TRANSTHORACIC ECHOCARDIOGRAPHY (TTE) An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015
|
|
|
- Barbara Marilynn Wilkins
- 6 years ago
- Views:
Transcription


1 TRANSTHORACIC ECHOCARDIOGRAPHY (TTE) An overview for Perioperative Care Dr Andrew Cluer, Sydney, Australia 2015 This piece of work is not meant to teach students echo interpretation, but instead offers an insight into interpretation and gives the reader a broad understanding of the uses and limitations of this powerful technology. It is important to recognise from the outset that echo data should be considered in clinical context and as such is useful when it corroborates clinical suspicions and often misleading when used in isolation. This is particularly so when a doctor says I know, lets get an echo! Both images and clips are included for student interest. By way of introduction and for those students who have never been introduced to the technical aspects of ultrasound, Wikipedia is on hand to help! This link acts as a good introduction, but it is not considered essential reading for this echo review. Rather the piece adds value where students would like to read more widely. Indications for resting preoperative transthoracic echocardiogram (TTE) have been published by the European Society of Cardiology (ESC)/European Society of Anaesthesiology (ESA), British Society of Echocardiography (BSE) and American Heart Association (AHA)/American College of Cardiology (ACC) (see links at the end of the document). For ease of reading the documents have been summarised in Table 1. These guidelines are extremely useful but it is worth noting they do not adequately address some important issues such as suspected or known pulmonary hypertension (PHT). Where deficient supplemental links are provided. In general terms the advantages of resting preoperative Trans Thoracic Echocardiography (TTE) in non-cardiac surgical patients are not entirely clear. Wijeysundera et al. (2011) retrospectively looked at over 260,000 patients who had undergone medium or high risk non-cardiac surgery and found that preoperative resting TTE was not associated with either a decreased hospital stay or an improved survival. Although retrospective this very large study suggests that much more research needs to be done to define which patients benefit from an increasingly common preoperative investigation. A relatively recent editorial in Anaesthesia (Heyburn & McBrien 2012) has actually advocated resting preoperative TTE for all patients with hip fractures though these recommendations are not reflected in any current international guidelines. Despite the above it is generally accepted that for specific individuals TTE can have a major impact on their perioperative clinical management. TTE enables rapid assessment of cardiac structure and function. It has certain advantages over Transoesophageal Echocardiography (TOE) including superior assessment of aortic valve areas and gradients, better imaging of the left ventricular apex and more accurate assessment of ejection fraction (EF%). It is also non-invasive, quicker and involves minimal risk to the patient. Indications for TOE include imaging of the mitral valve prior to cardiac surgery, detailed assessment of atrial structures,
2 suspected aortic dissection and investigation of endocarditis and is rarely indicated in the perioperative period. It is important to understand that TTE is a snapshot at one particular point in time. This is not an issue in euvolaemic, hemodynamically stable patients but can be of relevance at other times in the perioperative period. In the unstable patient measurements made using TTE can change rapidly and are dependent on many factors including volume loading, inotrope use and lung ventilatory settings. It may therefore be appropriate to carry out serial examinations in the perioperative period, echo being used as a monitor rather than a diagnostic tool. It is also important to understand that TTE is a snapshot at rest and therefore has a very limited role in the preoperative assessment of ischaemic heart disease. Recommendations on preoperative imaging stress testing are included in the ESC/ESA and AHA/ACC documents mentioned above. A skilled echocardiographer will always acquire a set of standard views and measurements however, they will seek to obtain extra information dependent on the patient information provided. It is therefore essential that TTE referrals state the clinical question to be answered. A comprehensive echocardiographic assessment of pulmonary hypertension is very different to an assessment of aortic stenosis. A case study in heart failure Mrs P is a 60 years old lady reviewed in the surgical pre-assessment clinic prior to planned Oesophagectomy for cancer. The patients past medical history includes:- Paroxysmal Atrial Fibrillation (anticoagulated) Non-Insulin Dependent Diabetes Mellitus New onset paroxysmal nocturnal dyspnoea and orthopnoea Exercise tolerance is currently 50 metres on the flat A systolic murmur is heard on auscultation The TTE request states Please assess biventricular function, pulmonary pressures and check for any valvular pathology. Mrs P s TTE report provides an overall picture of her cardiac structure and function. Like all reports it should make sense clinically and the individual components must fit together. For example, severely impaired left ventricular (LV) systolic function will generally be associated with some diastolic dysfunction, severe mitral regurgitation (MR) will generally be associated with significantly raised pulmonary pressures and significant diastolic dysfunction will generally be accompanied by a large left atrium. Aspects of a TTE report that do not make clinical sense imply some errors in measurement may have been made and should be viewed with suspicion. Understanding the overall message an echocardiographer or cardiologist is trying to convey with a TTE report is more important than simply focusing on isolated numbers such as ejection fraction (EF%). The reference ranges of most TTE
3 measurements are affected by age and sex. Many measurements should also be indexed to Body Surface Area (BSA) so a patient s height and weight should ideally be recorded (when was the last time you included this data in your request for investigation?). For example a Left Ventricular End Diastolic Diameter (LVEDD) of 6.0cm can be normal for a large man but very abnormal for a small woman. The British Society of Echocardiography smartphone app. is free to download and is a useful reference for normal and abnormal values. Medical practitioners often view a TTE report as a bewildering array of data and focus only on the short written conclusion which can occasionally be falsely reassuring. It is important to understand that an echocardiographer and clinician may regard different aspects of a TTE report as being significant. To get the most out of a report it is better to try and separate the meaningful data from the less helpful measurements and gain a deeper understanding of all the information provided. For example EF% (measured by Simpsons Biplane technique) is a validated and reproducible measurement, whereas EF% (measured by Teichholz technique) is not. A summary of the most useful measurements on a TTE report is provided in Table 2 and the following discussion aims to provide some guidance on how to interpret the data. Understanding the detail: A guide to echo interpretation The detail below is not meant to be memorised, rather the student should begin to understand what elements of the investigation are globally assessed (often with the experienced eyeball) and which are measured. For both elements of assessment it is important to appreciate the scope for error. 1. LEFT VENTRICLE: Assessment of the left ventricle should be divided into structure and function (systolic and diastolic). Structure - The most important aspects of LV structure are size and wall thickness. Both are measured at end diastole on a Parasternal Long-Axis View (PLAX) (Video 1 - PLAX) The thickness of the interventricular septum (IVS) and posterior wall (PW) is routinely reported along with any other abnormalities such as asymmetric hypertrophy or scarred myocardium. Structure of the LV also includes other pathology such as thrombus or septal defects. Simple 2-D measurements (see wiki link to understand these modes of imaging) are generally more accurate than M- Mode, which can overestimate the LV diameter if not careful. It is important to note that isolated basal septal hypertrophy can be a normal finding in the elderly and should not be confused with hypertrophic cardiomyopathy. Mrs P: LV Diastolic Diameter = 5.6cm, IVS = 0.9cm, PW = 1.0cm. Conclusion = mildly dilated LV with normal wall thickness. (Image 1 LV Size & Wall Thickness)
 and Apical 2 Chamber (Video 3 - A2C).")
