Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant
|
|
|
- Derick Reeves
- 5 years ago
- Views:
Transcription


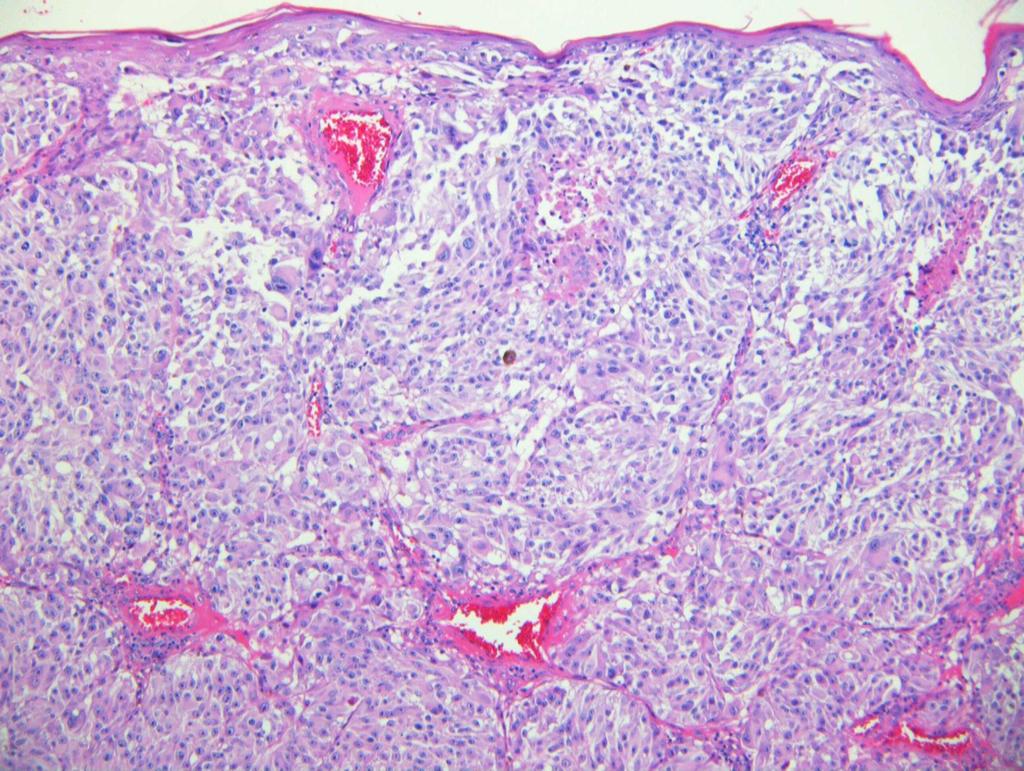
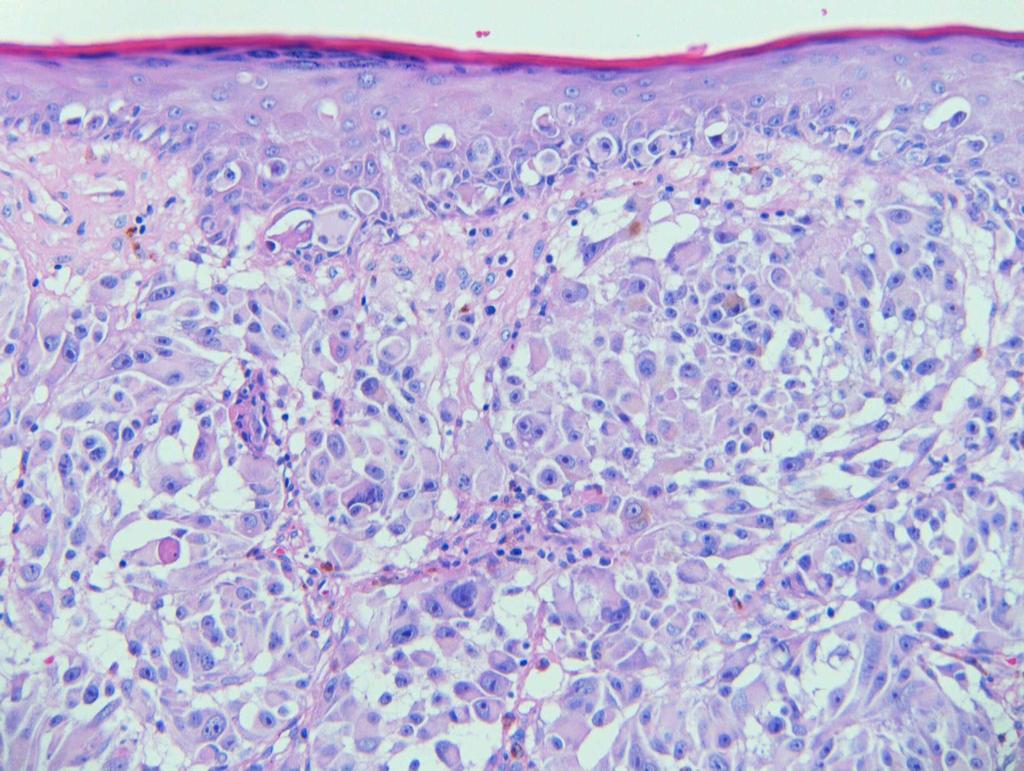
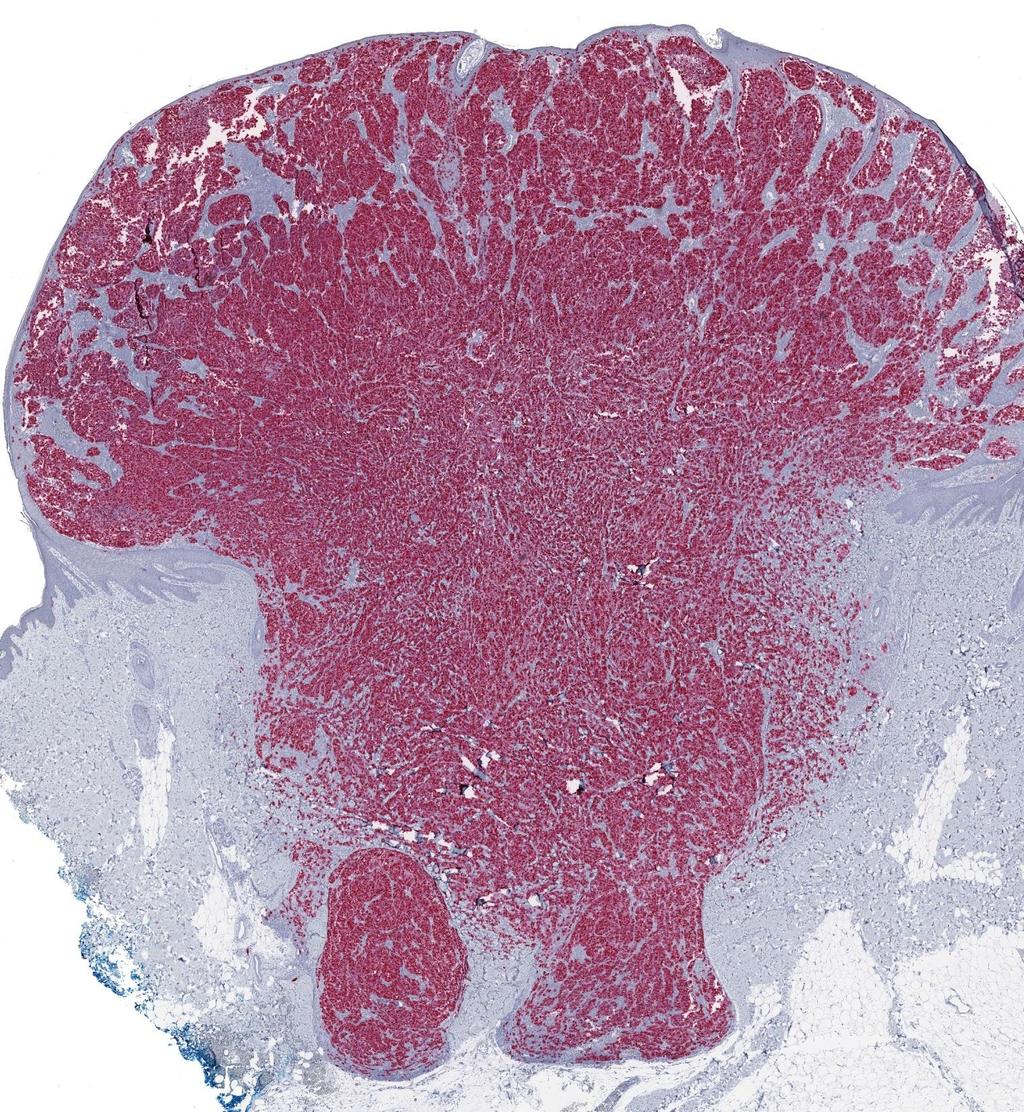
