25
26 Which of the following statements concerning prosthetic heart valve regurgitation is correct? A. Pseudo regurgitation is an issue most often encountered during performance of TEE. B. Any degree of regurgitation indicates dysfunction of a mechanical valve. C. Structural valve deterioration is an uncommon cause of pathological regurgitation. D. Mitral bioprostheses are less prone to suffer structural valve deterioration than are aortic bioprostheses. E. Annular dehiscence most often is a consequence of infective endocarditis.** Aortic Stenosis, Spectrum of Disease, Low Flow, Low Gradient, and Different Variants Martin G. Keane, MD, FASE 26
27 What can lead to underestimation of the aortic valve peak gradient on echo as compared with invasive hemodynamics? 1. Pressure Recovery 2. Equating Peak Instantaneous Gradient To Peak-topeak Gradient 3. A Large Incident Angle To The Aortic Outflow 4. Failure To Account For High Subvalvular Flow 5. Low Stroke Volume What can lead to underestimation of the aortic valve peak gradient on echo as compared with invasive hemodynamics: 1. Pressure Recovery 2. Equating Peak Instantaneous Gradient To Peak-topeak Gradient 3. A Large Incident Angle To The Aortic Outflow 4. Failure To Account For High Subvalvular Flow 5. Low Stroke Volume 27

28 Echo AoV PG vs. Cath/Hemo AoV PG 1. Pressure Recovery Echo PG HIGHER 2. Equating Peak Instantaneous Gradient (Echo) To Peak-to-peak (Hemodynamic) Gradient - Echo PG HIGHER 3. A Large Incident Angle To The Aortic Outflow Echo PG Mis-measured LOWER 4. Failure To Account For High Subvalvular Flow BOTH Echo And Hemo Pg s Elevated 5. Low Stroke Volume BOTH Echo And Hemo Pg s Lower Review Question #2: Reflect upon the image below Transesophageal (TEE): 28
29 Which Of The Following Statements Best Describes This Aortic Valve: 1. Unicuspid - Single Commissure 2. Bicuspid - Fusion Of Left & Right Cor. Cusps 3. Bicuspid - Fusion Of Left & Noncoronary Cusps 4. Functionally Bicuspid Aortic Valve (Trileaflet) 5. Cannot Be Determined Which Of The Following Statements Best Describes This Aortic Valve: 1. Unicuspid - Single Commissure 2. Bicuspid - Fusion Of Left & Right Cor. Cusps 3. Bicuspid - Fusion Of Left & Noncoronary Cusps 4. Functionally Bicuspid Aortic Valve (Trileaflet) 5. Cannot Be Determined 29
30 Short Axis TEE view - AoV N L R A patient presents with the following echo findings: LVOT diameter = 2.0 cm LVOT velocity = 130 cm/s Aortic velocity = 4.1 m/s 2D: Moderately calcified AV, Normal LVEF (70%) The aortic valve area is most likely: 1. Normal 2. Mildly Reduced 3. Moderately Reduced 4. Severely Reduced 5. Cannot Be Calculated (Incongruent Units) 30
 The aortic valve area is most likely: 1. Normal 2. Mildly Reduced DI = 130/410 3. Moderately Reduced DI = 0.32 4.")
31 A patient presents with the following echo findings: LVOT diameter = 2.0 cm LVOT velocity = 130 cm/s Aortic velocity = 4.1 m/s 2D: Moderately calcified AV, Normal LVEF (70%) The aortic valve area is most likely: 1. Normal 2. Mildly Reduced DI = 130/ Moderately Reduced DI = Severely Reduced 5. Cannot Be Calculated (Incongruent Units) 31



32 85 Y/O Woman With H/O Mild Aortic Stenosis Presents With Severe Dyspnea Hypoxic On Room Air, 2+ Pitting Edema 3/6 Mid-late Peaking SEM Radiating To Neck Cardiac Catheterization Ra = 16, Rv = 97/19, Pa 93/27 (53) Pcwp = 22, Co 3.2 L/Min, CI 1.5 L/Min/M 2 Arteriography Minimal Luminal Irregularities 32