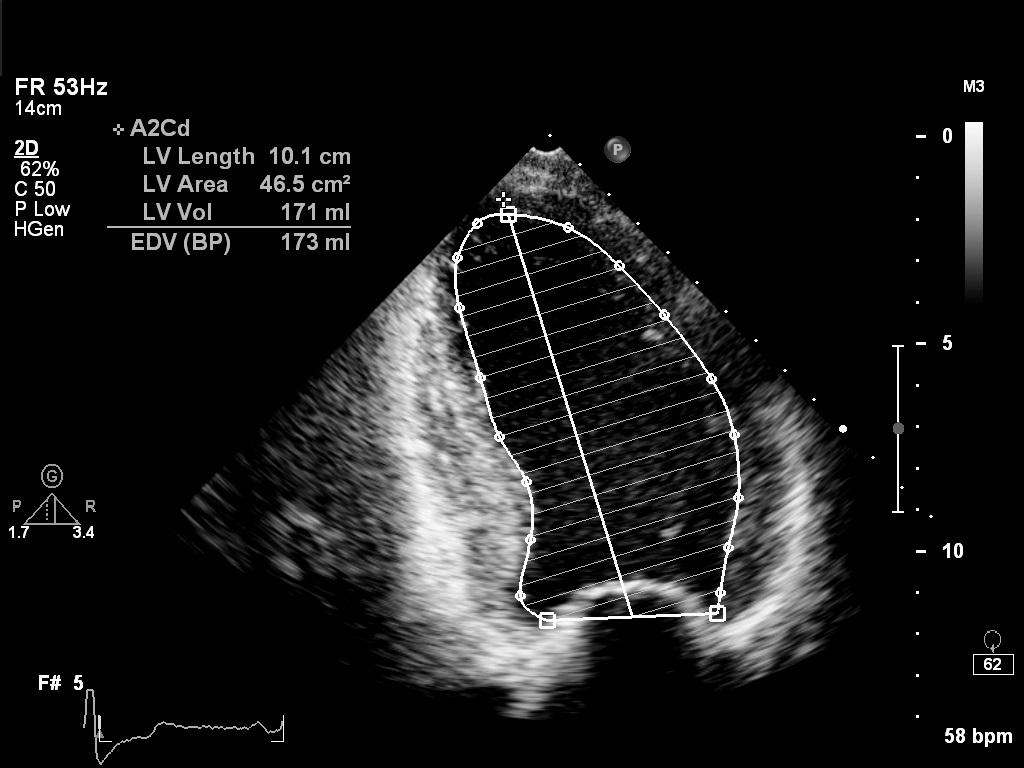
4 Image 1 Systolic Function - LV systolic function can be globally or regionally impaired. Quantification of systolic function is best achieved by calculating an EF% using Simpson s Biplane method. Views required are the Apical 4 Chamber (Video 2 A4C) and Apical 2 Chamber (Video 3 - A2C). On occasions an experienced echocardiographer will visually estimate the EF% or simply quantify systolic function as good overall function or mild, moderate or severe impairment. It is an interesting and important fact that visual estimates by experienced practitioners are as useful as a calculated EF%. Regional wall motion abnormalities (RWMA) usually imply ischaemic heart disease and their distribution often assists in determining the specific coronary artery affected. For example, an akinetic LV apex and anterior septum is likely secondary to disease of the left anterior descending coronary artery. RWMA can be subtle and difficult to identify and there are often variations in reporting between echocardiographers. Segmental basal inferior and inferoseptal hypokinesis is commonly reported and of little significance. Apical akinesis should always raise the suspicion of a thrombus and some departments will routinely investigate with a contrast study. Mrs P: LV Ejection Fraction = 20.2%. Conclusion = Global, severe impairment of systolic function. (Image 2,3,4 & 5)
5 Image 2

6 Image 3 Image 4
7 Image 5 Diastolic Function (dysfunction - alternatively known as heart failure with preserved ejection fraction). LV Diastolic function assessment is complex and interested readers are directed to ESC guidelines on this topic (Link provided at the end of the document). An important distinction to make is whether there is isolated LV diastolic dysfunction or does it accompany LV systolic dysfunction. Traditionally diastolic dysfunction is graded (1-4) using Doppler patterns from mitral inflow (Mitral E and A waves) and tissue Doppler from LV Septal (E Septal Velocity) and LV Lateral Walls (E Lateral Velocity). Grade 1 dysfunction is defined as impaired relaxation whereas Grade 4 dysfunction is defined as irreversible restrictive disease. In the presence of normal systolic function it is appropriate to grade diastolic dysfunction in this manner. Importantly type 1 diastolic dysfunction in the elderly is a normal finding. E/E ratio is the most useful measurement and an E/E Septal > 15 or E/E Lateral > 12 is abnormal. Diastolic dysfunction is generally always present in patients with significantly impaired LV systolic function and in this situation it makes more sense to try and quantify elevations in left atrial pressure. E/E is useful and will increase as left atrial pressure (LAP) increases. E/E is therefore a dynamic measurement and changes with fluid loading. Mrs P: Mitral E to LV E Septal Ratio = Conclusion = Severely elevated LAP (Image 6 Mitral E & A Waves, Image 7 - E Septal Velocity)

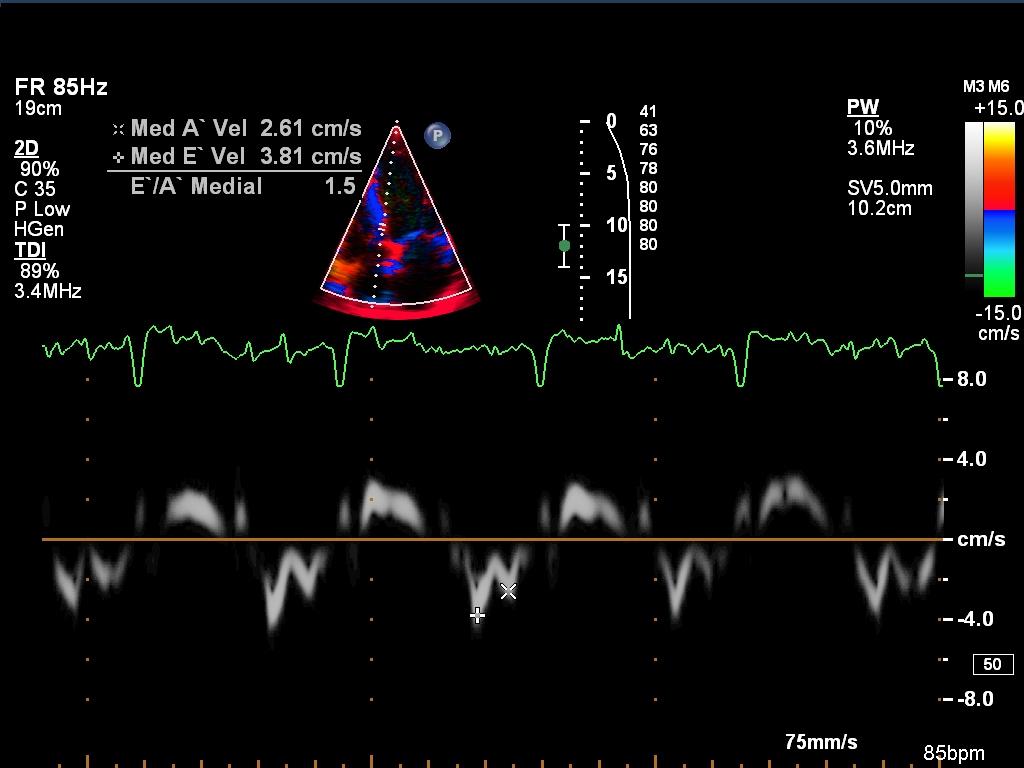
8 Image 6 Image 7
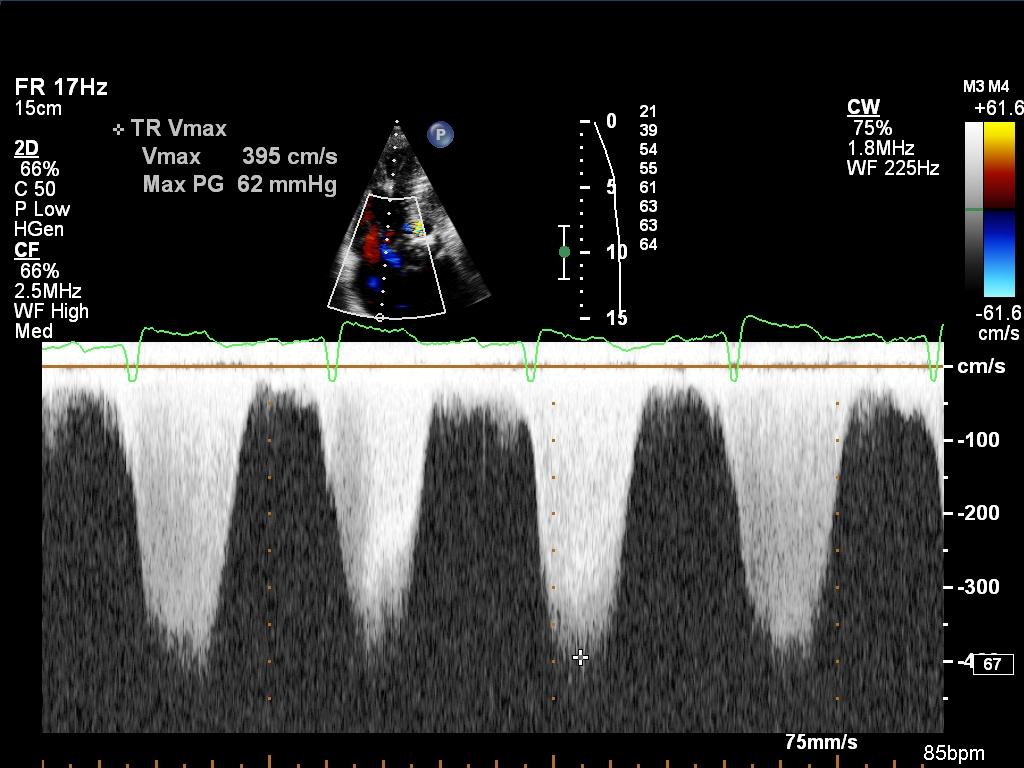