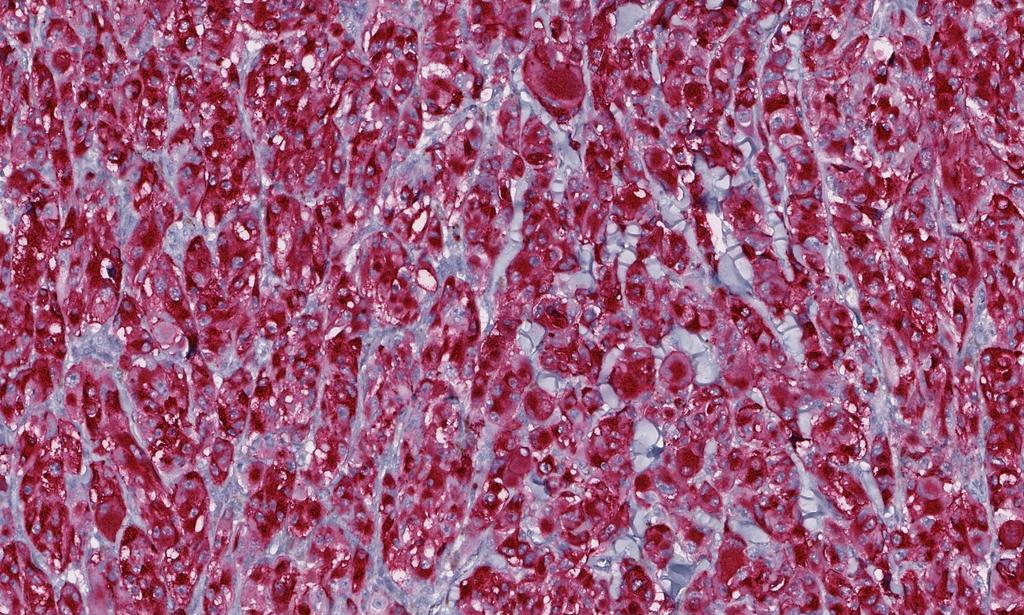
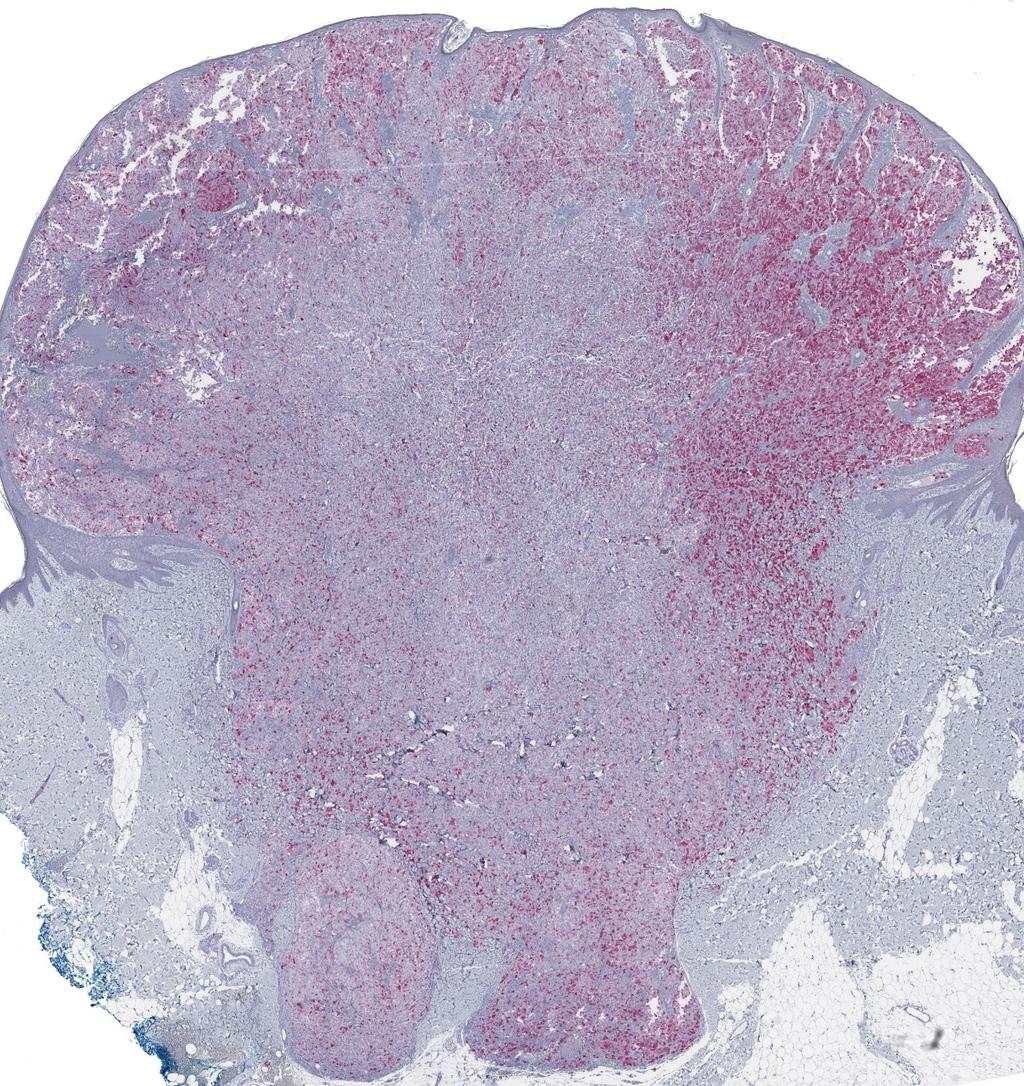
1 Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant Dermoscopy: coarse vascular structures. c/o A, B, C RAC7750