33 BSA = 2.14 Sv i = 28 ml 33


34 AVA by CE: 0.8 cm2 Mean gradient <40 mmhg means: 1. This Is Definitely NOT Severe AS 2. The Gradient Is Low Because There Is Depressed LV Ejection Fraction 3. The Gradient Is Low Because The CW Doppler Was Mismeasured 4. The Gradient Is Low Because Of Low Stroke Volume 5. As Long As Calculated AVA Is 0.8 Cm 2, The Mean Gradient Doesn t Matter. 34
35 Mean gradient <40 mmhg means: 1. This Is Definitely NOT Severe AS 2. The Gradient Is Low Because There Is Depressed LV Ejection Fraction 3. The Gradient Is Low Because The CW Doppler Was Mismeasured 4. The Gradient Is Low Because Of Low Stroke Volume 5. As Long As Calculated AVA Is 0.8 Cm 2, The Mean Gradient Doesn t Matter. Low Gradient AS: There s a LOT to think about!! LOW STROKE VOLUME (SV I ) DEPRESSED EF PRESERVED EF TINY VENTRICLE IMPAIRED FILLING SEVERE MR IMPAIRED RV OUTPUT INCREASED VASCULAR AFTERLOAD 35
 all that often. Despite the PVR of 6.3 WU, I firmly believe that this is predominant pulmonary venous hypertension.")

36 Marty There s an opening on the TAVR schedule next Tuesday, and this lady has TAVR written all over. YOU know this is severe AS, I know this is severe AS. MAKE THIS HAPPEN!!! Marty You know that I don t agree with Howard (or anyone) all that often. Despite the PVR of 6.3 WU, I firmly believe that this is predominant pulmonary venous hypertension. Her PHTN will improve post AVR!!! The best next step for diagnosis is 1. No Further Workup Is Needed. 2. Treadmill Stress Testing With Echo Assessment Of AV At Peak Stress. 3. Dobutamine Stress Echocardiography With Staged Assessment Of SV, Ava And Gradients 4. TEE Assessment Of Aortic Valve Morphology And Planimetry 5. Pulmonary Function Testing To Evaluate Lung Disease As An Etiology For Symptoms 36


37 The best next step for diagnosis is 1. No Further Workup Is Needed. 2. Treadmill Stress Testing With Echo Assessment Of AV At Peak Stress. 3. Dobutamine Stress Echocardiography With Staged Assessment Of SV, Ava And Gradients 4. TEE Assessment Of Aortic Valve Morphology And Planimetry 5. Pulmonary Function Testing To Evaluate Lung Disease As An Etiology For Symptoms 37
38 How to Evaluate Aortic Stenosis, Bicuspid Valve, and Aortic Root Dilation Amr E. Abbas, MD, FASE The most common form of bicuspid aortic valve is: 1. Fusion of the LCC/RCC 2. Fusion of the LCC/NCC 3. Fusion of the RCC/NCC 4. Equal distribution of cusp fusion 38
39 The most common form of bicuspid aortic valve is: 1. Fusion of the LCC/RCC 2. Fusion of the LCC/NCC 3. Fusion of the RCC/NCC 4. Equal distribution of cusp fusion The difference between Doppler maximum instantaneous gradient and Catheter peak to peak gradient is due to: 1. Pressure recovery 2. Is due to difference in the timing of the aortic pressure measurement between cath and echo 3. Is due to difference in the timing of the LV pressure measurement between cath and echo 4. Is related to the severity of aortic stenosis 39
40 The difference between Doppler maximum instantaneous gradient and Catheter peak to peak gradient is due to: 1. Pressure recovery 2. Is due to difference in the timing of the aortic pressure measurement between cath and echo 3. Is due to difference in the timing of the LV pressure measurement between cath and echo 4. Is related to the severity of aortic stenosis Discordance between echo and invasive measurements of mean transvalvular gradient is due to : 1. Pressure recovery 2. Eccentric jets 3. Very severe aortic stenosis 4. HOCM 40
41 Discordance between echo and invasive measurements of mean transvalvular gradient is due to : 1. Pressure recovery 2. Eccentric jets 3. Very severe aortic stenosis 4. HOCM Hypertrophic Cardiomyopathy or Phenocopy? Steven J. Lester, MD, FASE 41
.")