9 2. RIGHT VENTRICLE: The right ventricle (RV) is best assessed qualitatively for size, structure and function. Few quantitative measurements are useful. If the RV is enlarged and has normal systolic function then it is likely to be volume overloaded (Tricuspid Regurgitation (TR), Pulmonary Regurgitation or Atrial Septal Defect). If the RV is enlarged and has significantly impaired systolic function then possible pathology includes RV pressure overload, cardiomyopathy or infarction. Tricuspid Annular Plane Systolic Excursion (TAPSE) is often quoted as a quantitative measure of RV systolic function but in reality only reflects basal RV function and provides no information about the RV free wall. Mrs P: Qualitative comment Normal RV size and mildly impaired systolic function (Video 4 - RV). TAPSE = 1.5cm (Image 8) Calculation of Right Ventricular Systolic Pressure (RVSP) or Pulmonary Artery Systolic Pressure (PASP) is relatively easy and an extremely useful measurement in the assessment of PHT. RVSP = 4 x (Peak TR Velocity) 2 + Right Atrial Pressure (RAP). RAP is estimated from the size of the Inferior Vena Cava (IVC) and its collapsibility on deep inspiration (Video 5 IVC). It is important to note that pulmonary hypertension is defined by mean pulmonary artery pressure (link provided) and not PASP (or RVSP) which is quoted on a TTE report. Comprehensive echocardiographic assessment of PHT has been outlined in an excellent document written by Hammersmith Hospital Cardiology Department (link provided). Mrs P: TR Peak Velocity = 3.95m/sec, RAP = 10mmHg. PASP =72.4mmHg. Conclusion = moderate/severe elevation in pulmonary pressures. (Video 6 TR Colour Doppler, Image 9 Peak TR Velocity)

10 Image 8 Image 9

11 3. ATRIA: Atria are considered as the window to the ventricles. For example the first sign of significant LV diastolic dysfunction is an enlarged left atrium. Qualitative comments about the shape of the interatrial septum can also help with the assessment of left and right atrial pressure. Volumetric measurements are most accurate. Mrs P: LA Volume = 66.5mls. Conclusion = Enlarged Left Atrium. (Image 10 LA Volume) Image VALVES: Assessment of each valve should be by structure and function. Structure is usually assessed by zoomed 2D images whereas assessment of valvular function requires Doppler interrogation of blood flow through the valve. Doppler interrogation requires excellent technical skills and off axis measurements (misaligned Doppler cursor) can significantly underestimate trans-valvular gradients. Reference ranges for all measurements can be found on the BSE smartphone app. Tricuspid & Pulmonary Valves - TR and PR are usually assessed by eyeballing the colour Doppler regurgitant jet. Mild TR and PR is of no clinical significance. Severe TR causes flow reversal in the hepatic veins. Both tricuspid and pulmonary stenosis is rare but trans-valvular gradients can be measured. In general qualitative comments about the tricuspid and pulmonary valves are sufficient. Mrs P: Structurally normal tricuspid valve with moderate regurgitation. Structurally normal pulmonary valve with no regurgitation.