2 Case 231: F7. Exophytic naevus over left trapezious. Grown over a few weeks. Iniitally flat.?spitz naevus,?malignant c/o D RAC7750
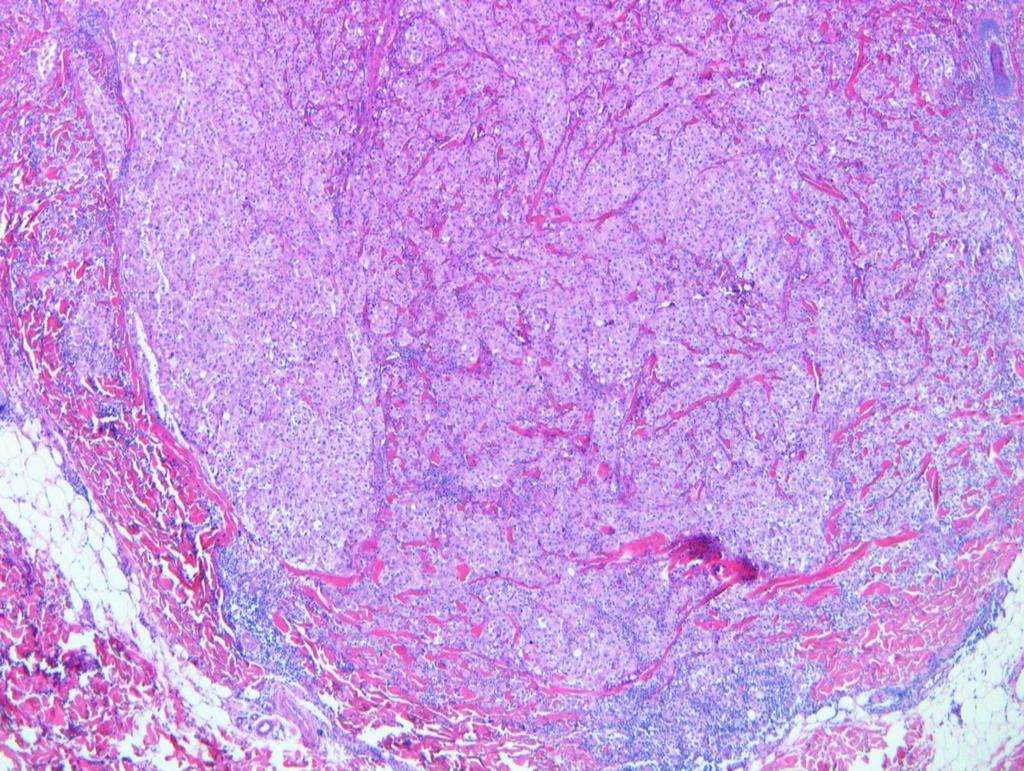
3 Base
4