42 7. 33 year old male with a history of hypertrophic cardiomyopathy presents with increasing symptoms of shortness of breath (NYHA III). There was no continuous wave Doppler interrogation of the left ventricular outflow tract (LVOT) obtained, however, the peak mitral regurgitation velocity was obtained at 720 cm/sec. The systolic blood pressure was 110mmHg. Assuming a left atrial pressure of 15mmHg, what is the LVOT peak instantaneous systolic gradient? MR Velocity = 720 cm/sec Left Atrial Pressure = 15 mmhg Systolic BP = 110 mmhg mmhg mmhg mmhg mmhg 42
 2 = 207 LVOT gradient 112 LAP 15 LA Aortic Systolic BP = 110 Ao 112mmHg 5.")
43 MR Velocity = 7.2 m/sec Systolic BP = 110 mmhg LV LV Pressure 222 P 4 (7.2) 2 = 207 LVOT gradient 112 LAP 15 LA Aortic Systolic BP = 110 Ao 112mmHg 5.3m/sec 43
44 8. You are called to the ICU to perform an echocardiogram on a 72 year old male with HCM being evaluated for hypotension. The arterial line is recording a systolic blood pressure of 89 mmhg. Your echocardiogram records the following continuous wave Doppler profiles from the left ventricle. Assuming a left atrial pressure of 15mmHg you conclude that the arterial line is providing an inaccurate reading and you report an estimated systolic blood pressure of xx mmhg? 3.6 m/sec 4.3 m/sec 7.0 m/sec 6.5 m/sec mmhg mmhg mmhg mmhg mmhg 44
45 mmhg mmhg mmhg mmhg mmhg MR LVOT 4.3 m/sec 74 mmhg 45
 2 + 15 SBP = 74 mmhg SBP = 137 mmhg 7.0 m/sec 6.5 m/sec 3.")



46 Left Atrial Pressure = 15 mmhg 4 (7.0) SBP = 74 mmhg SBP = 137 mmhg 7.0 m/sec 6.5 m/sec 3.6 m/sec 4.3 m/sec 74 mmhg 9. A 71 year old women, has had a murmur since childhood and was diagnosed with hypertrophic cardiomyopathy. She is increasingly symptomatic with shortness of breath with minimal exertion (NYHA III). She is referred for consideration of surgical myectomy. You perform a transthoracic echocardiogram and from the findings you make the following conclusion? 46
47 A. Confirm the diagnosis of hypertrophic cardiomyopathy and proceed with myectomy. B. The Doppler signal is mitral regurgitation and the patient may not be a candidate for a myectomy. C. There is valvular aortic stenosis. D. There is subvalvular aortic stenosis A. Confirm the diagnosis of hypertrophic cardiomyopathy and proceed with myectomy. B. The Doppler signal is mitral regurgitation and the patient may not be a candidate for a myectomy. C. There is valvular aortic stenosis. D. There is subvalvular aortic stenosis 47


48 Congenital Fibromuscular Subaortic Stenosis 9. An 18 year old male had a syncopal episode after a blood donation. Because of this event he presented for a pre-participation medical evaluation prior to playing ice hockey at a division 1 college program. Which echocardiographic finding is most consistent with athletes heart? a. Left ventricular wall thickness to be > 13mm. b. Left ventricular end-diastolic diameter to be reduced. c. Left ventricular global longitudinal peak systolic strain to be more negative than (<) - 16%. d. Abnormal left ventricular filling. 48
49 9. An 18 year old male had a syncopal episode after a blood donation. Because of this event he presented for a pre-participation medical evaluation prior to playing ice hockey at a division 1 college program. Which echocardiographic finding is most consistent with athletes heart? a. Left ventricular wall thickness to be > 13mm. b. Left ventricular end-diastolic diameter to be reduced. c. Left ventricular global longitudinal peak systolic strain to be more negative than (<) - 16%. d. Abnormal left ventricular filling. 10. Mitral regurgitation that is secondary to systolic anterior motion of the mitral valve has a jet generally travelling in which direction? a. Directed anteriorly. b. Directed infero-laterally. c. Is centrally directed. d. Often produces two distinct mitral regurgitation jets that flow in opposite directions. 49
50 10. Mitral regurgitation that is secondary to systolic anterior motion of the mitral valve has a jet generally travelling in which direction? a. Directed anteriorly. b. Directed infero-laterally. c. Is centrally directed. d. Often produces two distinct mitral regurgitation jets that flow in opposite directions. Echocardiography in Systemic Disease Sunil V. Mankad, MD, FASE 50


51 Question 1 A 68-year-old man presents with fatigue and abdominal bloating. On cardiac exam, the jugular venous pressure revealed CV waves to angle of the jaw. An RV lift is present. There is a grade 2/6 pansystolic murmur at the lower sternal border that gets louder with inspiration. There is a soft systolic ejection murmur and diastolic murmur at the second left interspace. In addition, there is an enlarged and pulsatile liver. Images obtained from his TTE are shown. Which of the following is the most likely diagnosis? 1. Rheumatic heart disease 2. Carcinoid heart disease 3. Ebstein s anomaly 4. Endocarditis 51