.")
12 Aortic Valve (AV) - Significant aortic stenosis is usually diagnosed by the appearance of calcified and restricted leaflets on Para-sternal long axis (PLAX) and Parasternal Short Axis (PSAX) views (Video 7 PLAX Aortic Stenosis & Video 8 PSAX Aortic Stenosis. Both videos are provided as examples but are not relevant to the case of Mrs P). The continuity equation is the most accurate method of estimating aortic valve area and is given by the equation below. Extremely accurate measurements from the Left Ventricular Outflow Tract (LVOT) are required. It is assumed that the LVOT is a circle and therefore LVOT area is simply calculated using the formula πr 2. Importantly small errors measuring the LVOT diameter or radius are magnified because the value is then subsequently squared in the calculation. Velocity Time Integrals (VTI) are usually calculated automatically by standard software installed on most ultrasound machines. Aortic Valve Area = (LVOT VTI x LVOT Area)/Aortic Valve VTI (Images 11 LVOT Diameter, Image 12 LVOT VTI, Image 13 AV VTI. These images are provided as examples but are not relevant to the case of Mrs P). Pressure gradients across a stenotic valve are also used to grade severity but they are more prone to error and can be affected by other factors such as LV systolic function. Interested students are directed to the ESC guidelines (link provided). Aortic regurgitation is assessed by a combination of methods including colour and spectral Doppler. Mrs P: No measurements needed as valve normal. Only a qualitative comment Structurally normal trileaflet valve with no significant regurgitation Image 11
 but information derived from Doppler interrogation is also useful.")
13 Image 12 Mitral Valve - Mitral stenosis is 99% rheumatic in aetiology and the valve has a characteristic hockey stick appearance on PLAX view. Mitral valve area is best calculated by tracing around the open valve leaflets in a PSAX view (planimetry) but information derived from Doppler interrogation is also useful. Mitral regurgitation (Video 9 - MR) is the most difficult of valvular lesions to accurately assess and interrogation from all parasternal and apical views in required. The most accurate way to quantify MR is by calculating regurgitant volume from measurement of Proximal Isovelocity Surface Area (PISA) on colour Doppler (Image 13- PISA). The aetiology of MR should always be stated and can be divided into organic or functional causes. Mild MR is of no clinical significance. Interested students are again directed to the ESC guidelines (link provided) Mrs P: MR Regurgitant Volume PISA = 43.9mls. Conclusion = Moderate functional MR AORTA, PERICARDIUM & OTHER FINDINGS: The aorta can be assessed at many points (ascending, arch, descending) using TTE. Standard measurements include the width at the level of aortic sinuses. Pericardial effusions are measured at end diastole and quantified as small, moderate or large however, size is less important than whether there are any echocardiographic signs of hemodynamic compromise as a result of the pericardial effusion.

14 Image 13 Many additional findings can be identified on TTE including non-cardiac pathology such as pleural effusions and abdominal aortic aneurysms. SIGNIFICANT FINDINGS ON PERIOPERATIVE TTE In patients scheduled for non-cardiac surgery it is also helpful to consider the question of what constitutes a significant finding on preoperative resting TTE. Significant findings can be considered as those which affect perioperative risk stratification, alter clinical (medical, anaesthetic or surgical) management and at the extreme end of the scale those findings which lead to cardiac surgical intervention prior to undergoing non-cardiac surgery. Left ventricular (LV) systolic heart failure is considered a risk factor for adverse perioperative cardiac events and is a component of several clinical risk indices. Kazmers et al. (1988) found an LV ejection fraction (EF) of less than 35% to be the most accurate predictor of adverse perioperative events and this was confirmed by Hammill et al. (2008). Matyal et al. (2009) showed that diastolic dysfunction was an independent risk factor for perioperative congestive heart failure in a study of 313 high risk patients undergoing vascular surgery. However, more research is certainly needed in this particular area. Diastolic dysfunction is often not assessed preoperatively and does not feature on any commonly utilized clinical risk indices and may be an evolving pathology that we will begin to understand better in the future.
15 With regards to valvular function it is helpful to consider stenotic and regurgitant pathology separately with stenotic pathology being more poorly tolerated by patients undergoing non- cardiac surgery. The ACC/AHA considers severe stenotic valvular disease (AS with a valve area of <1 sq cm and symptomatic mitral stenosis (MS)) as one of four active cardiac conditions that require evaluation and treatment prior to non-cardiac surgery. The issue with regards to valvular regurgitation in patients undergoing non-cardiac surgery is more complex. The ESC/ESA guidelines (Dalby Kristensen et al. 2014) advise that asymptomatic patients with preserved LV systolic function and severe mitral regurgitation (MR) or aortic regurgitation (AR) are not at increased perioperative risk. The 2014 ACC/AHA Valvular Heart Disease Guidelines (Nishimura et al. 2014) state that it is reasonable to perform moderate risk non-cardiac surgery, with appropriate haemodymanic monitoring, on patients with asymptomatic severe MR and asymptomatic severe AR if EF% is preserved. Although it may be reasonable to proceed with surgery in these cases prior diagnosis and accurate quantification of valvular regurgitation is clearly essential for perioperative planning. In addition there will be many other factors that determine how an individual patient is managed. Pulmonary hypertension (PHT) is another area of uncertainty with most evidence coming from observational data of patients with pulmonary arterial hypertension (Type 1 PHT). However, complication rates are extremely high in this group with significant perioperative morbidity and mortality. Both the ESC/ESA and ACC/AHA make a number of recommendations regarding the perioperative management of patients with PHT including thorough evaluation and optimisation by a PHT specialist prior to surgery. It is known that elevations in right atrial pressure (RAP) and reduced cardiac output are more important than isolated elevations in right ventricular systolic pressure (RVSP) as the former are representative of right ventricular (RV) failure. An RVSP >70mmHg has, nevertheless been identified as a risk factor for adverse perioperative events (Minai et al. 2014). It is extremely unlikely there will ever be any studies looking at major incidental findings such as intra-cardiac mass or pericardial effusion on preoperative resting TTE however, it would seem logical to consider these findings significant. The challenge of interpreting a preoperative resting TTE is separating the wood from the trees. The clinician needs to extract all the relevant findings whilst not attaching significance to minor and irrelevant abnormalities such as PASP of 40mmHg in an obese patient or Type 1 diastolic dysfunction in an elderly man. Correct interpretation comes with experience and by studying a large number of TTE reports, seeking advice when necessary from experts in the field. A note regarding the links below Links 1 and 2 are included to give the reader an idea of the complex nature of a diagnostic TTE. Link 3 gives reference ranges for all TTE data (it is not expected this information is committed to memory). Some of the articles referenced in the discussion are also outside the scope of MSc Perioperative Medicine and provided for interest only.