5 Necrotic foci
6

7 Atypical mitotic figure

8 Deep mitosis
9 Pie Chart Participants N=74
10 Benign: 9 Spitz 30 Uncertain favour benign 16 Uncertain favour malignant 20 Malignant 27 Spitzoid 30 Nodular 8 SSMM 1

11 Table for Malignant Responses
12 MPathDx* *I: Leave as is even if incompletely excised; II: Complete excision <5mm; III: 5mm; IV: as pt1a, pt1b; 1cm +/-; V: as pt2 or greater e.g. >1cm
13 EQA Participants: Benign N=9 Symmetrical with collarette and maturation with depth. No destructive growth. I'd at least be asking a local colleague for a second opinion, though. Almost symmetrical compound lesion with epithelioid cells having promiennt eosinophilic nucleoli and mitotic activity (9mf/10HPF); focal indvidual cells wrapping around dermal collagen; no definite pagetoid spread. Overall spitzoid lesion, favour spitz naevus with atypia (focal ulceration and high mitoses).
14 EQA Participants: Uncertain favour benign N=16 Atypical Spitz tumour - low score (according to Barnhill), uncertain malignant potential. Needs molecular analysis (HRAS mutation or kinase fusion, PTEN, 9p21 deletion, etc); also BRAF, BAP1. I would treat as malignant, but without SLNB. Bapoma? Several. DD with Epithelioid spitz polypoid tumour of large pleomorphic epitheliod naevus cells with big pink nucleoli, some multinucleated. Some mitoses incl deep ones. Vascular network and lymphocytes present? BAPoma Sheets of mitotically active spitzoid cells forming a wedge shaped but expansile dermal nodule. Given age group of patient, I would categorise as atypical Spitz tumour. Need to ensure complete excision (with more sections) and keep under clinical follow up for 5 years. Difficult case. On balance I favour atypical spitz, considering the age of the patient, otherwise could easily be diagnosed as melanoma
15 EQA Participants: Uncertain favour malignant N=20 I am wary of an outright diagnosis of melanoma in this age group, and would prefer to call STUMP (but clearly very worrying), and advise FISH, etc. Atypical Spitz tumour. STUMP. Favour melanoma, but this is a young patient Spitzoid lesion. Young child. Atypia with pleomorphism and deep mitoses. Do not wish to call MM but worrying features therefore classify atypical spitz tumour and manage as MM. SNB questionable. Looks like a Spitzoid melanoma. STUMP at least. Very mitotic, but well circumscribed and age 7. Would request FISH before calling it melanoma BAPOMA?
16 EQA Participants: Malignant N=27 Spitzoid lesion but without maturation and several deep mitoses seen such that despite the patients young age should be regarded as malignant Difficult case but I think on balance this is a Spitzoid malignant melanoma. Pushing deep border and occasional deep mitotic figures. Symetrical but consumption of epidermis, variable pleomorphism, loss of maturation, increased mitotic activity with deep mitoses.