52 Question 2 What is the most likely etiology of the mixed valve disease in this 56 year old patient with a hx of Hodgkins Lymphoma? Courtesy of Dr. WK Freeman 52


53 What is the most likely etiology of the mixed valve disease in this 56 year old patient with a hx of Hodgkins Lymphoma? 1. Chemotherapy induced valve disease 2. Radiation induce valve disease 3. Ergotamine induced valve disease 4. Degenerative calcific valve disease Radiation Induced Cardiac Disease Pancarditis: pericardial, myocardial,endocardial/valvular (fibroelastosis) Acute pericarditis during therapy Delayed pericarditis: constriction, pericardial effusion Cardiomyopathy: diastolic/systolic dysfunction CAD: intimal proliferation, endothelial dysfunction Conduction system defects 53

54 Radiation Therapy for Hodgkin s Lymphoma Cardiovascular Effects in 404 Patients (Treated ) Incidence Median Time After Therapy Coronary Artery Disease 10.4% 9 Yrs Carotid ± Subclavian Disease 7.4% 17 Yrs Significant Valvular Disease 6.2% 22 Yrs Hull MC, et al. JAMA 2003; 290:2831 Radiation Therapy for Hodgkin s Lymphoma Clinically Significant Valvular Disease Aortic Stenosis (48%) Mitral Regurgitation (28%) Mitral Stenosis (10%) Tricuspid Regurgitation (10%) Hull MC, et al. JAMA 2003; 290:2831 Aortic Regurgitation (4%) 54



55 Question 3 What is the most likely diagnosis in this 58 yo man with pulmonary infiltrates and syncope? 55

 C.")


56 What is the most likely diagnosis in this 58 yo man with pulmonary infiltrates and syncope? A. Ischemic Cardiomyopathy B. Arrythmogenic RV Cardiomyopathy (ARVC) C. Cardiac Sarcoidosis D. Systemic Lupus Erythematosus Cardiac Sarcoidosis Noncaseating granuloma Regional wall motion abnormalities in unusual distribution Heart block Sudden death Courtesy William Edwards, MD 56

 LV scar RWMAs Mitral valve regurgitation Pulmonary hypertension Sekhri V et al.")
57 Sarcoidosis Granulomas 11% right atrium 7% left atrium 73% interventricular septum 96% left ventricular free wall 46% right ventricular wall Bargout R: Int J Cardio, 2004 Sarcoidosis Echo features Echo abnormalities are rare LV dilatation LV aneurysms Cardiac Sarcoidosis (Echo) LV scar RWMAs Mitral valve regurgitation Pulmonary hypertension Sekhri V et al. Arch Med Sci



58 Question 4 33 Year Old Female with Lupus Erythematosus, antiphospholipid antibody positive, negative blood cultures, and multiple strokes TEE TEE What is the most likely diagnosis? 1. Staph aureus endocarditis 2. Libman-Sacks endocarditis 3. Thickened bicuspid aortic valve 4. Eosinophilic valvulitis Surgical Specimen 58
 vegetations Courtesy of W Edwards MD Question 5")
59 Systemic Lupus Erythematosus - Cardiac Involvement Pericarditis (fluid ANA+) Lupus anticoagulant Anticardiolipin antibodies Myocarditis Coronary arteritis Libman-sacks (marantic) vegetations Courtesy of W Edwards MD Question 5 59