16 Key links:
17 Appendices: Table 1: Indications for Preoperative Resting TTE as per AHA/ACC, ESC/ESA & BSE Indication Patients with shortness of breath (SOB) of unknown origin Heart failure with worsening SOB or other change in clinical state Patients with clinically suspected moderate or greater degrees of valvular stenosis or regurgitation if a/no prior TTE in 1 year or b/significant clinical change since last study. Systolic murmur suggestive of AS Clinical history or physical examination suggests valvular disease Estimate pulmonary artery systolic pressure (PASP) Patients undergoing high risk surgery All patients with known or suspected Valvular Heart Disease, who are scheduled for elective intermediate or high risk, non-cardiac surgery. Ischaemic heart disease & Exercise tolerance < 4 metabolic equivalents (METS) SOB in absence of clinical signs of heart failure. Electrocardiogram (ECG) +/- Chest X-Ray (CXR) abnormal) Heart murmur & cardiac or respiratory symptoms Presence of heart murmur in asymptomatic patient who has clinically suspected severe structural heart disease. Class of Level of Organisation Recommendation Evidence recommending Class IIa Level C AHA/ACC Class IIa Level C AHA/ACC Class I Level C AHA/ACC Appropriate Helpful AHA/ACC AHA/ACC Useful in AHA/ACC perioperative planning Class IIb Level C ESC/ESA Class I Level C ESC/ESA BSE BSE BSE BSE
18 Table 2: Most Useful Measurements on a TTE Report Structure Left Ventricle Size Left Ventricle Wall Thickness Left Ventricle Systolic Function Left Ventricle Diastolic Function Right Ventricle Systolic Function Left Atrium Right Atrium Aorta Pericardium IVC Valves Aortic Stenosis Aortic Regurgitation Mitral Stenosis Mitral Regurgitation Tricuspid Regurgitation Pulmonary Stenosis Measurement Left Ventricular End Diastolic Diameter (PLAX) LV Interventricular Septum (PLAX) LV Posterior Wall (PLAX) LV Ejection Fraction MOD BP E/E, LA Volume TAPSE RV S LA Volume RA Volume Aorta at Sinuses (+other locations) Size of Pericardial Effusion Size and Collapsibility (to estimate RAP) AV Peak Velocity & Gradient AV Mean Gradient AV Area Cont Eqn (VTI) AI Pressure Half Time AI Vena Contracta Mitral Valve Area (Planimetry) Pressure Half Time MV Mean Gradient Regurgitant Volume (PISA) TR Peak Velocity (to estimate RVSP/PASP) PV Peak velocity
19 References: Hammill, B.G. et al., Impact of heart failure on patients undergoing major noncardiac surgery. Anesthesiology, 108(4), pp Heyburn, G. & McBrien, M.E., Pre-operative echocardiography for hip fractures: time to make it a standard of care. Anaesthesia, 67(11), pp Kazmers, A. et al., Perioperative and late outcome in patients with left ventricular ejection fraction of 35% or less who require major vascular surgery. J Vasc Surg Sep;8(3): Matyal, R. et al., Perioperative diastolic dysfunction during vascular surgery and its association with postoperative outcome. Journal of vascular surgery, 50(1), pp Minai, O.A. et al., Perioperative risk and management in patients with pulmonary hypertension. Chest, 144(1), pp Nishimura et al., AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease. JAC, 63(22), pp.e57 e185. Wijeysundera, D.N. et al., Association of echocardiography before major elective non-cardiac surgery with postoperative survival and length of hospital stay: population based cohort study. BMJ, 342(jun30 1), pp.d3695 d3695.
British Society of Echocardiography
 British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
British Society of Echocardiography Affiliated to the British Cardiac Society A Minimum Dataset for a Standard Adult Transthoracic Echocardiogram From the British Society of Echocardiography Education
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus. Rapid Cardiac Echo (RCE)
 Syllabus. Rapid Cardiac Echo (RCE)") Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Certificate in Clinician Performed Ultrasound (CCPU) Syllabus Rapid Cardiac Echo (RCE) Purpose: Rapid Cardiac Echocardiography (RCE) This unit is designed to cover the theoretical and practical curriculum
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
The Doppler Examination. Katie Twomley, MD Wake Forest Baptist Health - Lexington
 The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
The Doppler Examination Katie Twomley, MD Wake Forest Baptist Health - Lexington OUTLINE Principles/Physics Use in valvular assessment Aortic stenosis (continuity equation) Aortic regurgitation (pressure
ECHOCARDIOGRAPHY DATA REPORT FORM
 Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Patient ID Patient Study ID AVM - - Date of form completion / / 20 Initials of person completing the form mm dd yyyy Study period Preoperative Postoperative Operative 6-month f/u 1-year f/u 2-year f/u
Hemodynamic Assessment. Assessment of Systolic Function Doppler Hemodynamics
 Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Hemodynamic Assessment Matt M. Umland, RDCS, FASE Aurora Medical Group Milwaukee, WI Assessment of Systolic Function Doppler Hemodynamics Stroke Volume Cardiac Output Cardiac Index Tei Index/Index of myocardial
Assessment of LV systolic function
 Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Tutorial 5 - Assessment of LV systolic function Assessment of LV systolic function A knowledge of the LV systolic function is crucial in the undertanding of and management of unstable hemodynamics or a
Adel Hasanin Ahmed 1
 Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Adel Hasanin Ahmed 1 PERICARDIAL DISEASE The pericardial effusion ends anteriorly to the descending aorta and is best visualised in the PLAX. PSAX is actually very useful sometimes for looking at posterior
Valvular Regurgitation: Can We Do Better Than Colour Doppler?
 Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Valvular Regurgitation: Can We Do Better Than Colour Doppler? A/Prof David Prior St Vincent s Hospital Melbourne Sports Cardiology Valvular Regurgitation Valve regurgitation volume loads the ventricles
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
JFICMI Basic Critical Care Echocardiography (BCCE)
") JFICMI Basic Critical Care Echocardiography (BCCE) 2017 Introduction The International expert statement on training standards for critical care ultrasonography position paper published in Intensive Care
JFICMI Basic Critical Care Echocardiography (BCCE) 2017 Introduction The International expert statement on training standards for critical care ultrasonography position paper published in Intensive Care
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING
 PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
PART II ECHOCARDIOGRAPHY LABORATORY OPERATIONS ADULT TRANSTHORACIC ECHOCARDIOGRAPHY TESTING STANDARD - Primary Instrumentation 1.1 Cardiac Ultrasound Systems SECTION 1 Instrumentation Ultrasound instruments
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Atrial Septal Defects
 Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Supplementary ACHD Echo Acquisition Protocol for Atrial Septal Defects The following protocol for echo in adult patients with atrial septal defects (ASDs) is a guide for performing a comprehensive assessment
Pediatric Echocardiography Examination Content Outline
 Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Pediatric Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 Anatomy and Physiology Normal Anatomy and Physiology 10% 2 Abnormal Pathology and Pathophysiology
Right Heart Evaluation ASE Guidelines Review. Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC
 Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
Right Heart Evaluation ASE Guidelines Review Chris Mann RDCS, RCS, FASE Faculty, Echocardiography Pitt Community College Greenville, NC Objectives Briefly review right atrial and right ventricular anatomy
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
Echocardiography. Guidelines for Valve and Chamber Quantification. In partnership with
 Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
Echocardiography Guidelines for Valve and Chamber Quantification In partnership with Explanatory note & references These guidelines have been developed by the Education Committee of the British Society
LUST trial. Echocardiography USER S MANUAL
 LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
LUST trial Echocardiography USER S MANUAL Rosa Sicari, Luna Gargani Ins1tute of Clinical Physiology Na1onal Council of Research, Pisa, Italy Parameters required (1) Aortic root Measurement of aortic root
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION
 LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
LV FUNCTION ASSESSMENT: WHAT IS BEYOND EJECTION FRACTION Jamilah S AlRahimi Assistant Professor, KSU-HS Consultant Noninvasive Cardiology KFCC, MNGHA-WR Introduction LV function assessment in Heart Failure:
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Echocardiography: Guidelines for Valve Quantification
 Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Echocardiography: Guidelines for Echocardiography: Guidelines for Chamber Quantification British Society of Echocardiography Education Committee Richard Steeds (Chair), Gill Wharton (Lead Author), Jane
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter.
 Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
Comprehensive Hemodynamics By Doppler Echocardiography. The Echocardiographic Swan-Ganz Catheter. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP North Shore HS, LIJ/Lenox Hill Hospital, New York
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Appendix II: ECHOCARDIOGRAPHY ANALYSIS
 Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Appendix II: ECHOCARDIOGRAPHY ANALYSIS Two-Dimensional (2D) imaging was performed using the Vivid 7 Advantage cardiovascular ultrasound system (GE Medical Systems, Milwaukee) with a frame rate of 400 frames
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics.
 Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Echo Doppler Assessment of Right and Left Ventricular Hemodynamics. Itzhak Kronzon, MD, FASE, FACC, FESC, FAHA, FACP, FCCP Northwell, Lenox Hill Hospital, New York Professor of Cardiology Hofstra University
Cardiac ultrasound protocols
 Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Cardiac ultrasound protocols IDEXX Telemedicine Consultants Two-dimensional and M-mode imaging planes Right parasternal long axis four chamber Obtained from the right side Displays the relative proportions
Stephen Glen ISCHAEMIC HEART DISEASE AND LEFT VENTRICULAR FUNCTION
 Stephen Glen ISCHAEMIC HEART DISEASE AND LEFT VENTRICULAR FUNCTION Overview Coronary arteries Terminology to describe contractility Measuring ventricular function Systolic dysfunction Practice cases- LV
Stephen Glen ISCHAEMIC HEART DISEASE AND LEFT VENTRICULAR FUNCTION Overview Coronary arteries Terminology to describe contractility Measuring ventricular function Systolic dysfunction Practice cases- LV
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care. Dr. Mark Tutschka Dr. Rob ArnAield
 Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
Advanced Applica,on of Point- of- Care Echocardiography in Cri,cal Care Dr. Mark Tutschka Dr. Rob ArnAield OBJECTIVES Provide an overview of common advanced echocardiographic techniques suitable for use
What are the best diagnostic tools to quantify aortic regurgitation?
 What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
What are the best diagnostic tools to quantify aortic regurgitation? Agnès Pasquet, MD, PhD Pôle de Recherche Cardiovasculaire Institut de Recherche Expérimentale et Clinique Université catholique de Louvain
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital
 Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Giovanni Di Salvo MD, PhD, FESC Second University of Naples Monaldi Hospital VSD is one of the most common congenital cardiac abnormalities in the newborn. It can occur as an isolated finding or in combination
Doppler Basic & Hemodynamic Calculations
 Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
Doppler Basic & Hemodynamic Calculations August 19, 2017 Smonporn Boonyaratavej MD Division of Cardiology, Department of Medicine Chulalongkorn University Cardiac Center, King Chulalongkorn Memorial Hospital
ASCeXAM / ReASCE. Practice Board Exam Questions Monday Morning
 ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
ASCeXAM / ReASCE Practice Board Exam Questions Monday Morning Ultrasound Physics Artifacts Doppler Physics Imaging, Knobology, and Artifacts Echocardiographic Evaluation of the RV Tricuspid and Pulmonary
좌심실수축기능평가 Cardiac Function
 Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Basic Echo Review Course 좌심실수축기능평가 Cardiac Function Seonghoon Choi Cardiology Hallym university LV systolic function Systolic function 좌심실수축기능 - 심근의수축으로심실에서혈액을대동맥으로박출하는기능 실제임상에서 LV function 의의미 1Diagnosis
Valvular Heart Disease: Assessment and Timing of Intervention. Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust
 Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
Valvular Heart Disease: Assessment and Timing of Intervention Graham Cole Consultant Cardiologist Imperial College Healthcare NHS Trust Disclosures: Speaker fee: Bayer Acknowledgements: Matt Shun-Shin
DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES
 QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES") THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
THORAXCENTRE DOPPLER HEMODYNAMICS (1) QUANTIFICATION OF PRESSURE GRADIENTS and INTRACARDIAC PRESSURES J. Roelandt DOPPLER HEMODYNAMICS Intracardiac pressures and pressure gradients Volumetric measurement
Echo in Pulmonary HTN
 Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
Echo in Pulmonary HTN Steven A. Goldstein MD FACC FASE Professor of Medicine Georgetown University Medical Center MedStar Heart Institute Washington Hospital Center Monday, October 10, 2017 Pulmonary Artery
RIGHT VENTRICULAR SIZE AND FUNCTION
 RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
RIGHT VENTRICULAR SIZE AND FUNCTION Edwin S. Tucay, MD, FPCC, FPCC, FPSE Philippine Society of Echocardiography Quezon City, Philippines Echo Mission, BRTTH, Legaspi City, July 1-2, 2016 NO DISCLOSURE
Echocardiographic Evaluation of the Cardiomyopathies. Stephanie Coulter, MD, FACC, FASE April, 2016
 Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Echocardiographic Evaluation of the Cardiomyopathies Stephanie Coulter, MD, FACC, FASE April, 2016 Cardiomyopathies (CMP) primary disease intrinsic to cardiac muscle Dilated CMP Hypertrophic CMP Infiltrative
Stress Testing in Valvular Disease
 2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida Orlando, FL October 10, 2017 2:40 2:50 PM 10 min Grand Harbor Ballroom South Stress Testing in Valvular Disease Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
The new Guidelines: Focus on Chronic Heart Failure
 The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
The new Guidelines: Focus on Chronic Heart Failure Petros Nihoyannopoulos MD, FRCP, FESC Professor of Cardiology Imperial College London and National & Kapodistrian University of Athens 2 3 4 The principal
Normal TTE/TEE Examinations
 Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Normal TTE/TEE Examinations Geoffrey A. Rose, MD FACC FASE Sanger Heart & Vascular Institute Before you begin imaging... Obtain the patient s Height Weight BP PLAX View PLAX View Is apex @ 9-10 o clock?
Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM
 The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
The Patient with Aortic Stenosis and Mitral Regurgitation Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM Aortic Stenosis + Mitral Regurgitation?
HEMODYNAMIC ASSESSMENT
 HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
HEMODYNAMIC ASSESSMENT INTRODUCTION Conventionally hemodynamics were obtained by cardiac catheterization. It is possible to determine the same by echocardiography. Methods M-mode & 2D echo alone can provide
Tricuspid and Pulmonary Valve Disease
 Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Tricuspid and Pulmonary Valve Disease Lawrence Rudski MD FRCPC FACC FASE Professor of Medicine Director, Division of Cardiology Jewish General Hospital McGill University Question 1 All of the following
Pulmonary Hypertension. Echocardiography: Pearls & Pitfalls
 Pulmonary Hypertension Echocardiography: Pearls & Pitfalls Αθανάσιος Γ. Κουτσάκης Ειδικευόμενος Καρδιολογίας Α Καρδιολογική Κλινική ΑΠΘ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας Ιωάννινα,
Pulmonary Hypertension Echocardiography: Pearls & Pitfalls Αθανάσιος Γ. Κουτσάκης Ειδικευόμενος Καρδιολογίας Α Καρδιολογική Κλινική ΑΠΘ Σεμινάρια Ομάδων Εργασίας Ελληνικής Καρδιολογικής Εταιρείας Ιωάννινα,
Aortic Regurgitation and Aortic Aneurysm - Epidemiology and Guidelines -
 Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
Reconstruction of the Aortic Valve and Root - A Practical Approach - Aortic Regurgitation and Aortic Aneurysm Wednesday 14 th September - 9.45 Practice must always be founded on sound theory. Leonardo
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD
 COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
COMPREHENSIVE EVALUATION OF FETAL HEART R. GOWDAMARAJAN MD Disclosure No Relevant Financial Relationships with Commercial Interests Fetal Echo: How to do it? Timing of Study -optimally between 22-24 weeks
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Fig.1 Normal appearance of RV in SAX:
 Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Tutorial 7 - Assessment of the right heart Assessment of the Right heart The right heart assessment clinically and echocardiographically is not a very important part of mainstream cardiology. In the ICU,
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Imaging Guide Echocardiography
 Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
Imaging Guide Guide to Small Animal Echocardiography using the Vevo Imaging Systems System Compatibility: This guide contains instructions and suggestions for work on the Vevo2100, VevoLAZR, Vevo 3100
NEW GUIDELINES. A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee
 NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
NEW GUIDELINES A Guideline Protocol for the Assessment of Aortic Regurgitation From the British Society of Echocardiography Education Committee Gill Wharton, Prathap Kanagala (Lead Authors) Richard Steeds
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Choose the grading of diastolic function in 82 yo woman
 Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Question #1 Choose the grading of diastolic function in 82 yo woman E= 80 cm/s A= 70 cm/s LAVI < 34 ml/m 2 1= Grade 1 2= Grade 2 3= Grade 3 4= Normal 5= Indeterminate 2018 MFMER 3712003-1 Choose the grading
Breakout Session: Transesophageal Echocardiography
 Breakout Session: Transesophageal Echocardiography Doris Ockert, MD Andrew Schroeder, MD University of Wisconsin School of Medicine and Public Health Jutta Novalija, MD, PhD Medical College of Wisconsin
Breakout Session: Transesophageal Echocardiography Doris Ockert, MD Andrew Schroeder, MD University of Wisconsin School of Medicine and Public Health Jutta Novalija, MD, PhD Medical College of Wisconsin
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM. General Instructions: ID NUMBER: FORM NAME: H F A DATE: 10/13/2017 VERSION: CONTACT YEAR NUMBER:
 ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
ARIC HEART FAILURE HOSPITAL RECORD ABSTRACTION FORM General Instructions: The Heart Failure Hospital Record Abstraction Form is completed for all heart failure-eligible cohort hospitalizations. Refer to
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery
 Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
Aortic Stenosis and Perioperative Risk With Non-cardiac Surgery Aortic stenosis (AS) is characterized as a high-risk index for cardiac complications during non-cardiac surgery. A critical analysis of old
ECHO HAWAII. My home. Pulmonary Hypertension and Pulmonary Embolism: Role of Echo U.S.A. Japan. Hawaii Island 1/9/2018
 Pulmonary Hypertension and Pulmonary Embolism: Role of Echo ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan My home Japan U.S.A Hawaii Island 1 Economy
Pulmonary Hypertension and Pulmonary Embolism: Role of Echo ECHO HAWAII January 15 19, 2018 Kenya Kusunose, MD, PhD, FASE Tokushima University Hospital Japan My home Japan U.S.A Hawaii Island 1 Economy
TAVR: Echo Measurements Pre, Post And Intra Procedure
 2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
2017 ASE Florida, Orlando, FL October 10, 2017 8:00 8:25 AM 25 min TAVR: Echo Measurements Pre, Post And Intra Procedure Muhamed Sarić MD, PhD, MPA Director of Noninvasive Cardiology Echo Lab Associate
5 Working With Measurements
 5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
5 Working With Measurements Measurement Overview Measurements accompanying ultrasound images supplement other clinical procedures available to the attending physician. Accuracy of the measurements is determined
Copyright 2017 American College of Emergency Physicians. All rights reserved.