17 N=24 Pie Chart Slide Club *1 STUMP, NOS assigned to Favour Malignant
18 SLIDE CLUB RESPONSES Uncertain favour malignant, Spitzoid Uncertain favour malignant Spitzoid MM.Highly cellular predominantly dermal tumour with barely any intervening stroma, a complete lack of architectural and cytological maturation and several deep mitoses. Nodular severely atypical epithelioid/spitzoid melanocytic tumor; lots of mitoses superficial and deep, no maturation, no definite ulceration, deep dermal bulky growth. I would prefer a classification as high risk Spitzoid tumor/stump, but melanoma not excluded, based on histological findings alone. I would definitely do additional immunostainings and molecular analysis before signing out such a case. It is a young girl. I have seen such cases in young children with favourable outcome, more than 20 years follow-up without recurrences. AST, high risk (Spatz et al) Age is the obvious confounder here, but despite the patient's age, I suspect this is malignant melanoma, nodular type. While the age definitely prompts consideration of a Spitzoid melanoma, I see few genuinely 'Spitzoid' histopathologic features here. Ancillary testing might help with classification. Spitzoid melanoma of childhood with a comment that these tumours may have a favorable outcome and that LNSB is unnecessary. Epithelioid spitz naevus
19 SLIDE CLUB RESPONSES Uncertain favour benign. Requires molecular correlation with FISH. Atypical Spitzoid tumour, deep and atypical mitotic figures but no necrosis. Malignant rare at this age so more likely benign although uncertain malignant potential Spitzoid tumor of uncertain malignant potential. Cannot rule out Spitz melanoma. Would do HMB45, MelanA/Mart, Ki-67 and p16 stains, also BRAF V600E and available usion genes if BRAF negative. CGH could be a useful next step. Will be interested in results of these studies. clearly spitzoid in type. At low power the lesion has a rather dumbell configuration with focal extension into superficial subcutis. The lesion comprises epithelioid and spindle shaped cells in compact aggregates with little intervening stroma. There is uniform and severe nuclear atypia, mitoses at varying levels and also attenuatuion of the epidermis. This lesion is a spitzoid nodular melanoma. 1 st : High-risk atypical Spitz tumor (inflamed, with necrosis) 2 nd : This is an atypical Spitz tumour with high-risk features. Pleomorphic epithelioid cells with inflammation; cells are larger in the depth than close to the surface; there is a group of apoptotic cells (this is a bad sign). Atypical Spitz tumor with extension into the deep dermis. Would order immunostains (Ki67/MelanA, p16, HMB45). The mitotic activity is worrying but could be related to the initial fast growth phase of the tumor. I would recommend to manage this lesion by complete excision with 5-10 mm margin and clinical surveillance.
20 SLIDE CLUB RESPONSES the combination of deep expansive nodules, pleomorphism and mitoses makes the diagnosis of benignity impossible. This even though the evolution will probably be favourable. In my own limited experience only a small fraction of these lesions kills the patient Very spitzoid in nature, but with severe nuclear atypia with irregular large nucleoli deep, plus mitoses and pushing margin all point to uncertain malignant potential [favour malignant] spitzoid nodular melanoma of childhood In view of the large atypical cell type; massiveness of the dermal architecture associated with epidermal consumption ; mitotic activity at all levels), and add a note that, although regional lymph node involvement may well occur (be detected at SN), distant metastasis is relatively unlikely to occur (though can by no means be ruled out). spitzoid MM with atypical mitoses Spitzoid melanoma. I thought also in polypoid Spitz nevus, but neoplastic melanocytes are confluent, there is no maturation and I think that I have seen some mitotic figures in deeper areas (digital); Polypoid melanoma (glass) [Spitzoid, Uncertain favour malignant] No obvious pagetoid spread but the epidermis is considerably thinned and there are intraepidermal melanocytes. The atypia and mitotic activity are too much to simply ascribe to the young age. However, I would recommend genetic analysis and make a final report in the light of the findings.
21 SLIDE CLUB RESPONSES Melanoma, Spitzoid. Young age gives me a low baseline level of suspicion but histology is very worrying high risk atypical Spitzoid tumour and favour a malignant Spitz tumour (normally for a case like this we would do BRAF & NRAS IHC as well as immunochemistry for assessment of proteins associated with various chromosomal fusions including ALK, ROS1, NTRK1&3, MET & RET, p16 and FISH) (glass) Spitz Tumour of uncertain malignant potential (STUMP) High risk Spitz tumour with numerous mitoses and extends focally into subcutis. Could consider ABBOTT probe set and p16/c-myc or acgh but advise wide local excision. [Spitzoid, Uncertain favour malignant] Exophytic, symmetric prolieration of spitzoid melanocytes extending into the reticular dermis. Lesional melanocytes show prominent nucleoli and pleomorphism. There is associated inflammation. Worrisome features include signficnt mitotic rate of dermal melanocytes and melanocytes with pyknotic nuclei. Little maturation. However, given the patient's young age and history of recent growth, this could be a Spitz nevus in its growth phase.
22 Additional Studies: IHC HMB45 & S100 strong, diffuse p16 widespread loss Ki67: lack of maturation, high superficial & deeper areas ALK1 negative
23 HMB45
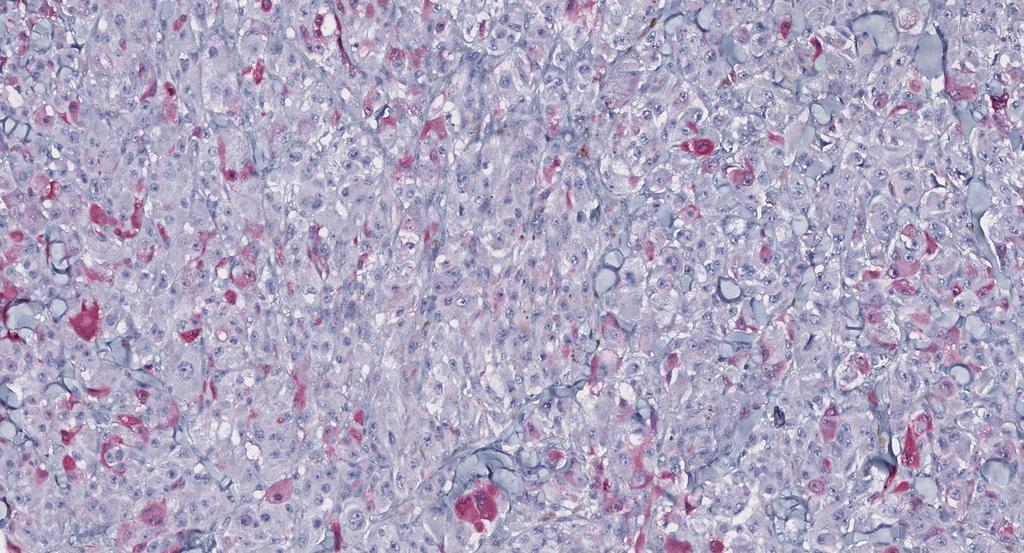
24 p16


25 Ki67 Ki67: lack of maturation, high in superficial & deeper areas
26 MICRO REPORT: Case 231 Nov17 AST, high risk features Absent Kamino bodies Pleomorphic, large epithelioid melanocytes Expansile growth, little intervening stroma Extending deep, into the subcutaneous fat with a focal pushing deep margin. Foci of tumour cell necrosis Mitotic activity was moderately high at 8/mm 2 Atypical mitotic figures


27 Dec 17: At post-operative review, a palpable ipsilateral supraclavicular lymph node was noted. A CT PET confirmed an enlarged 10mm markedly FDG avid lymph node that was highly metabolically active and suspicious for metastasis
 lymph node deposit")