60 What is the most likely diagnosis in this 35 year old female with a history of migraine headaches and no history of rheumatic fever? 1. Ergot associated valvular disease 2. Aortic and mitral valve endocarditis 3. Parachute mitral with coexistent aortic regurgitation 4. Left sided carcinoid valve disease Drug-Induced Valvular Disease Echocardiographic Findings Thickening and retraction of valve leaflets or cusps Mimics Rheumatic - No commissural fusion Valve Disease - Reduced mobility, restricted closure coaptation Thickened, fused, shortened MV/TV chordal support apparatus Variable regurgitation, rarely significant stenosis 60
 0 Restricted MV motion 7 (24%) 0 TR Grade 2/4 13 (45%) 0 Restricted TV motion 7 (24%) 0 AR Grade 1/4 4 (14%) 0 PREVALENCE OF MDMA ABUSE: 0.")
61 Bhattacharyya S, et al. Lancet 2009; 374:577 MDMA (3,4-Methylenedioxymethamphetamine) Echo Findings with Ecstasy Abuse MDMA Users (n=33) Controls (n=29) Duration of use 6.1 ± 3.4 yrs 0 Age (yrs) 24.3 ± ± 3.1 MR Grade 2/4 4 (14%) 0 Restricted MV motion 7 (24%) 0 TR Grade 2/4 13 (45%) 0 Restricted TV motion 7 (24%) 0 AR Grade 1/4 4 (14%) 0 PREVALENCE OF MDMA ABUSE: 0.4 6% WORLDWIDE Droogmans S, et al. Am J Cardiol 2007; 100:
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
ASCeXAM / ReASCE. Practice Board Exam Questions. Monday Afternoon
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
ASCeXAM / ReASCE Practice Board Exam Questions Monday Afternoon Aortic Valve Prostheses Aortic Regurgitation Stress Echocardiography Ischemic Heart Disease and Myocardial Infarction 3D Echocardiography
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
ASCeXAM / ReASCE. Practice Board Exam Questions. Tuesday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
ASCeXAM / ReASCE Practice Board Exam Questions Tuesday Morning Congenital Heart Disease in Adults Congenital Heart Disease Cases Diastolic Function Pericardial Disease Congenital Heart Disease Cases Michael
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
G. AORTIC STENOSIS (AS)
") G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
G. AORTIC STENOSIS (AS) DEFINITION THE FACTS Aortic stenosis (AS) is a narrowing/thickening/obstruction of the aortic valve (AOV) that impedes systolic flow traveling from the left ventricle, through the
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Pericardial Disease: Case Examples. Echo Fiesta 2017
 Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Pericardial Disease: Case Examples Echo Fiesta 2017 2014 2014 MFMER MFMER 3346252-1 slide-1 Objectives Have a systematic approach to evaluation of constriction 2014 MFMER 3346252-2 CASE 1 2013 MFMER 3248567-3
Diastolic Function Assessment New Guideline Update Practical Approach
 Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
Mayo Clinic Department of Cardiovascular Diseases Mayo Clinic Echocardiography Review Course for Boards and Recertification Diastolic Function Assessment New Guideline Update Practical Approach Jae K.
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Diastolic Heart Function: Applying the New Guidelines Case Studies
 Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
Diastolic Heart Function: Applying the New Guidelines Case Studies Mitral Regurgitation The New ASE William Guidelines: A. Zoghbi Role MD, of FASE, 2D/3D MACCand CMR Professor and Chairman, Department
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Uptofate Study Summary
 CARDIOLOGY: Valvulopathies Aortic Stenosis 1. Aetiology is age dependant - Age > 70: Senile calcification (50%), rheumatic (25%), biscupid (25%) - Age < 70: Bicuspid (75%), rheumatic (25%) - Note: Rheumatic
CARDIOLOGY: Valvulopathies Aortic Stenosis 1. Aetiology is age dependant - Age > 70: Senile calcification (50%), rheumatic (25%), biscupid (25%) - Age < 70: Bicuspid (75%), rheumatic (25%) - Note: Rheumatic
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS
 MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
MAKING SENSE OF MODERATE GRADIENTS IN PATIENTS WITH SYMPTOMATIC AORTIC STENOSIS David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
ECHO HAWAII. Role of Stress Echo in Valvular Heart Disease. Not only ischemia! Cardiomyopathy. Prosthetic Valve. Diastolic Dysfunction
 Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Role of Stress Echo in Valvular Heart Disease ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan Not only ischemia! Cardiomyopathy Prosthetic Valve Diastolic
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Quantification of Aortic Regurgitation
 Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
Quantification of Aortic Regurgitation ASE Review 2018 Boston Susan E Wiegers, MD, FASE, FACC Professor of Medicine And thanks to Dr. Roberto Lang Disclosure None related to this presentation 1 Objectives
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Stage of Valvular AS. Outline 10/14/16. Low-flow and Other Challenges to the Assessment of Aortic Stenosis. Severe AS
 Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
Low-flow and Other Challenges to the Assessment of Aortic Stenosis Nithima Ratanasit, MD, FACC, FASE Siriraj Hospital, Mahidol University Bangkok, Thailand Outline Types of low-flow aortic stenosis Assessment
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT
 ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