 POLICY Approved April 2017 Guidelines for the Use of Transesophageal Echocardiography (TEE) in the ED for Cardiac Arrest Approved by the ACEP Board of Directors April 2017 1. Introduction The American
POLICY Approved April 2017 Guidelines for the Use of Transesophageal Echocardiography (TEE) in the ED for Cardiac Arrest Approved by the ACEP Board of Directors April 2017 1. Introduction The American
Value of echocardiography in chronic dyspnea
 Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
Value of echocardiography in chronic dyspnea Jahrestagung Schweizerische Gesellschaft für /Schweizerische Gesellschaft für Pneumologie B. Kaufmann 16.06.2016 Chronic dyspnea Shortness of breath lasting
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
The background of the Cardiac Sonographer Network News masthead is a diagnostic image:
 Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Number 5 Welcome Number 5 Welcome to the newsletter created just for you: sonographers who perform pediatric echocardiograms in primarily adult echo labs. Each issue features tips on echocardiography of
Echo in Heart Failure
 Echo in Heart Failure Karima Addetia, MD Heart Failure: Definition A clinical syndrome that results from impairment of ventricular filling or ejection of blood. Manifestations include dyspnea and fatigue,
Echo in Heart Failure Karima Addetia, MD Heart Failure: Definition A clinical syndrome that results from impairment of ventricular filling or ejection of blood. Manifestations include dyspnea and fatigue,
B-Mode measurements protocols:
 Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Application Note How to Perform the Most Commonly Used Measurements from the Cardiac Measurements Package associated with Calculations of Cardiac Function using the Vevo Lab Objective The Vevo LAB offline
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation.
 Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
Evaluation of the Right Ventricle in Candidates for Right Ventricular Assist Device Implantation. Evaluation of RVAD Function. Ioannis A Paraskevaidis Attikon University Hospital Historical Perspective
ICE: Echo Core Lab-CRF
 APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
APPENDIX 1 ICE: Echo Core Lab-CRF Study #: - Pt Initials: 1. Date of study: / / D D M M M Y Y Y Y 2. Type of Study: TTE TEE 3. Quality of Study: Poor Moderate Excellent Ejection Fraction 4. Ejection Fraction
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Comprehensive Echo Assessment of Aortic Stenosis
 Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Comprehensive Echo Assessment of Aortic Stenosis Smonporn Boonyaratavej, MD, MSc King Chulalongkorn Memorial Hospital Bangkok, Thailand Management of Valvular AS Medical and interventional approaches to
Vevo 2100 System Cardio Measurements. Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc.
 Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
Vevo 2100 System Cardio Measurements Dieter Fuchs, PhD FUJIFILM VisualSonics, Inc. dfuchs@visualsonics.com Instructions This document is a guideline on how to assess cardiac function in rodents imaged
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Data Collected: June 17, Reported: June 30, Survey Dates 05/24/ /07/2010
 Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
Job Task Analysis for ARDMS Pediatric Echocardiography Data Collected: June 17, 2010 Reported: Analysis Summary For: Pediatric Echocardiography Exam Survey Dates 05/24/2010-06/07/2010 Invited Respondents
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision
 A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
A Surgeon s Perspective Guidelines for the Management of Patients with Valvular Heart Disease Adapted from the 2006 ACC/AHA Guideline Revision Prof. Pino Fundarò, MD Niguarda Hospital Milan, Italy Introduction
Echo Assessment Pre-TAVI
 Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial Interest /arrangement or affiliation with the organization(s) listed below Echocardiographic
Echocardiography for the Electrophysiologist: Day-to-day practice. Emmanuel Fares, MD
 Echocardiography for the Electrophysiologist: Day-to-day practice Emmanuel Fares, MD EP and pacing service, Department of Cardiovascular Medicine, Cairo University Agenda Role of echo in arrhythmia management:
Echocardiography for the Electrophysiologist: Day-to-day practice Emmanuel Fares, MD EP and pacing service, Department of Cardiovascular Medicine, Cairo University Agenda Role of echo in arrhythmia management:
Top 10 Facts in Contrast Echocardiography. Pamela R. Burgess, BS, RDCS, RDMS, RVT, FASE
 Top 10 Facts in Contrast Echocardiography Pamela R. Burgess, BS, RDCS, RDMS, RVT, FASE Presenter Disclosure The following relationship exist related to this presentation: Pamela R. Burgess, BS, RDCS, RDMS,
Top 10 Facts in Contrast Echocardiography Pamela R. Burgess, BS, RDCS, RDMS, RVT, FASE Presenter Disclosure The following relationship exist related to this presentation: Pamela R. Burgess, BS, RDCS, RDMS,
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Doppler-echocardiographic findings in a patient with persisting right ventricular sinusoids
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 1990 Doppler-echocardiographic findings in a patient with persisting right
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors
 Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Quantification of Mitral Stenosis: Planimetry, pressure Half time, Continuity Common Errors Christopher J Kramer RDCS Advanced Cardiovascular Services Aurora Health Care Milwaukee, WI No Disclosures Baumgartner,
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency
 Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Uncommon Doppler Echocardiographic Findings of Severe Pulmonic Insufficiency Rahul R. Jhaveri, MD, Muhamed Saric, MD, PhD, FASE, and Itzhak Kronzon, MD, FASE, New York, New York Background: Two-dimensional
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function. Irmina Gradus-Pizlo, MD
 Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function Irmina Gradus-Pizlo, MD Disclosures: Nothing to disclose Overview Is pulmonary hypertension
Pulmonary Hypertension: Echocardiographic Evaluation of Pulmonary Hypertension and Right Ventricular Function Irmina Gradus-Pizlo, MD Disclosures: Nothing to disclose Overview Is pulmonary hypertension
Cardiac Magnetic Resonance in pregnant women
 Cardiac Magnetic Resonance in pregnant women Chen SSM, Leeton L, Dennis AT Royal Women s Hospital and The University of Melbourne, Parkville, Australia alicia.dennis@thewomens.org.au Quantification of
Cardiac Magnetic Resonance in pregnant women Chen SSM, Leeton L, Dennis AT Royal Women s Hospital and The University of Melbourne, Parkville, Australia alicia.dennis@thewomens.org.au Quantification of
MR echo case. N.Koutsogiannis Department of Cardiology University Hospital Of Patras
 MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
MR echo case N.Koutsogiannis Department of Cardiology University Hospital Of Patras Case A 35 years old male came to the echo lab for a third opinion for his valvulopathy. He reports a long standing MR
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
CASE REPORT: DOUBLE ORIFICE MITRAL VALVE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VALVE IN AN AFRO-CARIBBEAN
 CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
CASE REPORT: DOUBLE ORIFICE MITL VAE WITH CLEFT IN ANTERIOR LEAFLET OF DOMINANT VAE IN AN AFRO-CARIBBEAN Disclosure: No potential conflict of interest. Received: 27.08.13 Accepted: 23.06.14 Citation: EMJ
MITRAL REGURGITATION ECHO PARAMETERS TOOL
 Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and
Comprehensive assessment of qualitative and quantitative parameters, along with the use of standardized nomenclature when reporting echocardiographic findings, helps to better define a patient s MR and