28 c/o A: Lymph node 1.6cm diameter, grossly involved Dear Y, This girl has now come up with a gross (palpated) lymph node deposit 1.6cm in the neck. Question is whether at this age she should undergo a full neck dissection. I d be tempted to say not if it was my daughter but obviously you might have a view with the results of CGH still pending. She s actually provisionally booked for a neck dissection next Monday. Kind regards, X
29 Initial cytogenetic tests, namely comparative genomic hybridisation showed multiple segmental gains and losses on chromosomes 1, 6, 9, 10, 11 and 17. DLRS = 0,20
30 [Y]: Preliminary RNA sequencing data revealed mutations in PIK3CA p.5733f (c.2318c>t), MTOR p.a2416v (c.7247 C>T) and 3 different mutations on the BRCA 1 gene. A new analysis we have identified an exon 2 G12S mutation in KRAS in this child. There are very few data on KRAS mutated melanocytic tumors to my knowledge. (But I am working on this topic ) It is not very good news on the therapeutic options if they were needed in the future.
31 Discussion with the adult specialist skin cancer MDT (SSMDT) highlighted the difficulty in predicting malignant potential from the clinical, biological and molecular features. Detailed further discussion with the general paediatricians, paediatric head and neck and plastic surgeons resulted in the difficult decision to recommend a therapeutic level 1-3 partial neck dissection in view of the number of severely atypical histopathological and molecular features with lymph node involvement, which suggested a less indolent course despite the age of the patient. Following the radical neck dissection, 56/56 lymph nodes were subsequently negative. The patient made an excellent postoperative recovery, with minor wound infection and mild lymphoedema of the ipsilateral jaw post-operatively only.
32 Discussion: Slide Club Responses Clearly age led a significant proportion of EQA responders to favour benign diagnosis despite worriesome histology Bapoma mentioned by some participants Slide Club Panel: More decisively away from benign/favour benign (<20%) Spitzoid : How can we define today? Spatz et al: Unfortunately grading AST is based on a now quite old paper with relatively few cases and little molecular work-up
33 GENERAL DISCUSSION POINTS This rare case of a paediatric spitzoid melanoma with lymph node involvement highlights the challenges in the clinical, histopathological and molecular diagnosis of atypical spitzoid lesions. Molecular studies can play a key role in the diagnosis of spitzoid melanomas in paediatric patients. KRAS exon 2 mutations, as found in our patient have been rarely described in melanomas to date. In the Cancer Genome Atlas database only 0.9% (6/666) of melanomas displayed a KRAS mutation. G12D mutation was the most frequently found (3/6). Management of atypical spitzoid tumours is variable, with a lack of evidence of prognostic benefit for sentinel lymph node biopsy over wide local excision and regular clinical follow-up (ref). Managing rare paediatric spitzoid lesions within an adult SSMDT is less than ideal / remains a challenge and may impact on the provision of optimal holistic and developmentally appropriate care. Provision of a paediatric-specific SSMDT at a regional or national level may help tailor potentially radical treatment decisions in this group of patients.

34 Melanomas of childhood. Am J Pathol. 1948;24: Sophie Spitz Differentiation histologically between juvenile and adult melanoma could not be made with certainty in most cases



35 Spatz A, Calonje E, Handfield-Jones S, Barnhill RL. Spitz tumors in children: a grading system for risk stratification.arch Dermatol Mar;135(3): Alan Spatz University of McGill Canada Eduardo Calonje St John s Institute UK Raymond Barnhill Institut Curie Paris, France


36 ATYPICAL SPTIZ TUMOUR (AST) SPITZ TUMOUR OF UNCERTAIN MALIGNANT POTENTIAL (STUMP) GRADING for childhood cases May promote better reproducibility for diagnosis between observers Should be born in mind that not all cases of metastasis (especially loco-regional nodes) indicate a long-term adverse outcome But even lesions in low risk category may result in death from metastatic disease Needs validation in a larger dataset

37 SPITZ NAEVUS v ATYPICAL SPTIZ TUMOUR (STUMP) Spatz A, Calonje E, Handfield-Jones S, Barnhill RL. Spitz tumors in children: a grading system for risk stratification.arch Dermatol Mar;135(3):333-5.
38 ...currently no IHC or Molecular that can be used to make an entirely safe diagnosis of Spitz nevus or melanoma in problematic cases. 40% 15y or younger H&N commoner location in children c/w adults Compouned (46%); Junctional (33%); Dermal (21%) Epithelioid and/or spindle cells: 100% Maturation: 72% Inflammation: 70% (rarely dense) Epidermal hyperpalsia: 66% Melanin: 50% Telangiectases: 40% Kamino bodies: 34% Desmoplastic stroma: 26% Mitosis: 23% Note: Polypoid SN looks decidedly uncommon! Pagetoid: 13% Stromal hyalinisation: 8% Am J Dermatopathol Apr;31(2):