ECHOCARDIOGRAPHIC APPROACH TO CONGENITAL HEART DISEASE: THE UNOPERATED ADULT Karen Stout, MD, FACC Divisions of Cardiology University of Washington Medical Center Seattle Children s Hospital NO DISCLOSURES
PRINCIPLES OF ENDOCARDITIS
 015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Usually we DON T need to go beyond the gradient
 Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Aortic Stenosis Going Beyond the Gradient James D. Thomas, MD, FACC, FASE Director, Center for Heart Valve Disease Bluhm Cardiovascular Institute Professor of Medicine, Feinberg School of Medicine, Northwestern
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic evaluation of mitral stenosis
 Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Echocardiographic evaluation of mitral stenosis Euroecho 2011 Philippe Unger, MD, FESC Erasme Hospital, ULB, Brussels, Belgium I have nothing to declare EuroHeart Survey Etiology of single native left-sided
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
pulmonary valve on, 107 pulmonary valve vegetations on, 113
 INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
INDEX Adriamycin-induced cardiomyopathy, 176 Amyloidosis, 160-161 echocardiographic abnormalities in, 160 intra-mural tumors similar to, 294 myocardial involvement in, 160-161 two-dimensional echocardiography
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation
 Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Case Reviews: Hemodynamic Calculations in Valvular Regurgitation Case 5 History: 69-year-old man with orthotopic heart transplant 15 years ago. Inferior MI several years ago. Recurrent CHF. Currently dyspneic
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation
 Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Imaging Assessment of Aortic Stenosis/Aortic Regurgitation Craig E Fleishman, MD FACC FASE The Heart Center at Arnold Palmer Hospital for Children, Orlando SCAI Fall Fellows Course 2014 Las Vegas Disclosure
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo
 Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Diastolic Function Assessment Practical Ways to Incorporate into Every Echo Jae K. Oh, MD Echo Hawaii 2018 2018 MFMER 3712003-1 Learning Objectives My presentation will help you to Appreciate the importance
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function
 Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Basic Approach to the Echocardiographic Evaluation of Ventricular Diastolic Function J A F E R A L I, M D U N I V E R S I T Y H O S P I T A L S C A S E M E D I C A L C E N T E R S T A F F C A R D I O T
Cardiac MRI: Clinical Application to Disease
 Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
Cardiac MRI: Clinical Application to Disease Jessi Smith, MD Cardiothoracic imaging, Indiana University Slides courtesy of Stacy Rissing, MD Outline Imaging planes Disease findings Pulse sequences used
HISTORY. Question: What type of heart disease is suggested by this history? CHIEF COMPLAINT: Decreasing exercise tolerance.
 HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
HISTORY 15-year-old male. CHIEF COMPLAINT: Decreasing exercise tolerance. PRESENT ILLNESS: A heart murmur was noted in childhood, but subsequent medical care was sporadic. Easy fatigability and slight
Outline. EuroScore II. Society of Thoracic Surgeons Score. EuroScore II
 SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
SURGICAL RISK IN VALVULAR HEART DISEASE: WHAT 2D AND 3D ECHO CAN TELL YOU AND WHAT THEY CAN'T Ernesto E Salcedo, MD Professor of Medicine University of Colorado School of Medicine Director of Echocardiography
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention
 Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Degenerative Mitral Regurgitation: Etiology and Natural History of Disease and Triggers for Intervention John N. Hamaty D.O. FACC, FACOI November 17 th 2017 I have no financial disclosures Primary Mitral
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer
 «Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
«Paradoxical» low-flow, low-gradient AS with preserved LV function: A Silent Killer Philippe Pibarot, DVM, PhD, FACC, FAHA, FESC, FASE Canada Research Chair in Valvular Heart Diseases Université LAVAL
Interventions in Adult Congenital Heart Disease: Role of CV Imaging. Associate Professor. ACHD mortality. Pillutla. Am Heart J 2009;158:874-9
 Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Interventions in Adult Congenital Heart Disease: Role of CV Imaging Sangeeta Shah MD, FACC, FASE Associate Professor ACHD mortality Pillutla. Am Heart J 2009;158:874-9 Adult Congenital Heart Disease Heterogenity
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
Mitral Valve Disease. Chapter 29
 Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Cases in Adult Congenital Heart Disease
 Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Cases in Adult Congenital Heart Disease Sabrina Phillips, MD FACC FASE Associate Professor of Medicine The University of Oklahoma Health Sciences Center No Disclosures I Have Palpitations 18 Year old Man
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Quantitation of Aortic Regurgitation ASCeXAM / ReASCE Review Course
 Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Quantitation of Aortic Regurgitation 2017 ASCeXAM / ReASCE Review Course David Adams, ACS, RCS, RDCS, FASE Duke University Medical Center May 1, 2017 Disclosures None 1 Exam based on: Zoghbi et al. JASE
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following