39 Ferrara et al Am J Dermatopathol Jun;32(4): Reed / PSCN is recognisable clincally & dermascopically The commonest variant of Spitz naevus in one large series Clinical view of a heavily pigmented asymmetric plaque located on the left arm of a 33-year-old man. B, Dermoscopically, the lesion exhibits a starburst pattern typified by pigmented streaks distributed at the periphery in a regular fashion. Despite the shape, asymmetry, distribution of color, and structure are rather homogenous in dermoscopy. C, Histopathologically, the lesion is slightly raised and sharply circumscribed (hematoxylin eosin 340); D, there is a moderate epidermal hyperplasia with hypergranulosis and a prevailingly nested junctional proliferation of spindle and epithelioid melanocytes (hematoxylin eosin 3250). The overall histopathologic features are quite in between a PSCSN and a RN.
 Ferrara et al Am J Dermatopathol. 2010 Jun;32(4):410-4.")
40 pink-red papulonodular lesions, previously considered classical Spitz nevus, could be histopathologically atypical with a great probability than tanblack macules & plaques of PSCSN/RN The previously typical clinical lesions associated with Spitz naevus are probable not infrequently AST (a tumour of intermediate or borderline malignancy) Ferrara et al Am J Dermatopathol Jun;32(4): A, Clinical view of a pink nodule located on the right arm of an 11-year-old girl. B, At a first dermoscopic examination, the lesion exhibits a few red to black hemorrhagic globules over a pink background. C, The second dermoscopic view refers to the same lesion after 15 days when the planned excision was finally performed. The hemorrhagic globules are no more appreciated, and the lesion shows a tan pigmentation at the periphery with a few irregular vessels in the amelanotic central portion. D, Histopathologically, the lesion is nodular and asymmetric (hematoxylin eosin 340); E, despite the absence of any pagetoid spread, there is atrophy of the epidermis, together with some irregular architecture of the dermal nests, which are notably larger in the depth than close to the surface (hematoxylin eosin 3100). The lesion was 4.48 mm in thickness: a sentinel node biopsy showed isolated tumor cells within the subcapsular sinus.
 Mitoses 8/18 (atypical & clustered in 4) Absent maturation 9/18 Absent zonation 8/18 SUBTYPES Genuine (7) Uniform (5) Packed (5) Polypoid (3)")
41 18 cases Mean age 35.2 (15 to 56) Mean size 7.27mm Mean Breslow 2.51 High cell density 10/18 Atypia 9/18 (marked in 1) Mitoses 8/18 (atypical & clustered in 4) Absent maturation 9/18 Absent zonation 8/18 SUBTYPES Genuine (7) Uniform (5) Packed (5) Polypoid (3) Pigmented (2) BEST PARAMETERS: cell density, mitosis, zonation, infiltration pattern, consumption of epidermis Requena et al Am J Dermatopathol Jul;34(5): mitoses in Spitz nevus are scarce, typically in the superficial areas of the neoplasm. We consider this criterion very important in the differential diagnosis of Spitz nevus and spitzoid melanoma; thus, the presence of mitoses in the lower portion or many grouped in an area of a spitzoid lesion must be considered highly indicative of melanoma
42 Last follow-up: slight keloid scar at the site of her original surgery and the worrisome moment in April time when she presented with a changing melanocytic lesion on her parietal scalp which we excised and was shown to be a benign melanocytic naevus she has full mobility and dances and acts and is doing fantastically. She has slight swelling on the side of the surgery but not significant lymphoedema. Acknowledgements: All EQA and Slide Club responders Dr Ina Nicklaus Dr Bella Ganatra Dr Emma Howard Dr Claire Bowen Dr Arnaud de la Fouchardiere
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783
 Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783 Pie Chart Participants N=74 Benign: 48 N=74 Blue naevus: 38 Intradermal: 12 DPN: 10 Compound 3 Clonal: 3; Spitz 2; Special Site: 1; Congenital:
Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783 Pie Chart Participants N=74 Benign: 48 N=74 Blue naevus: 38 Intradermal: 12 DPN: 10 Compound 3 Clonal: 3; Spitz 2; Special Site: 1; Congenital:
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
10/2/17. MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often Borderline) Melanocytic Tumors. An Introduction to SNP Arrays
 Melanocytic Tumors. An Introduction to SNP Arrays") MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the
 Histopathology (4x) shows a domed papule with melanocytes extending into the") Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Guy Perrot (Ги Перро)
") НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Self assessment case. Dr Saleem Taibjee Dorset County Hospital, Dorchester
 Self assessment case Dr Saleem Taibjee saleemtaibjee@gmail.com Dorset County Hospital, Dorchester Clinical details 34-year-old man: Shave excision Skin tag / papilloma left thigh The best diagnosis is:
Self assessment case Dr Saleem Taibjee saleemtaibjee@gmail.com Dorset County Hospital, Dorchester Clinical details 34-year-old man: Shave excision Skin tag / papilloma left thigh The best diagnosis is:
1/10/2018. Soft Tissue Tumors Showing Melanocytic Differentiation. Overview. Desmoplastic/ Spindle Cell Melanoma
 2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
2016 MFMER slide-1 2016 MFMER slide-2 2016 MFMER slide-3 Soft Tissue Tumors Showing Melanocytic Differentiation Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester,
21/07/2017. Hobnail endothelial cells are not the same as epithelioid endothelial cells
 UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
UPDATE IN CUTANEOUS VASCULAR S DERMATOPATHOLOGY SESSION BELFAST PATHOLOGY JUNE 21/2017 Dr E Calonje St John s Institute of Dermatology, London, United Kingdom THE FAMILY OF VASCULAR S WITH EPITHELIOID
Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing *
 DERMATOPATHOLOGY 91 Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing * Gustavo Costa Verardino 1 Mayra Carrijo Rochael 1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20153310
DERMATOPATHOLOGY 91 Spitz nevi in the classic histopathological pattern - lamb in wolf`s clothing * Gustavo Costa Verardino 1 Mayra Carrijo Rochael 1 DOI: http://dx.doi.org/10.1590/abd1806-4841.20153310
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
ARTICLE INFO ABSTRACT
 Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Melanocytic Pigmentation: A Single Manifestation of Myriad of Pathologies [PP: 05-09] Dr. Swapna Honwad Department of Oral Pathology dr.swapnahonwad@gmail.com Dr. Elsy P. Simon Department of Endodontics
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Diagnostic problems in uterine smooth muscle tumors
 Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Diagnostic problems in uterine smooth muscle tumors Marina Kos Ljudevit Jurak Clinical Department of Pathology, Clinical Hospital Center Sestre milosrdnice, Zagreb Institute of Pathology, University of
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Malignant Peripheral Nerve Sheath Tumor
 C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
C H A P T E R 120 Malignant Peripheral Nerve Sheath Tumor Currently, malignant peripheral nerve sheath tumor (MPNST) is the most commonly used generic name for the neoplasms known in the past as neurosarcoma,
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Basics in Dermoscopy
 Basics in Dermoscopy Manal Bosseila Professor of Dermatology, Cairo University Member of European Academy Dermatology & Venereology EADV Member of International Dermoscopy Society IDS Member of Aesthetic
Basics in Dermoscopy Manal Bosseila Professor of Dermatology, Cairo University Member of European Academy Dermatology & Venereology EADV Member of International Dermoscopy Society IDS Member of Aesthetic
The Pathology of Neoplasia Part II
 The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
Special slide seminar
 Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
Special slide seminar Tomáš Rozkoš The Fingerland Department of Pathology Charles University Medical Faculty and Faculty Hospital in Hradec Králové Czech Republic Case history, 33 years old resistance
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Papillary Lesions of the breast
 Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Papillary Lesions of the breast Emad Rakha Professor of Breast Pathology The University of Nottingham Papillary lesions of the breast are a heterogeneous group of disease, which are characterised by neoplastic
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations
 F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors
 The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
The Relevance of Cytologic Atypia in Cutaneous Neural Tumors Recent Findings - New Developments New Problems Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology Department
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis
 Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Selected Pseudomalignant Soft Tissue Tumors of the Skin and Subcutis Andrew L. Folpe, M.D. Professor of Laboratory Medicine and Pathology Mayo Clinic, Rochester, MN folpe.andrew@mayo.edu 2016 MFMER slide-1
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles
Among the benign intraepithelial melanocytic proliferations, Inflamed Conjunctival Nevi. Histopathological Criteria. Resident Short Reviews
 Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
S everal morphological features are frequently used in the
 1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
Cellular Neurothekeoma
 Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
Cellular Neurothekeoma Scott W Binder, MD Pritzker Professor of Pathology & Dermatology Sr. Vice Chair Director, Pathology Clinical Services Chief, Dermatopathology Geffen/UCLA School of Medicine Clinical
EARLY ONLINE RELEASE
 EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
Update On Lipomatous Tumors: Old Standbys and New Concepts
 Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Update On Lipomatous Tumors: Old Standbys and New Concepts John R. Goldblum, M.D. Chairman, Department of Anatomic Pathology Cleveland Clinic Professor of Pathology Cleveland Clinic Lerner College of Medicine
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Dermatologica Sinica
 DERMATOLOGICA SINICA 30 (2012) 57e61 Contents lists available at SciVerse ScienceDirect Dermatologica Sinica journal homepage: http://www.derm-sinica.com CASE REPORT Pigmented epithelioid melanocytoma:
DERMATOLOGICA SINICA 30 (2012) 57e61 Contents lists available at SciVerse ScienceDirect Dermatologica Sinica journal homepage: http://www.derm-sinica.com CASE REPORT Pigmented epithelioid melanocytoma:
K Blessing, J J H Grant, D S A Sanders, M M Kennedy, A Husain, P Coburn
 J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Less Common Variants of Cutaneous Melanoma
 Less Common Variants of Cutaneous Melanoma Raymond L. Barnhill* 1, G. Peter Sarantopoulos 1, and Kapil Gupta 2 1 Department of Pathology and Laboratory Medicine, University of California, Los Angeles,
Less Common Variants of Cutaneous Melanoma Raymond L. Barnhill* 1, G. Peter Sarantopoulos 1, and Kapil Gupta 2 1 Department of Pathology and Laboratory Medicine, University of California, Los Angeles,
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
04/10/2018. Intraductal Papillary Neoplasms Of Breast INTRADUCTAL PAPILLOMA
 Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Intraductal Papillary Neoplasms Of Breast Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head The University of Texas MD Anderson Cancer Center 25 th Annual Seminar in Pathology Pittsburgh,
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on
 Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
Case: The patient is a 24 year- old female who was found to have multiple mural nodules within the antrum. Solid and cystic components were noted on imaging. There is no significant past medical history.
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of
 Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Tiền liệt tuyến Tiền liệt tuyến Gross appearance of nodular hyperplasia in material obtained from suprapubic prostatectomy. Note the multinodular appearance and the admixture of solid and microcystic areas.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Myxo-inflammatory Fibroblastic sarcoma
 AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
AKA Myxo-inflammatory Fibroblastic sarcoma Acral Myxoinflammatory fibroblastic sarcomaam.j.surg.path1998; 22; 911-924 Inflammatory myxoid tumour of soft parts with bizarre giant cells [Pathol.Res.Pract.
SMOOTH MUSCLE TUMOURS
 SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
SMOOTH MUSCLE TUMOURS NORMAL SMOOTH MUSCLE Cytology Immunohistochemistry Ultrastructure Masson Trichrome Smooth Muscle Ultrastructure Many myofilaments running parallel to the long axis of the smooth
A 25 year old female with a palpable mass in the right lower quadrant of her abdomen
 May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
May 2016 A 25 year old female with a palpable mass in the right lower quadrant of her abdomen Contributed by: Paul Ndekwe, MD, Resident Physician, Indiana University School of Department of Pathology and
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various